
Abstract
Introduction:
Management of impacted maxillary canines is considered to be complex and challenging task by orthodontists due to the varied biomechanical considerations involved.
Objective:
This article describes an effective and efficient treatment modality for de-impaction of bilaterally impacted labial and palatal canines.
Case Report:
A female patient aged 13 years and 5 months presented with the following complaints: absence of tooth numbers 13 and 23, crowding in the upper and lower anterior dental units, and over-retained tooth numbers 53 and 63 with a non-consonant smile arc.
Results:
Arch development was done to create space for tooth numbers 13 and 23, as well as to relieve crowding. The impacted canines were surgically exposed, and guided traction was employed to place them in their ideal position. A class I canine and premolar relation was established. The smile aesthetics were also improved. The result remained stable 12 months after the end of treatment. The improvement can be quantified by the reduction in scores of orthodontic indices measured pretreatment and posttreatment.
Conclusion:
Modifications in continuous arch mechanics can be reliably used in the management of impacted canines and arch development.
Introduction
Tooth impaction has been defined as the infraosseous position of a tooth after the expected time of eruption, 1 or it can be said that the tooth in question has not erupted into the oral cavity beyond its normal time of eruption. The most common tooth that is impacted after the third molars is the maxillary canine.2,3
There also exists a gender predilection, as maxillary canine impaction is twice as common in females as compared to men. The frequency of canine impactions in the maxilla is more than twice that of those observed in the mandible. It is also known that among individuals who have impacted maxillary canines, 8% have bilateral impactions. 4 The maxillary tooth impaction can be either labial or palatal with respect to the position from the dental arch. About one-third of all impacted maxillary canines are labially impacted, while two-thirds are palatal in location.5,6
Labial impactions of the maxillary canines have been ascribed to either the ectopic migration of the canine crown over the root of the lateral incisor or the shifting of the maxillary dental midline causing insufficient space for the canine to erupt. 7 Palatal impactions of the maxillary canine have been ascribed to the guidance theory and/ or genetic theory.8,9
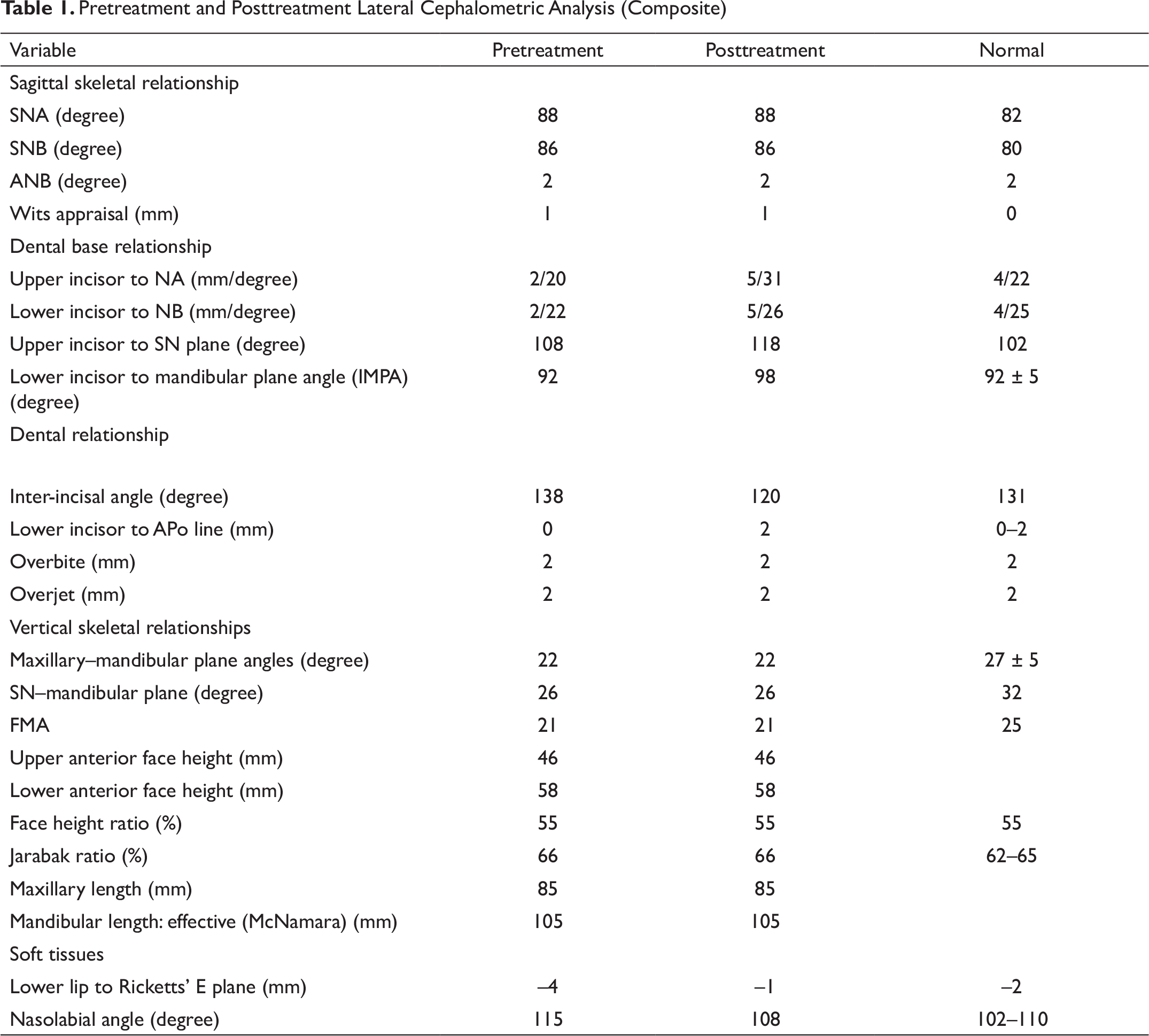
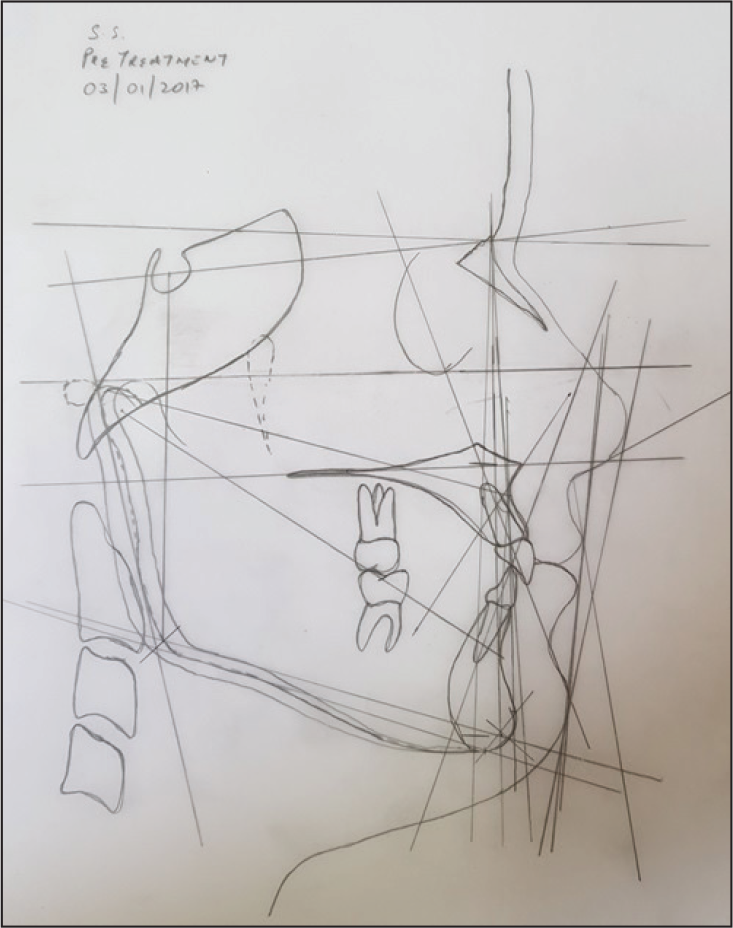
Pretreatment and Posttreatment Lateral Cephalometric Analysis (Composite)
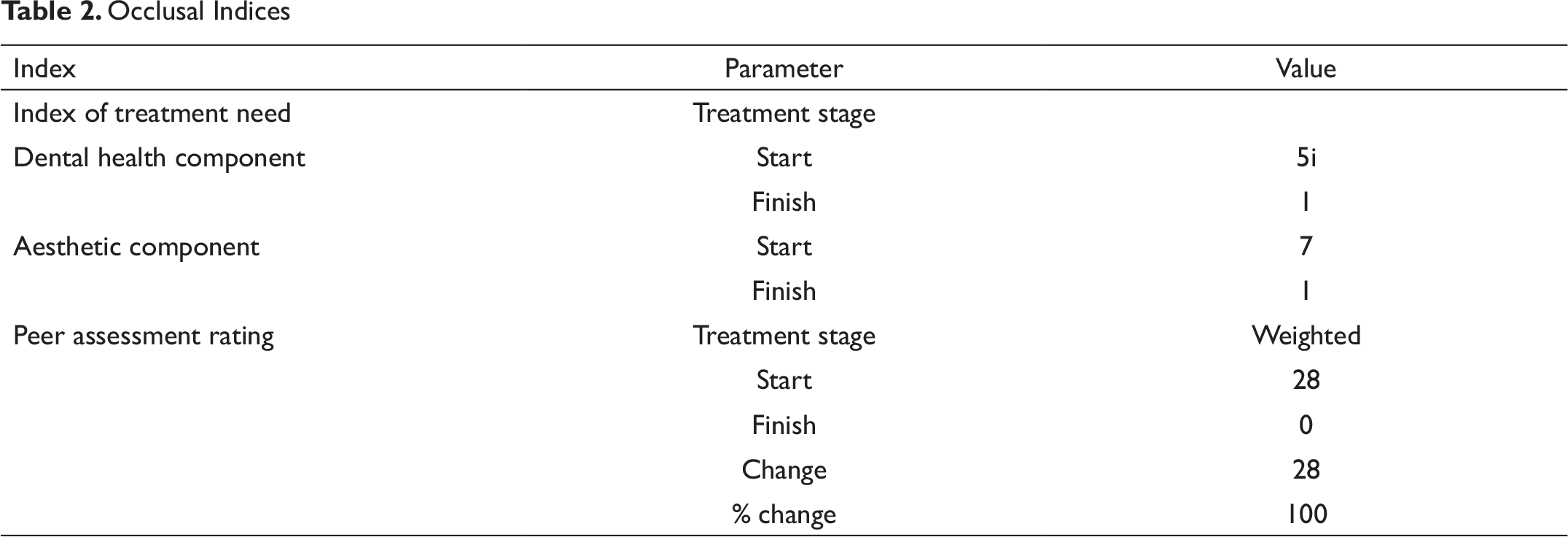
Occlusal Indices
Pretreatment Extraoral View: Frontal at Rest

