
Abstract
Abstract
A 19-year-old dental student reported with a chief complaint of malaligned teeth and an impacted upper right canine (13). On clinical and radiographic examination, he had a slightly depressed maxilla in the upper right region, right deviation of nasal bridge, acceptable facial profile, horizontal, palatally impacted canine whose crown was almost reaching the midline, spaced upper anteriors, excessive gingival display on smile, deep bite, and 34 in crossbite. Comprehensive orthodontic therapy along with surgical exposure of 13 helped in achieving all the treatment objectives to great satisfaction without any adverse effects on the periodontium or the dentition. This case report details the diagnosis and clinical management.
Introduction
The permanent maxillary canines are only second to the third molars in order of dental impactions. Becker and Chaushu 1 stated that while genetics could be attributed as a cause of impacted canines, the path of eruption of the canine is strongly influenced by environmental factors. He classified these factors as local hard tissue obstruction, local pathology, departure from or disturbance of normal development of the incisors, genetic or hereditary factors.
Maxillary canines are important esthetically and functionally, but patients with impacted maxillary canines are perceived to be more difficult and time-consuming to treat than the average orthodontic patient. Should you try to bring the impacted tooth into the arch, expecting that this procedure will add extra time and expense to an average treatment, or should you extract the offending tooth, saving time and money for the patient but perhaps at the expense of esthetics and long-term function?
Stewart et al 2 investigated answers to these questions and concluded that patients with unilateral impaction required, on average, just over 3 months more to treat than control patients with no impaction. The greater the distance the impacted canine was from the occlusal plane, the greater the angulation and more medially displaced it was. The younger the patient at the start of treatment, the longer the duration of orthodontic treatment. When the impacted canine crown was at a distance from the occlusal plane of less than 14 mm, treatment time averaged 23.8 months; a distance of more than 14 mm required an average treatment time of 31.1 months.
Palatally impacted canines can cause, due to their absence in the line of occlusion, a lack of alveolar bone development in the place where it would ideally have been, especially if the deciduous canine has exfoliated early. It then becomes imperative for the orthodontist to factor any gingival concerns, functional and esthetic, in treatment.
This case report details the various aspects of diagnosis and management of a palatally impacted maxillary canine.
Pretreatment Assessment
AD, a 19-year-old male, was a dental student and reported with a chief complaint of malaligned teeth and an impacted canine. There was no other relevant medical history related to the canine impaction.
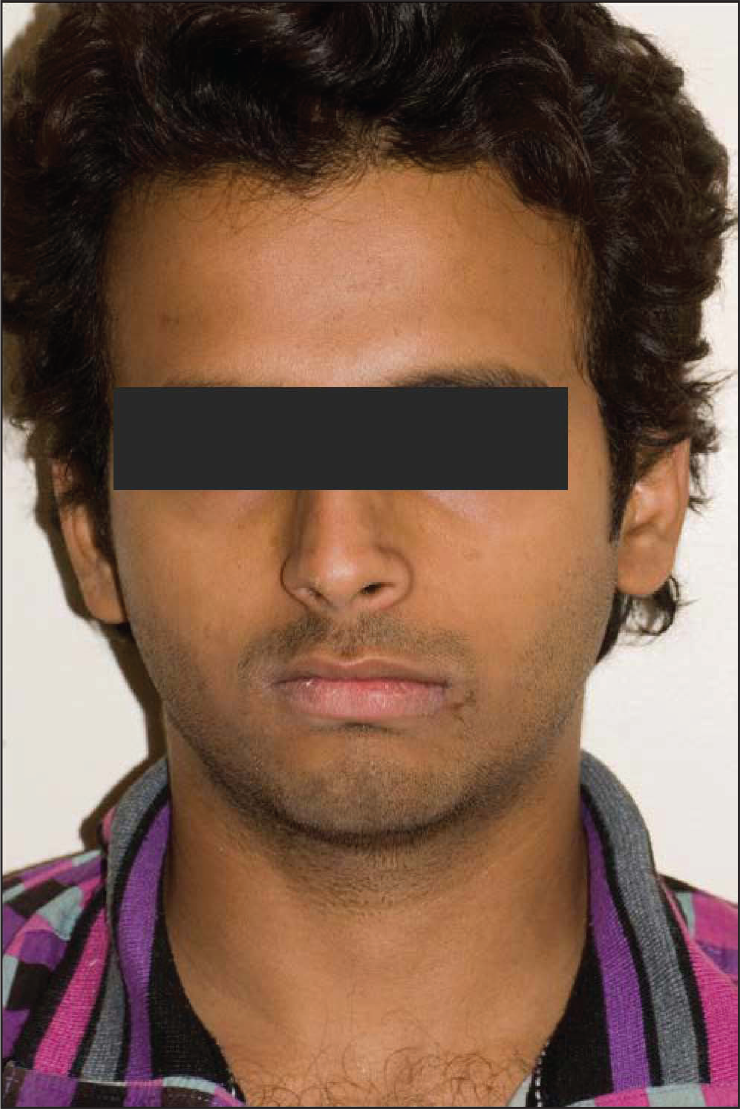
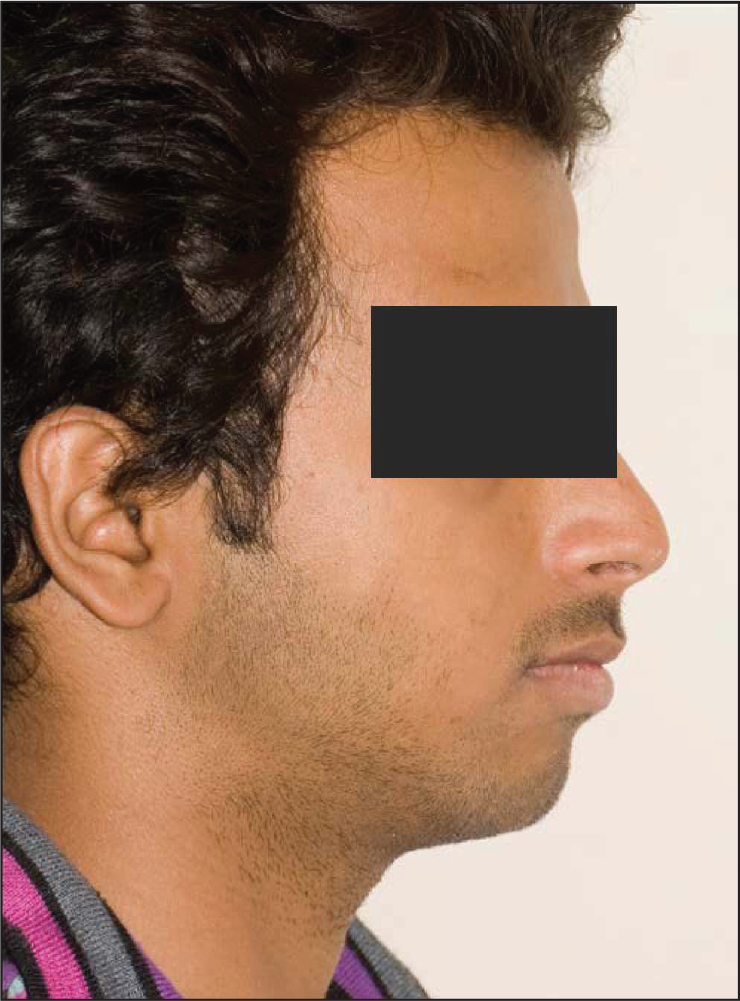
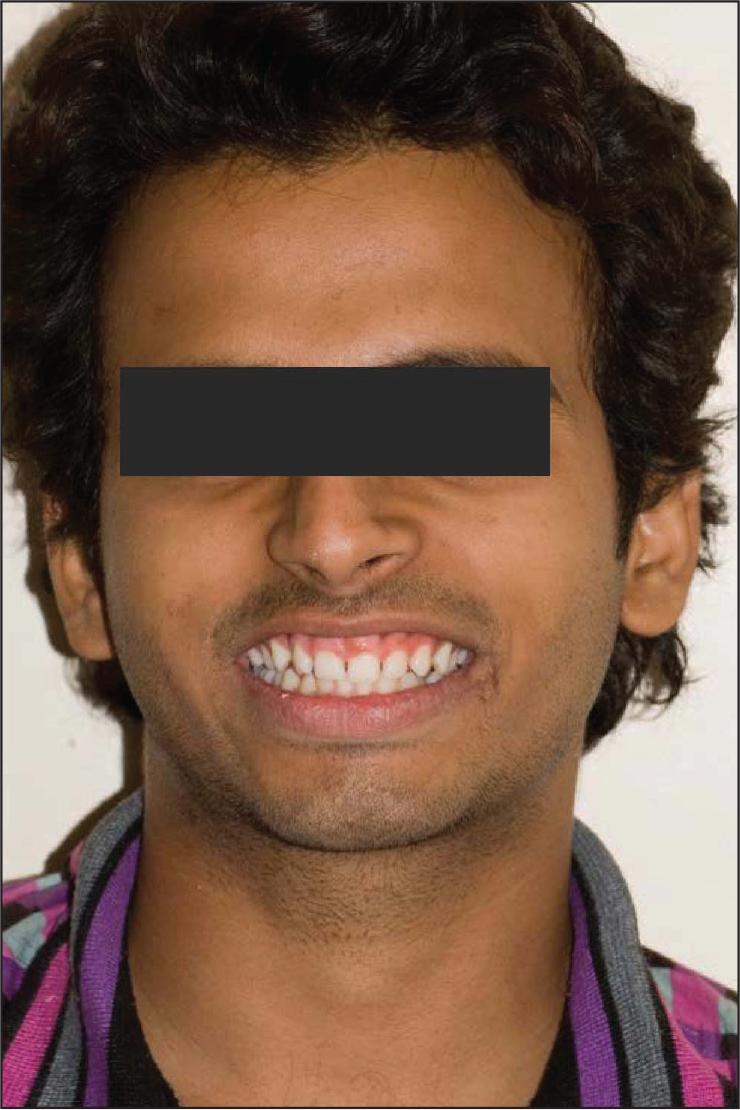
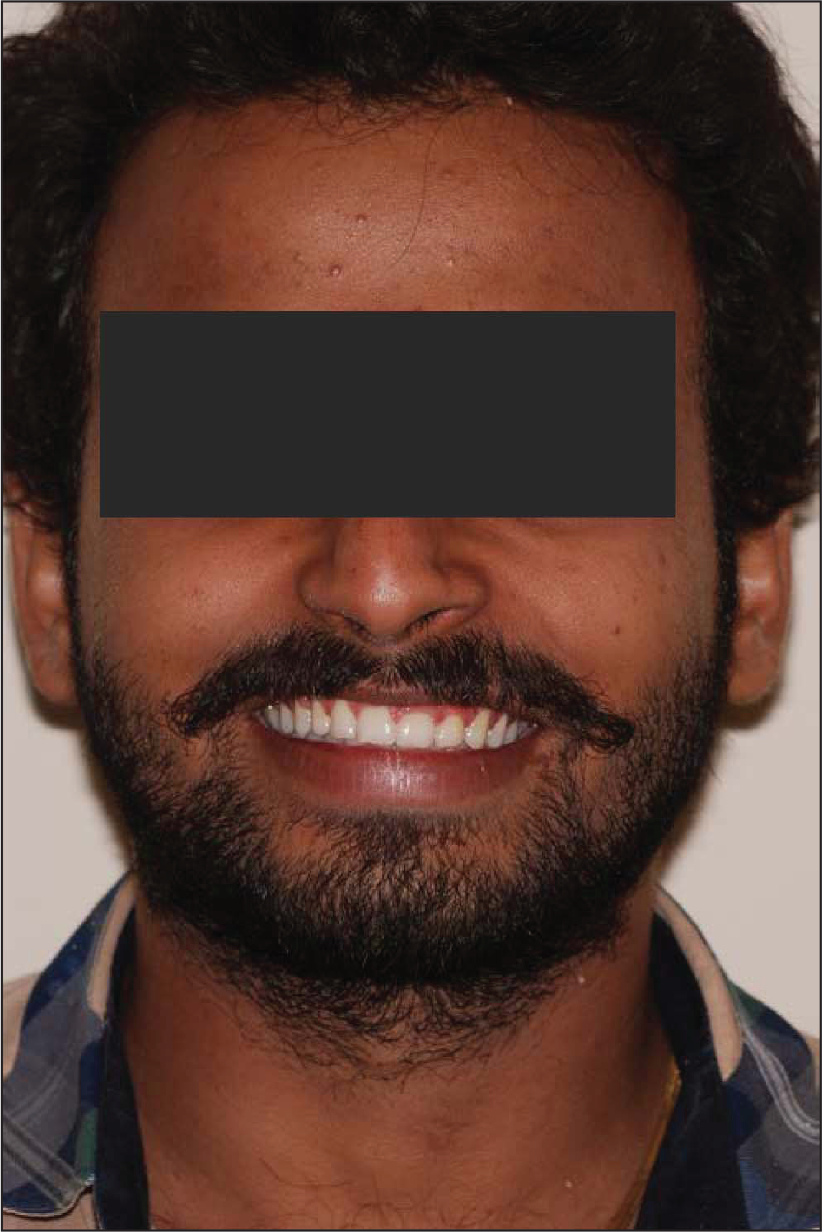
Extraoral examination revealed mild asymmetry due to a depressed canine eminence in upper right maxilla, deviated nasal bridge, slight canting of the interpupillary (3 degree) and the intercommissural (1 deg) lines, normal vertical facial proportions, convex facial profile, competent, nonprotrusive lips. There was an excessive show of upper incisors along with a gummy smile (Figures 1-3).
Extraoral Pretreatment Frontal
Extraoral Pretreatment Profile
Extraoral Pretreatment Smiling
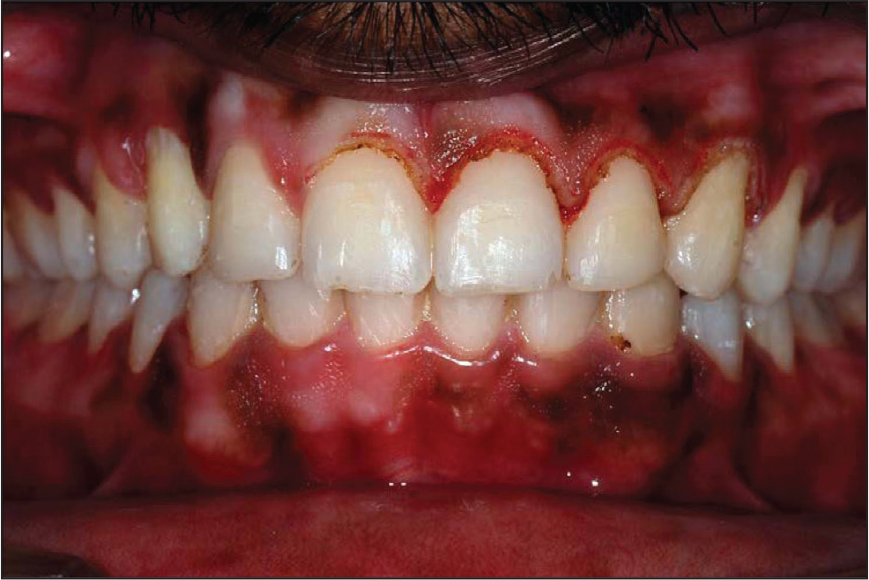
Intraoral examination revealed exaggerated canine fossa due to absence of root prominence of 13, exaggerated root prominence of 12, 14, and all upper anterior teeth, irregular gingival contours of 11, 12, 21, 22, 23 with increased thickness of attached gingiva and presence of pseudopockets. The oral hygiene was fair. All teeth except 13 were present. The third molars were partly erupted (Figures 4-8).