Pretreatment Extraoral View: Profile

The management of canine impactions can be broadly described in the following key steps: diagnosis and localization of the impacted cuspid(s), arch development or creation of space for the impacted cuspid, surgical exposure involving open or closed surgical techniques,10,11 guided eruption process utilizing a variety of traction techniques,12-14 and detailing the final position of the impacted cuspid to achieve a harmonious relationship with adjacent and opposing dental units.
Management of palatally impacted maxillary canines is technically more challenging given the difficulty in access, complex mechanics, and the greater range of tooth movement as compared to labially impacted canines. 15
This article presents the management of bilaterally impacted maxillary canines (one of which is labial, while the other is palatal) in an adolescent female using a non-extraction technique with a 1-year post treatment review.
Case Report
Section A: Case Evaluation and Development of the Problem List
Pretreatment Evaluation
A girl 13 years and 5 months old, Sh. Sh., reported with a complaint of crooked upper and lower front teeth. There was no contributory medical or dental history.
Pretreatment Extraoral View: Frontal Smiling

Extraoral examination revealed a mesocephalic and mesoprosopic shape of head and facial form, respectively. The facial profile was adjudged to be straight with matched skeletal bases and a normodivergent growth pattern. The lips were incompetent, with a 2 mm interlabial gap at rest. The nasolabial angle was normal, and the mentolabial sulcus was shallow (Figures 1A–1C).
Her smile analysis 16 revealed a non-consonant smile arch with a reverse resting upper lip line and the presence of buccal corridors. Her maxillary midline was not matched with the facial midline, and there was also an asymmetrical dental arch due to vertical discrepancies between incisors. The gingival components of her smile were normal (Figures 2A–2E).
Intraoral examination revealed the presence of all erupted permanent teeth until the second molars, with the absence of both right and left permanent maxillary canines. She also had over-retained right and left deciduous maxillary canines. She had an Angle’s class I molar relationship on both sides. A mild dental deep bite was noted. The arch forms were ovoid for both the maxilla and mandible. The upper and lower dental midlines did not match. She also had rotations in multiple teeth, and a palatal bulge was palpable in the right maxillary region and a labial bulge on the left maxillary quadrant. The gingiva appeared normal. The size and shape of tongue were normal too.
Pretreatment Intraoral View: Frontal