Intraoral Pretreatment Left Lateral

Intraoral Pretreatment Frontal

Intraoral Pretreatment Right Lateral

Intraoral Pretreatment Upper Occlusal

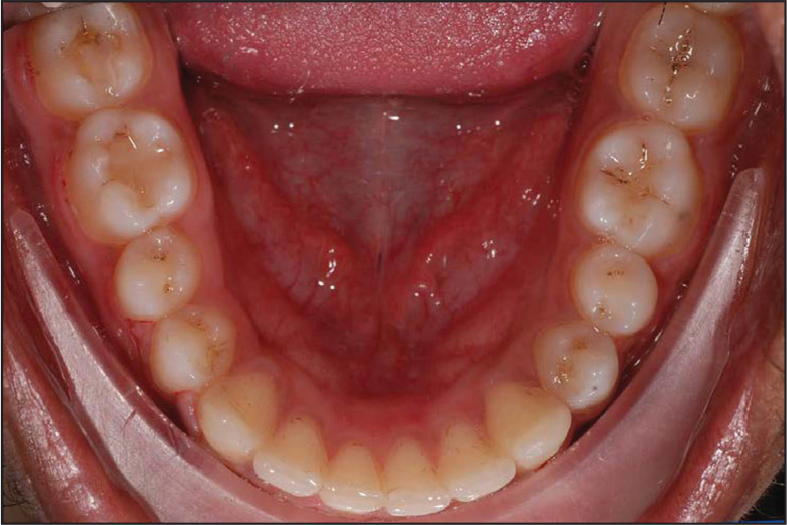
Orthodontic evaluation revealed 8 mm spacing in upper arch and 3 mm crowding in lower arch.
Occlusal evaluation revealed an overjet of 1.5 mm and an overbite of 4.5 mm. The upper midline was shifted to the right and lower shifted to the left. Angle’s Class I molar and Class II canine were present in left buccal occlusion and Angle’s Class I relationship in right buccal occlusion. The tooth #34 was in lingual crossbite. There were asymmetric upper and lower arch forms. There was a reverse curve of Spee in upper arch causing a pseudo-deep bite. There were wear facets on palatal cusp of 24, and 24 showed slight rotation.
Intraoral Pretreatment Lower Occlusal

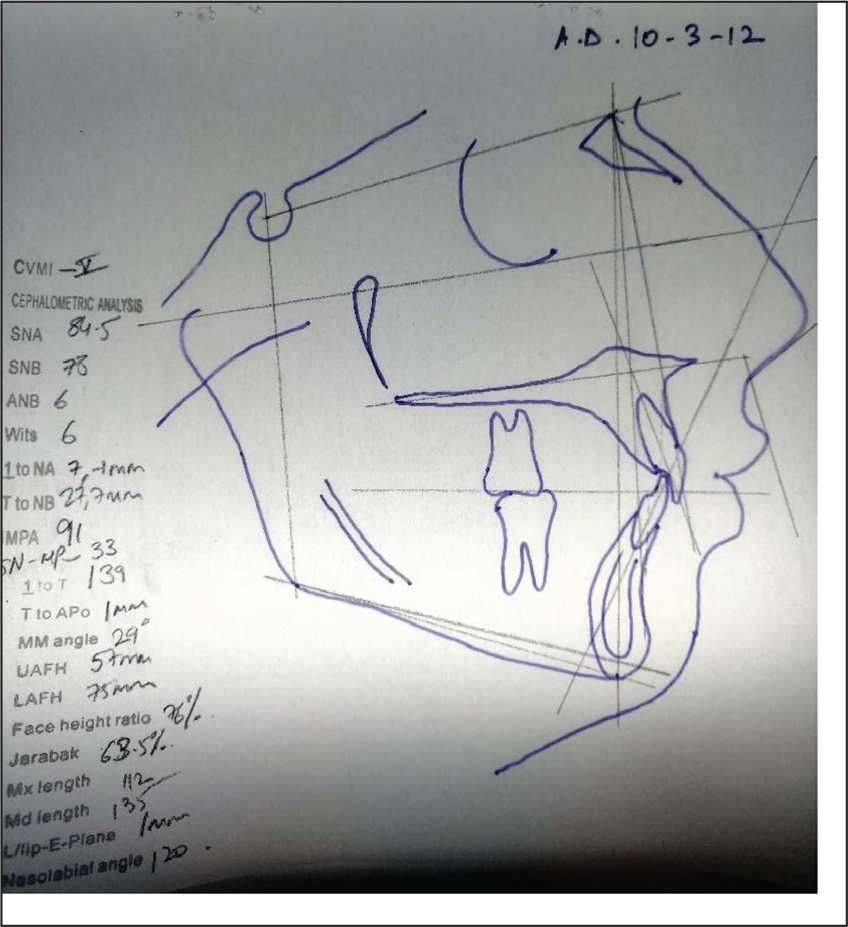
Pretreatment Lateral Cephalogram Tracing
Pretreatment OPG Snapshot
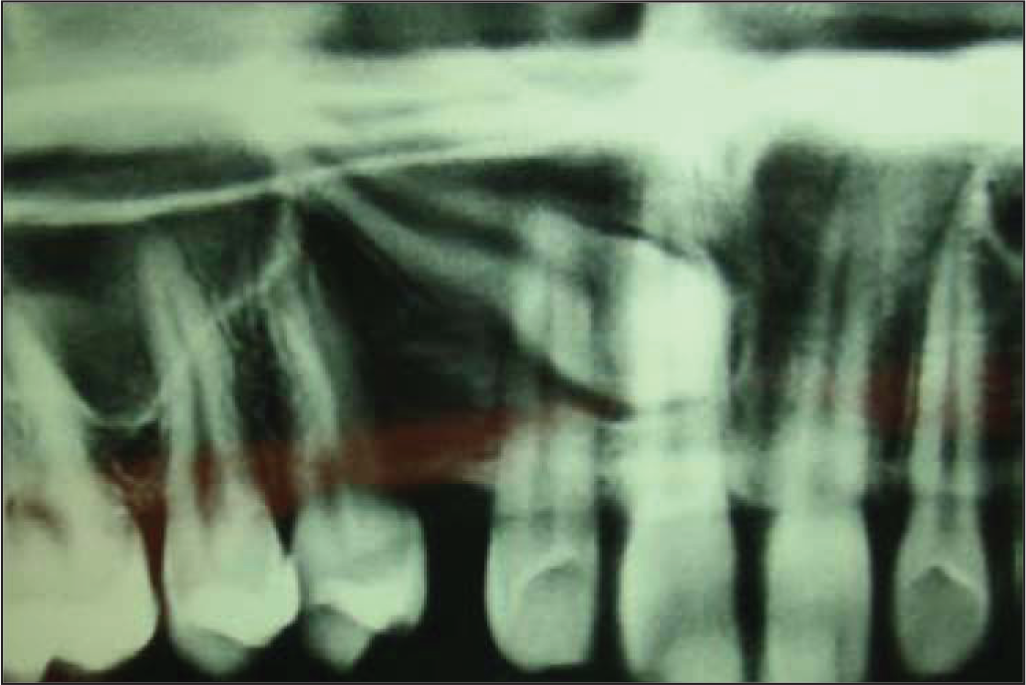
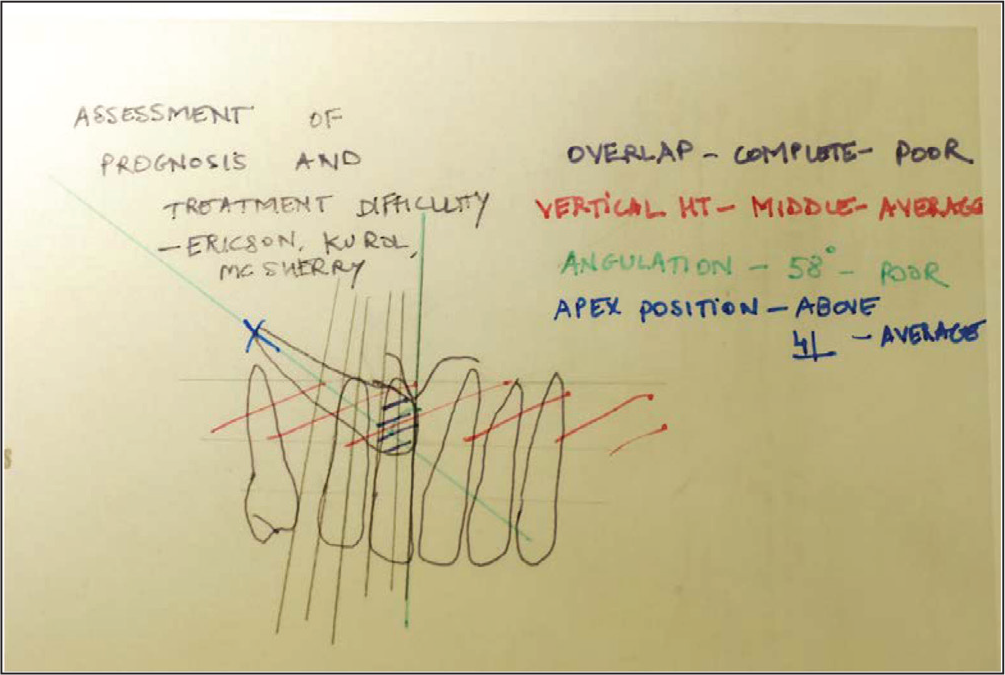
Difficulty of Treatment Analysis of OPG
Model analysis indicated an Ashley Howe’s index of 37% suggesting that the case was borderline extraction. Tooth-size analysis indicated average sized upper and lower total tooth material. Nance Carey’s index suggested extraction of lower second premolars. Bolton’s analysis suggested normal proportions (while calculating we assumed an equal width of 13, 23).
General Radiographic Examination
Pretreatment lateral cephalogram tracing in Figure 9, orthopantomogram (OPG) and spiral CT scan were evaluated.
The OPG snapshot (Figure 10) showed a horizontally impacted no. 13 almost touching the midline. It was analyzed for difficulty of treatment of canine impaction and prognosis assessment as per Ericson and Kurol. 3 The horizontally impacted and palatally placed canine was in zone 5 (crown in the region of upper incisors), with crown at an average vertical height, poorly angulated (>30 deg to the midline), and the root tip positioned above the first premolar (Figure 11).
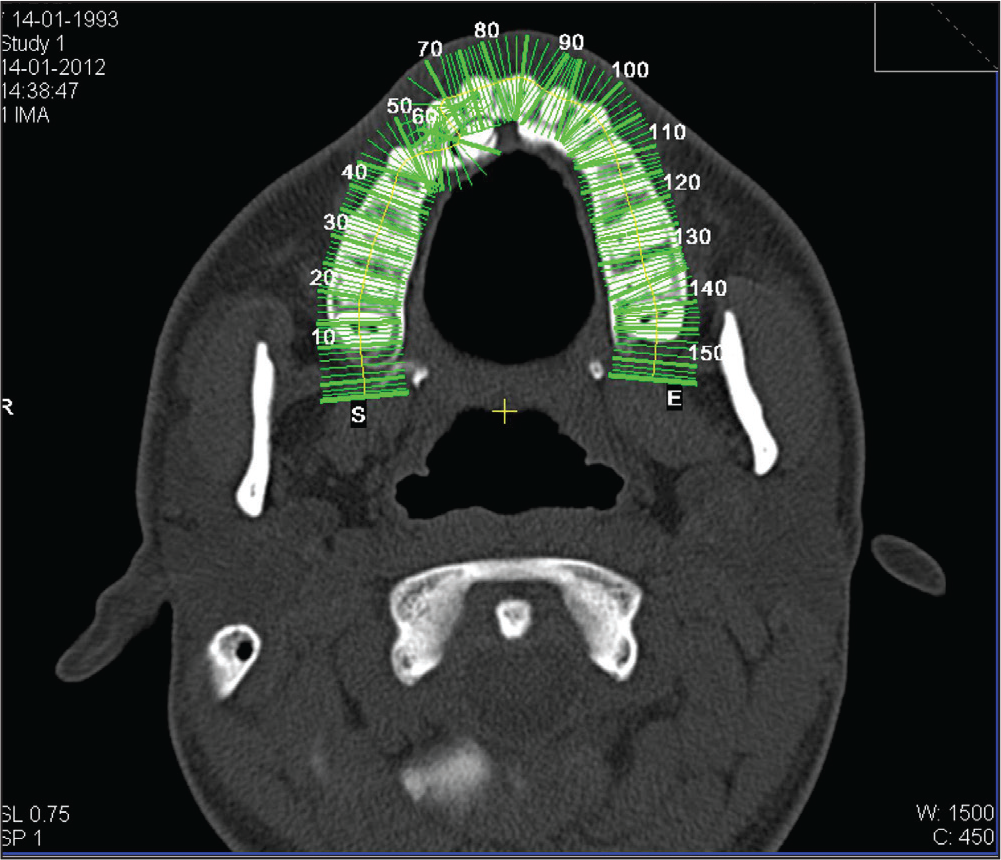
Slice Numbers of the Spiral CT Scan
The upper midline was shifted to the left with respect to the anterior nasal spine (ANS).