Pretreatment Intraoral View: Left Buccal View

Pretreatment Intraoral View: Right Buccal View

Pretreatment Intraoral View: Maxillary Occlusal View

Pretreatment Intraoral View: Mandibular Occlusal View

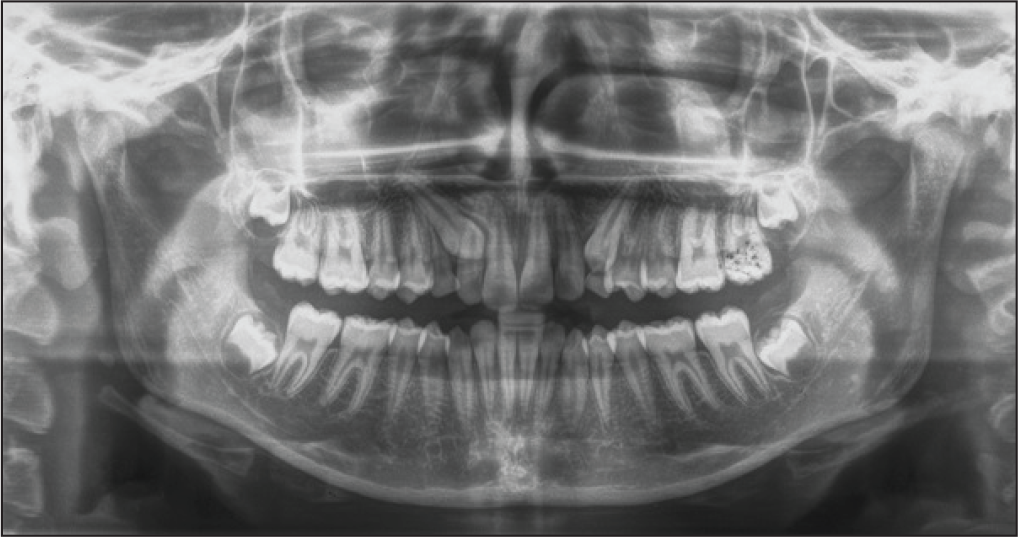
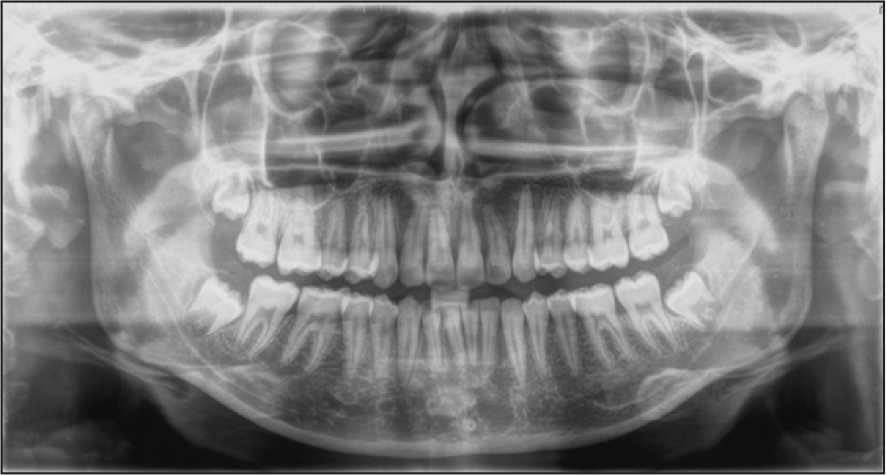
Pretreatment Orthopantomogram
Pretreatment Lateral Cephalogram
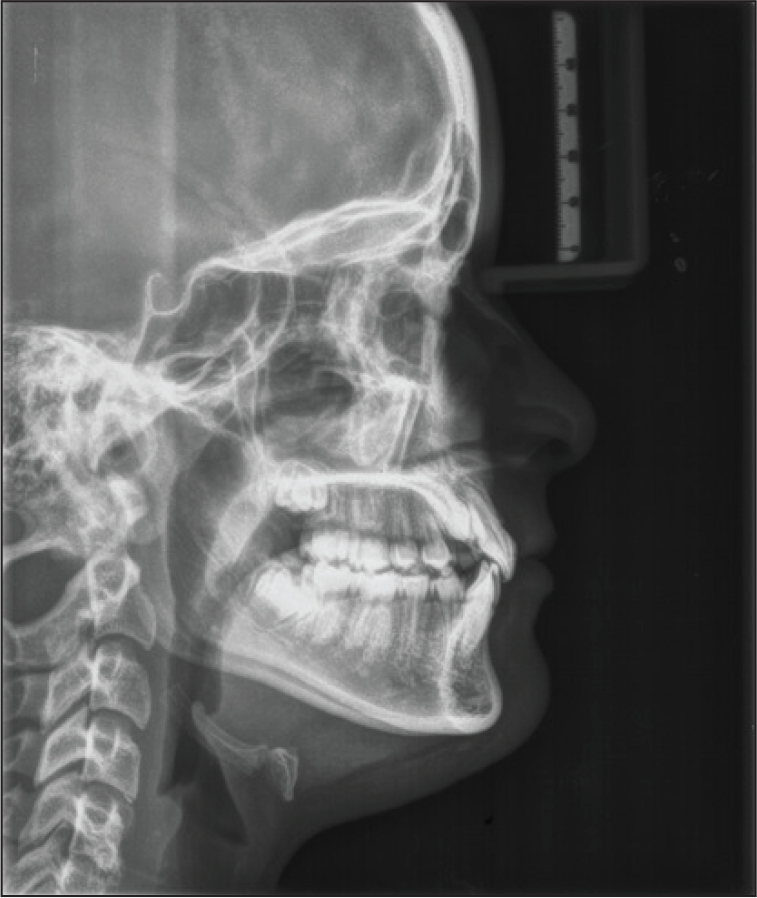
Pretreatment Lateral Cephalometric Analysis
Upon assessing the impacted cuspids for severity using sector classification,17,18 it was seen that tooth number 13 was present in sector IV and was at an angulation of 41°, which was suggestive of a guarded prognosis, while tooth number 23 had a favorable prognosis as it was present in sector I and had an angulation of 27°.
The lateral cephalometric analysis (Figures 4A and 4B; Table 1) revealed a class I pattern (ANB = 2°, beta angle = 30°, Wits appraisal = 1 mm). The sella, nasion, A point (SNA) (88
However, in this case, the SN–maxillary plane angle is 4°. This indicates that the position of the sella is at fault. Because this affects the SNA and SNB values to the same extent, the ANB value does not require correction. To avoid errors associated with discrepancies of the position of the cranial base within the skull, it is advisable to carry out an additional analysis that is independent of this region. This is easily achieved