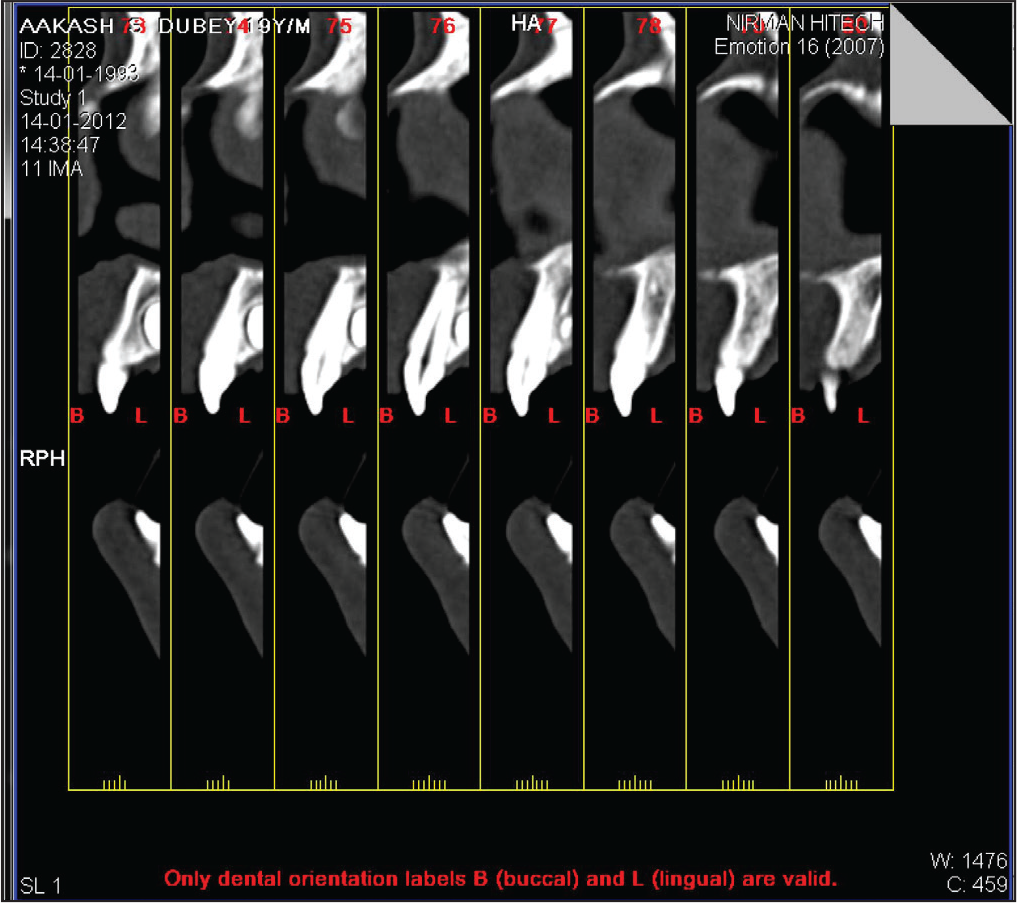
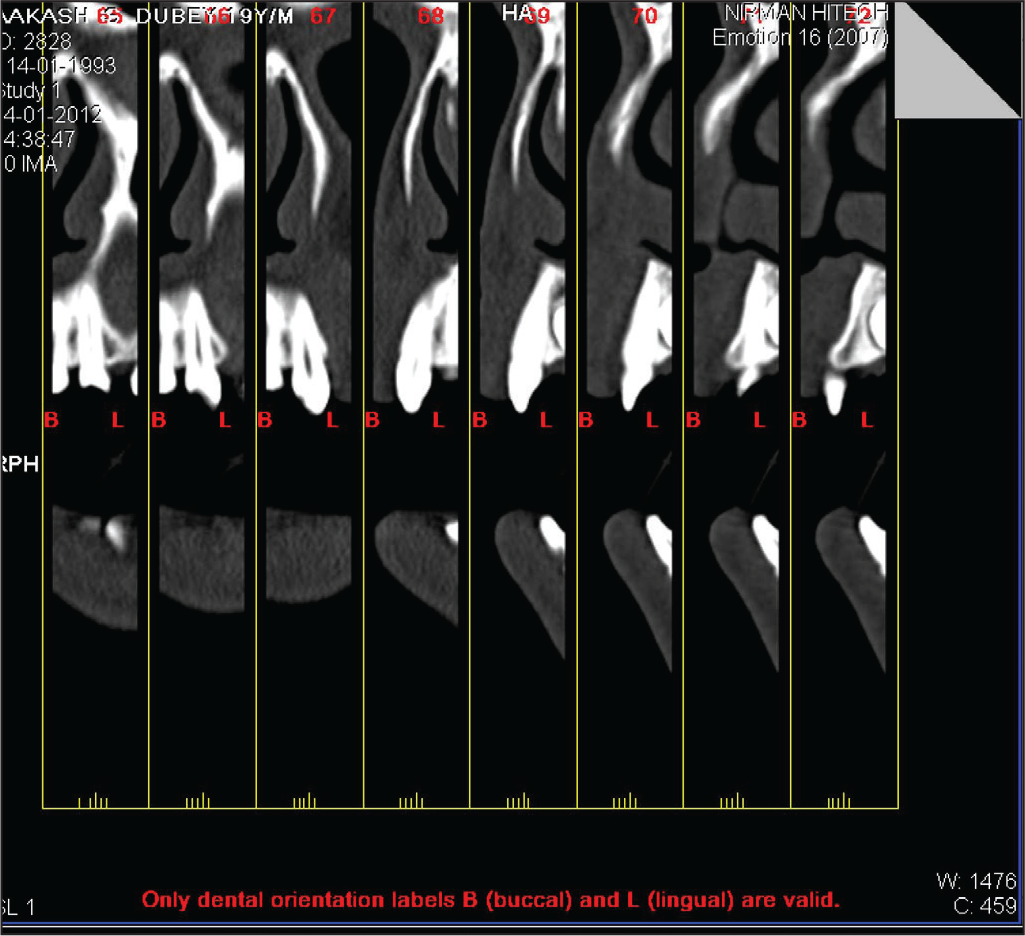
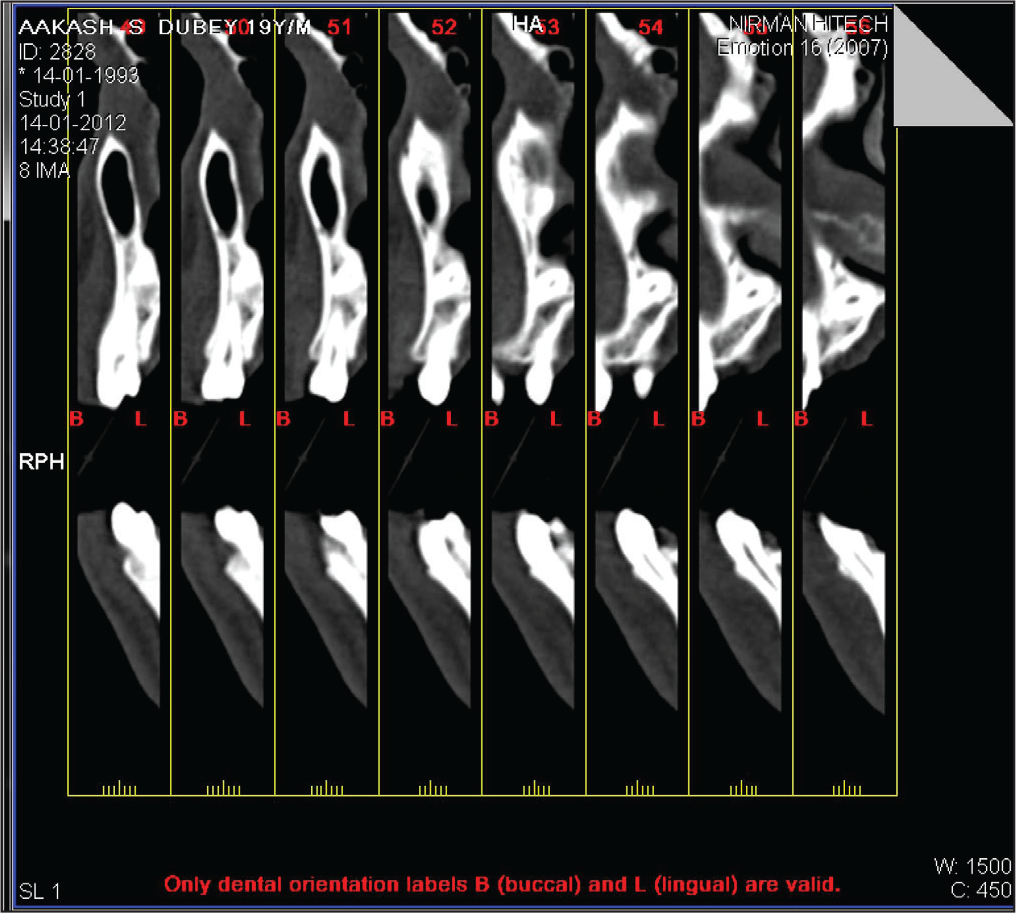
Spiral CT analysis (Figures 12-16) revealed crown of #13 approximately 6-7 mm palatal to the root of #11 with lingual surface towards palatal soft tissue; the root tips were above and palatal to the root tip of 14. The crown was almost touching the midline. Alveolar bone in the region of 13 was thinned out due to early exfoliation of #53. Slices 53 and 54 (Figure 16) show the alveolar bone thinning in the 13 region and the bony concavity in the alveolar ridge. Occlusal radiograph (Figure 17) showed the proximity of the root of the impacted canine with respect to the apices of the premolars.
Slice Numbers 73-78, Crown Tip to Mid-Crown
Slice Numbers 65-72, Crown Position
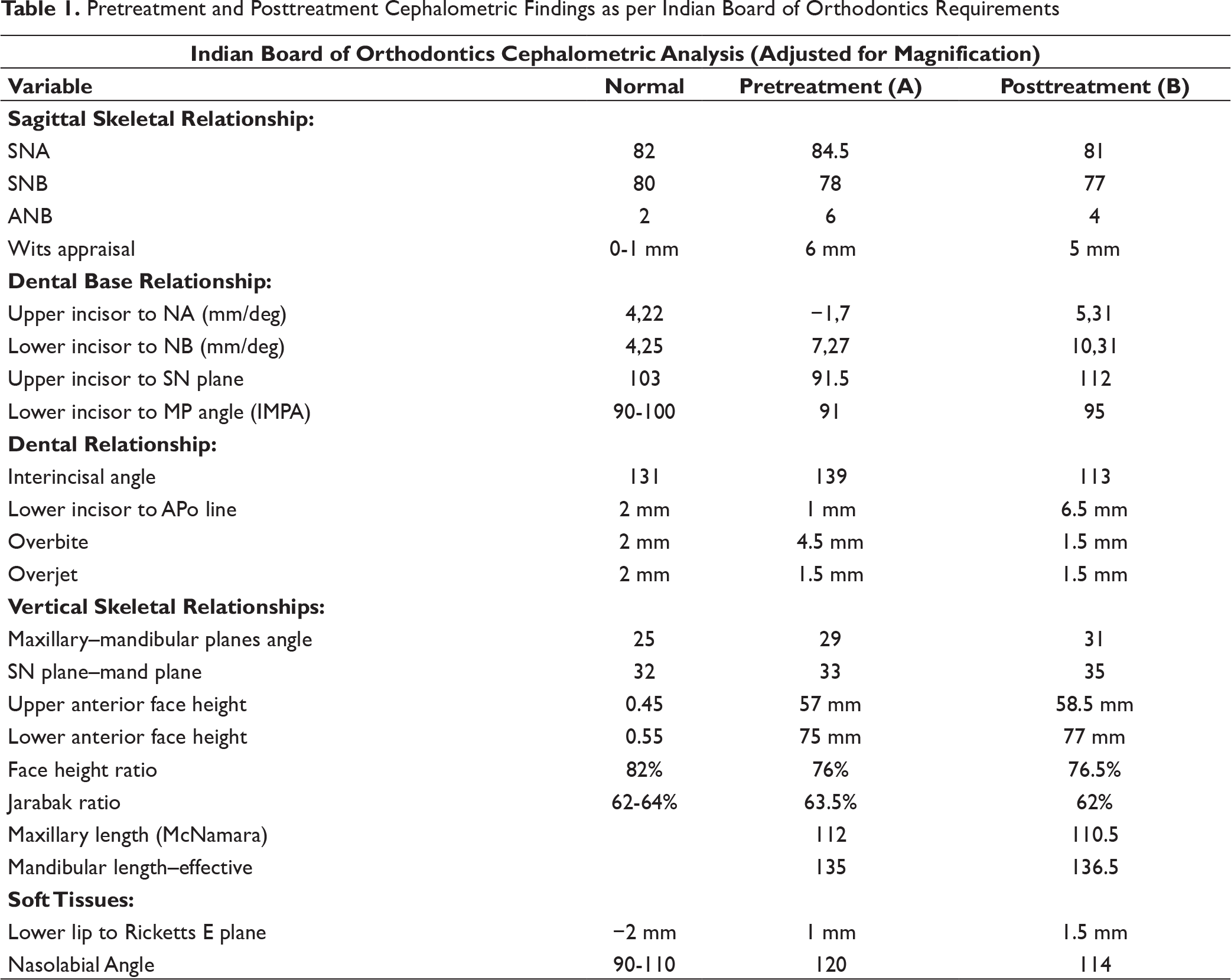
Pretreatment and Posttreatment Cephalometric Findings as per Indian Board of Orthodontics Requirements
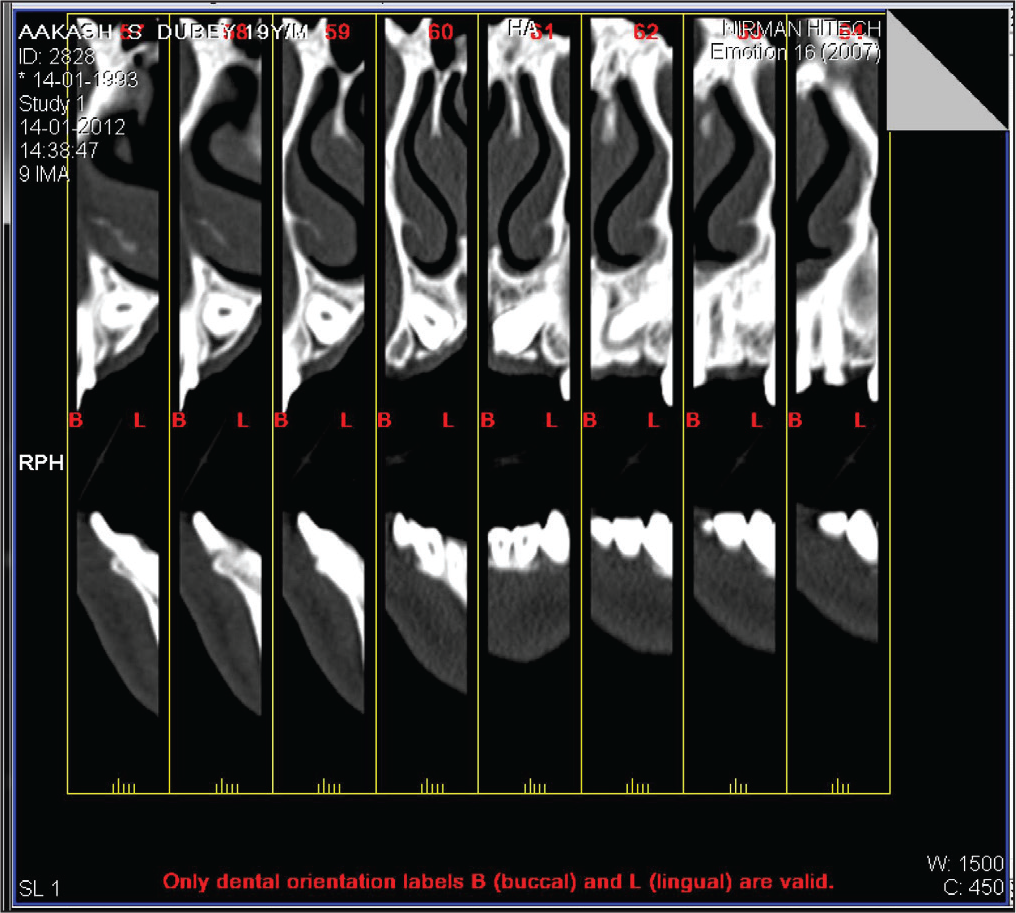
Slice Numbers 57-64, Cemento Enamel Junction to Mid-Root
Slice Numbers 49-56, Root Tip Views
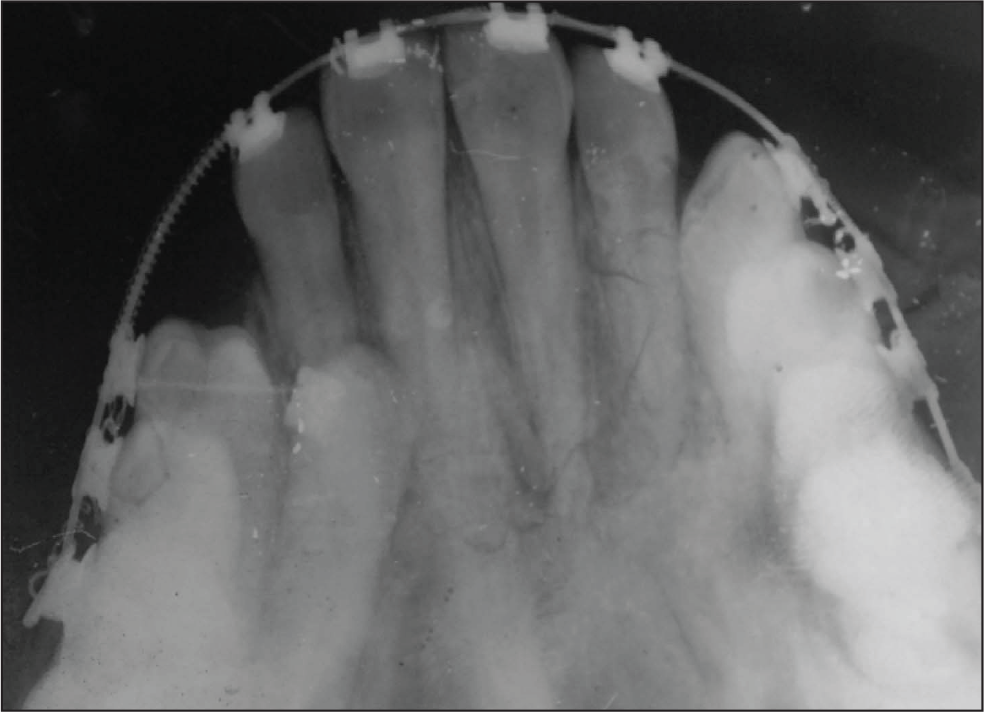
Occlusal Radiograph of Upper Arch Taken Prior to Surgical Exposure
Holdaway’s Soft Tissue Analysis 5
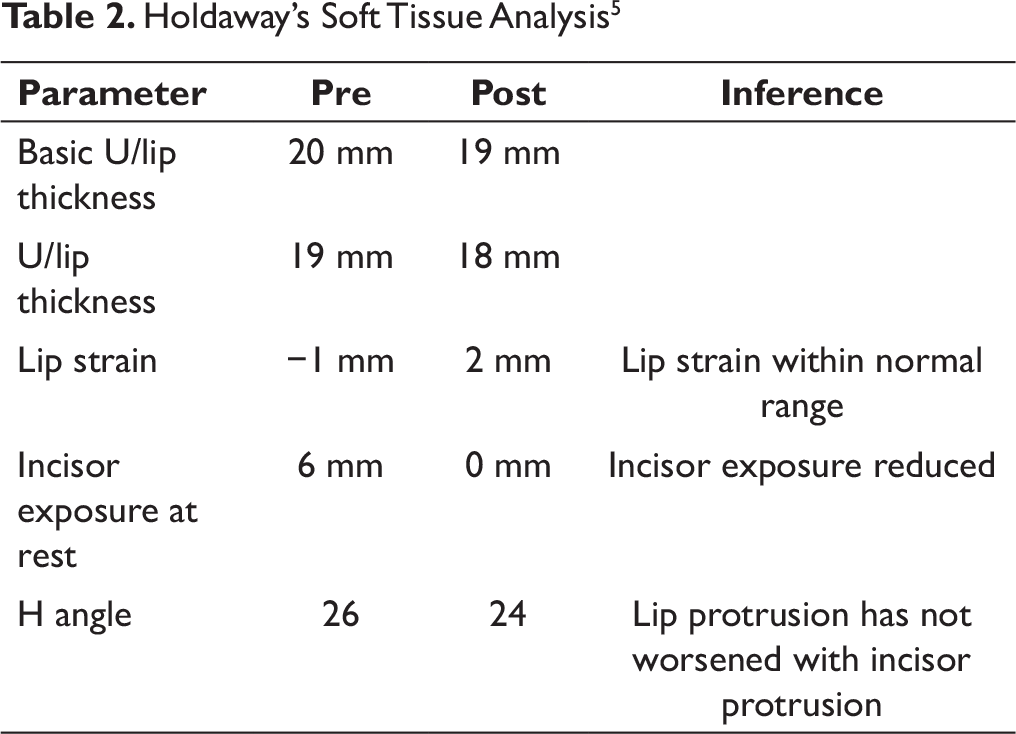
Pretreatment cephalogram was traced and the findings have been tabulated in Tables 1 and 2. They revealed a skeletal Class II base with slightly retrognathic mandible and tendency towards a vertical growth pattern. The upper incisors were retroclined and lower incisors displayed compensatory proclination with an acceptable soft tissue profile and an increased nasolabial angle. There was negative lip strain and increased incisor exposure at rest. Facial proportions indicated an increased lower facial height. Increased basal plane angle indicated an increased mandibular anterior dental height.
Based on the above evaluations, the following diagnosis was arrived at along with a problem list and treatment objectives
Diagnostic Summary
The 19-year-old patient presented with a dental Class I on a skeletal Class II base with a vertical growth pattern. The upper and lower anteriors were retroclined. There was a palatally positioned horizontally impacted 13. There was mild maxillary asymmetry due to a depressed upper right canine region with asymmetric upper and lower arch forms and deviated midlines. There was canting of the interpupillary plane and a minor cant of the intercommissural line. There was upper dental spacing and lower dental crowding with a pseudo-deep bite. The upper anterior gingival contours were irregular with pseudopockets and increased attached gingival heights. There was mild rotation of 14, 24 and a lingual crossbite of 34. The oral hygiene was fair. The soft tissue profile was acceptable.
Problem List
Palatally impacted 13
Upper arch spacing
Lower arch crowding
Asymmetric arch forms, dental rotations
Deep bite
Retroclined upper and lower incisors
Irregular gingival contours, increased gingival exposure on smile, and pseudopockets in upper anterior teeth
Aims and Objectives of Treatment
Alignment of impacted 13 and upper and lower anterior and posterior teeth
Correct upper and lower anterior inclination
Correct deep bite
Close upper arch spaces
Decrowd lower arch
Correct asymmetric arch forms and midline shift
Correct irregular gingival contours
Reduce incisor exposure
Achieve Class I molar and canine relationship