by using the Wits appraisal of jaw disharmony. The Wits appraisal indicates a class I skeletal pattern, which is further corroborated by the beta angle (30°), which is an indicator of sagittal discrepancy. Both these analyses are independent of the sella point and hence show the class I skeletal relation despite a change in the SN plane, if any.
The vertical proportions assessed by the facial height ratio and Jarabak ratio were within the normal range, indicating an average growth pattern. This was also provided credence by an average measurement of the FMA angle (21°).
The upper and lower incisors were also upright over the respective basal bones.
Treatment Objectives
Gain space for maxillary permanent canines (3|3), (tooth numbers 13 and 23) and guide them to their proper position.
Relieve crowding in maxillary and mandibular anterior teeth.
Achieve normal axial inclinations.
Achieve a functional occlusion (class I canine relationship) and a canine-guided occlusion.
Achieve lip competency.
Preserve class I molar occlusion.
Preserve straight profile.
Section B: Treatment
Proposed Treatment Plan
A pre-adjusted edgewise appliance 0.022 in × 0.028 in slot of MBT prescription was employed.
Steps:
Extractions of tooth numbers 53 and 63 were indicated.
Level and align arches.
Alleviate crowding between dental units.
Create space for maxillary permanent canines (3|3).
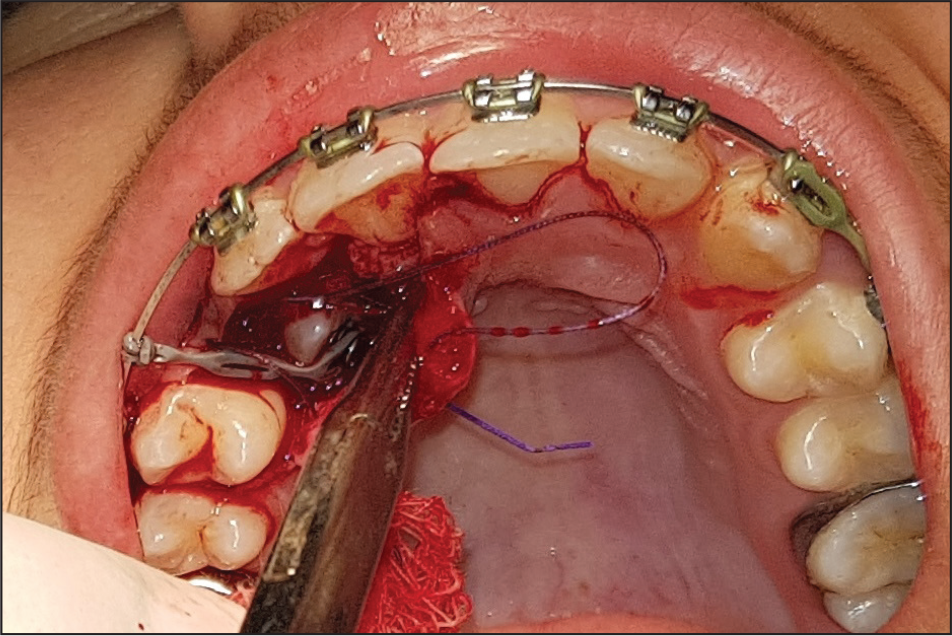
Initiate minor surgical procedures to uncover 13 and 23, bond orthodontic attachments, and apply traction (a, full thickness flap raised for surgical exposure of tooth number 13; b, operculectomy with tooth number 23).
Perform guided eruption with tooth numbers 13 and 23.
Finish and detail the occlusion.
Proposed retention strategy: bonded lingual retainers with tooth numbers 22,21,11,12 and 31,32,41,42 with upper and lower Essix-type clear retainers.
Once tooth number 23 was brought to its occlusal level, surgical exposure of tooth number 13 was performed. A full-thickness mucoperiosteal flap was raised, tooth number 13 was exposed, hemostasis was achieved, and a curved Begg bracket was bonded (Figure 5A). Using a 0.09 in stainless steel ligature wire and elastomeric chain, traction was applied to tooth number 23 to guide its eruption (Figure 5B). Once tooth number 23 was visible in the dental arch, a PAE bracket was bonded onto it and ligated with a 0.012 in copper–nickel–titanium archwire. Brackets were later repositioned while detailing the occlusion. Settling elastics were used to achieve intercuspation in the buccal segments.
After 24 months of active treatment, the fixed appliance was removed and posttreatment records obtained.
Full Thickness Mucoperiosteal Flap Raised to Expose Tooth Number 13

Traction Placed to Guide Eruption of Tooth Number 13
Retention
Bonded lingual retainers with tooth numbers 22,21,11,12 and 31,32,41,42, with upper and lower Essix-type clear retainers, were used. The patient was advised to wear her retainers for 3 years, with a periodic review every 6 months.
No adverse events were recorded during treatment.
Posttreatment Intraoral View: Frontal

Posttreatment Intraoral View: Left Buccal View

Posttreatment Intraoral View: Right Buccal View

Posttreatment Intraoral View: Maxillary Occlusal View

Posttreatment Intraoral View: Mandibular Occlusal View

Results
Posttreatment Assessment
Clinical
The facial profile was straight at the end of the treatment, with proper placement of the impacted cuspids in the dental arch. The crowding of the dental units was also relieved. The smile was improved (Figures 6A–6E). A class I incisor and molar relationship was maintained. The overjet and overbite were both corrected to 2 mm. A class I canine relationship was achieved with a mutually protected function during lateral excursion. Harmonious inter-arch and intra-arch relationships were achieved in the buccal dental units. The maxillary midline was coincident with the facial midline at the end of the treatment. No white spot lesions were seen at the end of the treatment (Figures 7A–7C).
The change in the occlusal indices also reflects the improvement achieved by the orthodontic treatment (Table 2).
Posttreatment Extraoral View: Frontal at Rest
Posttreatment Extraoral View: Profile

Posttreatment Extraoral View: Frontal Smiling

Posttreatment Orthopantomogram
Posttreatment Lateral Cephalogram

Posttreatment Lateral Cephalometric Analysis
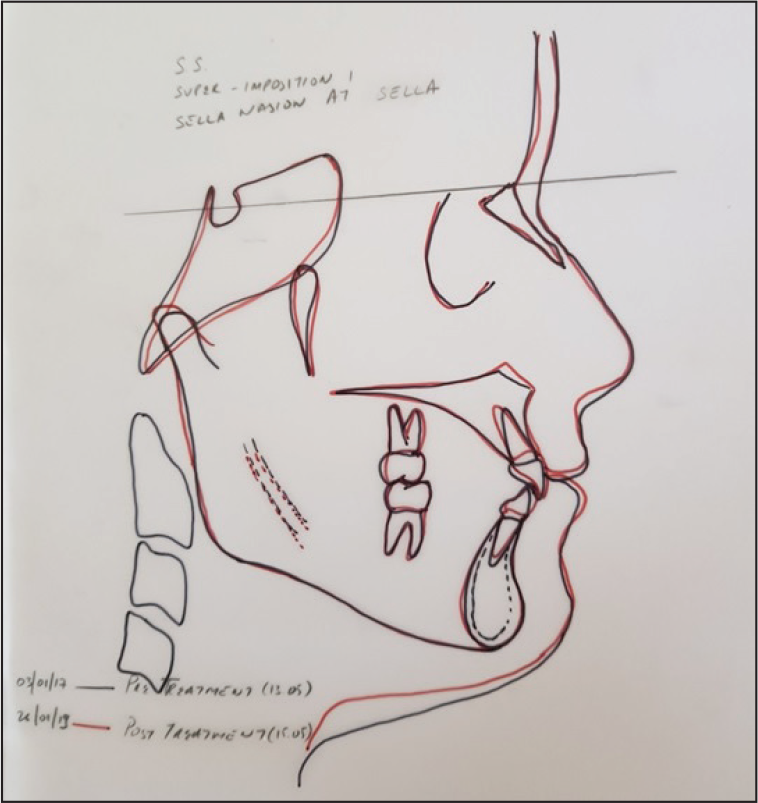
Lateral Cephalometric Superimposition (SN Plane at Sella)
One-Year Recall Extraoral View: Frontal at Rest