Establish and maintain harmonious soft tissue balance
Treatment Plan
Despite the difficulty involved in treating, in time and effort, the unfavorably positioned 13, the treatment of choice was to attempt to save it for the following reasons.
Absence of canine eminence resulted in a depressed facial appearance of the upper right canine region. It was assumed that by sufficient labial torque application to the canine root after alignment, at least some alveolar support could be regained. A shorter treatment plan against the selected plan would have been to extract the impacted canine and restore the missing canine with a prosthodontic implant. The oral surgeon opined that bone graft would be additionally required to place the implant with an optimum inclination. However, the patient refused the same. The patient was well aware of the difficulty and time involved in correcting the canine impaction and assured his cooperation towards his preferred mode of treatment. Space required for decrowding the lower anteriors would be gained by slight proclination of the lower anteriors. Deep bite would be corrected by intrusion of the upper anterior and by correcting the inclinations of the upper and lower anteriors. This was favored by the increased nasolabial angle and the negative lip strain at pretreatment.
No extractions were required. A 018 (McLaughlin Bennett Trevisi) MBT prescription metal preadjusted appliance was chosen.
Special Anchorage Requirements
We planned to use a piggyback light wire spring to upright the root and torque it later in treatment. Second molar bonding would assist in maintaining arch form.
Minor Adjunctive Surgery
Surgical exposure of impacted 13 using the palatal flap technique
Gingivectomy at the end of treatment to idealize gingival contours and improve smile esthetics
Additional Dental Treatment
Recontouring of the incisal edges of the anterior teeth if need be
Restorative fillings as and if needed
Oral prophylaxis as and when required
Proposed Retention Strategy
Upper Hawley’s retainer plate with a 4-4 labial bow and with a moderate anterior bite plane. Lower lingual bonded retainer with a dead-soft, flat cross-section, sandblasted Stainless steel (SS) wire.
Additional Notes on Treatment Plan
Care was to be taken to ensure that there were no adverse effects on the roots of the teeth or on the periodontium in course of the prolonged treatment duration.
Prognosis for Stability
Once the canine would be in alignment, the lack of spaces in upper arch, proper interincisal relations, idealized arch forms, good cusp-fossa interrelationship, and harmonious soft tissue balance would help in leading to a good prognosis for stability.