One-Year Recall Extraoral View: Profile

One-Year Recall Extraoral View: Frontal Smiling

One-Year Recall Intraoral View: Frontal

One-Year Recall Intraoral View: Left Buccal View

One-Year Recall Intraoral View: Right Buccal View

One-Year Recall Intraoral View: Maxillary Occlusal View

One-Year Recall Intraoral View: Mandibular Occlusal View

Radiographic Appraisal
Discussion
IOTN scores of 5i (dental component) and 7 (aesthetic component) are suggestive of an immediate need for orthodontic treatment. The patient and her parents expressed concerns over irregular upper and lower teeth, as well as poor smile aesthetics.
Since both her maxillary canines were impacted, it was decided to unravel the crowding in the maxillary and mandibular anterior segments while maintaining the posterior buccal occlusion in a class I relationship on both sides. The need for guided eruption (intervention) for an impacted canine was urgent, because of the sequelae of canine impaction. 20 This included root resorption of adjacent teeth, formation of dentigerous cyst around the impacted canine, migration of neighboring teeth, and loss of arch length infection and referred pain. Delayed eruption and the presence of labial and palatal bulges were suggestive of an impacted canine, which was confirmed on reading the radiographs. Also, over-retained deciduous canines are usually shed by the second or third decade of life. This would pose an aesthetic challenge during the patient’s adult life. Further, well-positioned canines are useful in restoring a canine-guided occlusion, which improves chewing efficiency and increases the longevity of the dentition.
On evaluating the patient’s smile aesthetics, it was decided to not remove any permanent teeth in order to preclude dark buccal corridors. This was corroborated by the cephalometric appraisal, which revealed that the upper and lower incisors were retroclined on their respective skeletal bases. Uprighting the incisors would help in creating space to align the crowded dentition, as well as in improving the posture of the lips. Towards the end of the treatment, it could be observed that the patient now has a more “fuller” profile, with upper and lips confirming with the aesthetic line (Ricketts’ E line). The presence of a normal Z angle at the beginning of the treatment also led support to treating this case without extracting any permanent teeth.
To achieve these objectives, a pre-adjusted edgewise appliance (0.022 in × 0.028 in) with an MBT prescription was chosen. For surgical exposure of tooth number 13, it was decided to raise a full-thickness flap in order to visualize the tooth and bond an attachment. This was the procedure of choice, as it helps maintain the gingival architecture around the tooth once it is brought into the arch. With respect to tooth number 23, due to the thin gingival tissue covering it, there was no option of raising a full-thickness flap, as the attachment would have pierced through the gingiva. Hence, it was decided to perform an operculectomy. Care was taken to excise a small amount of gingival tissue over the incisal and middle third of the tooth, thereby preserving the gingiva in the cervical region.
Conclusion
Sh. Sh. was successfully treated with orthodontic treatment and minor adjunctive surgical procedures over a period of 24 months. All treatment objectives envisaged were realized. The patient’s chief complaints were addressed. The patient and her family were pleased with the treatment progress and the results obtained. Aesthetic and occlusal goals as envisaged at the beginning of treatment were met. This is reflected in the decrease in Index of orthodontic treatment needs (IOTN) and peer assessment rating (PAR) scores (Table 2).
Root parallelism between tooth numbers: 31 and 41; and 12 and 13; and More buccal root torque with tooth number 13 required.
Apart from the points mentioned above, all of Andrews’ 6 keys were satisfied posttreatment.
The treatment results were seen to be stable 1 year after the treatment, and the patient has been advised to report for a periodic review every 6 months.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.