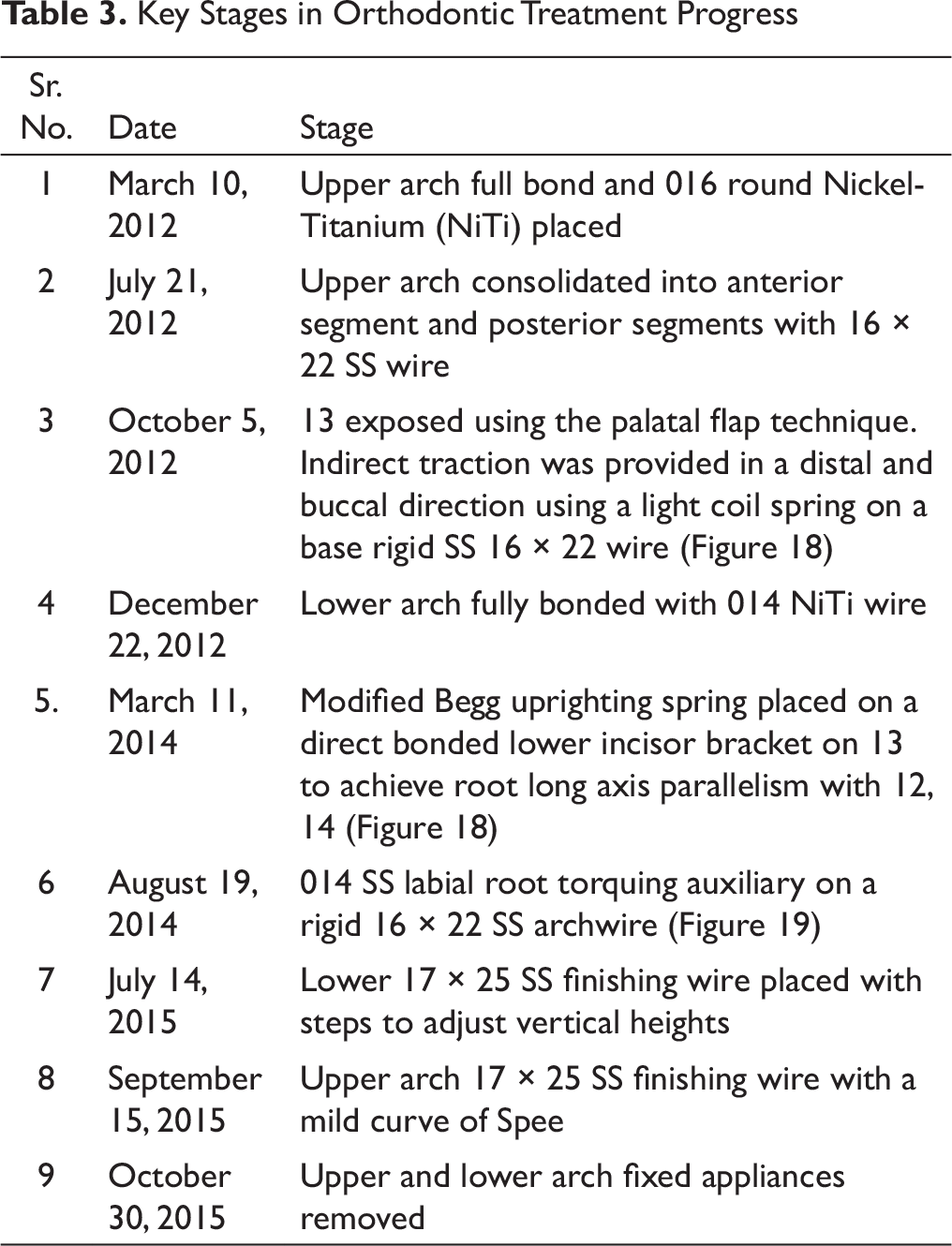
Treatment Progress
Key Stages in Orthodontic Treatment Progress
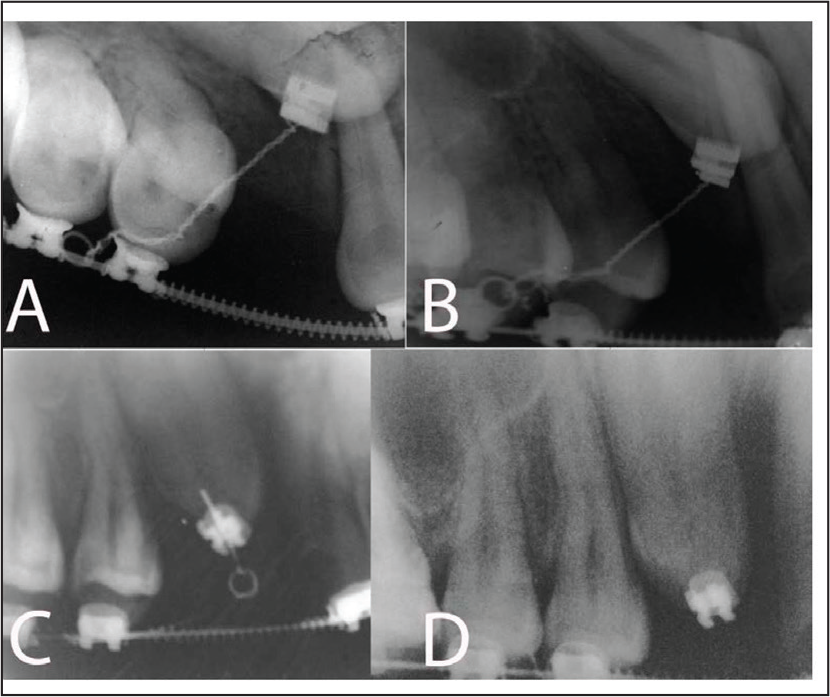
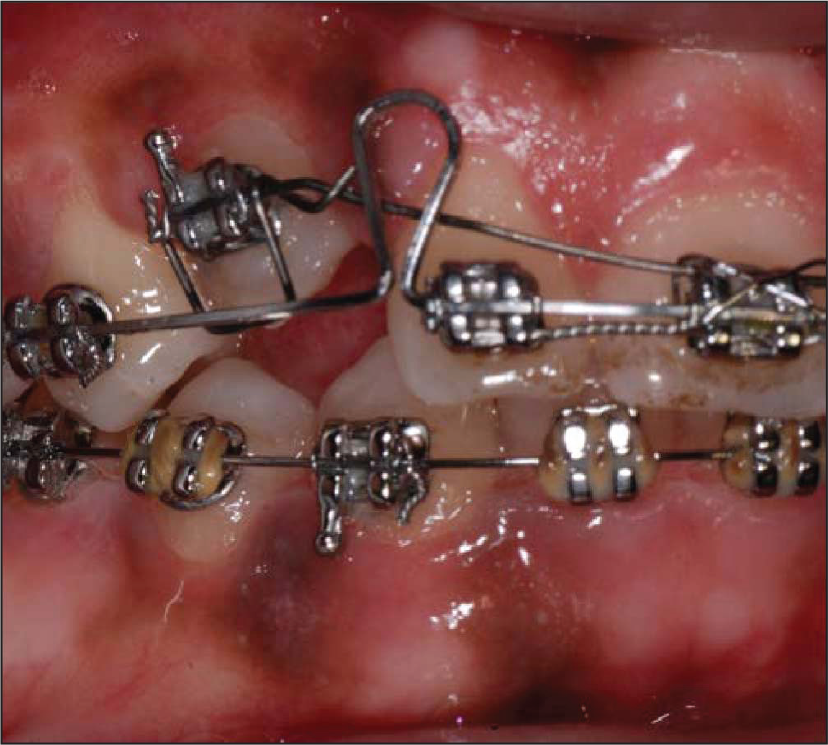
Series of IOPAs to Show the Progress of the Movement of Canine Crown Initially With a Tipping Force from Coil Spring and Later Using Begg Root Uprighting Springs
Light Wire Root Torquing Auxiliary to Torque the Canine Root Labially
Subsequently minor enamel recontouring was done for the upper incisors and canines along with a laser gingivectomy to idealize the gingival contours.
Posttreatment Assessment
Photographs, OPG, lateral cephalogram and IOPA upper anteriors were taken at the end of treatment.
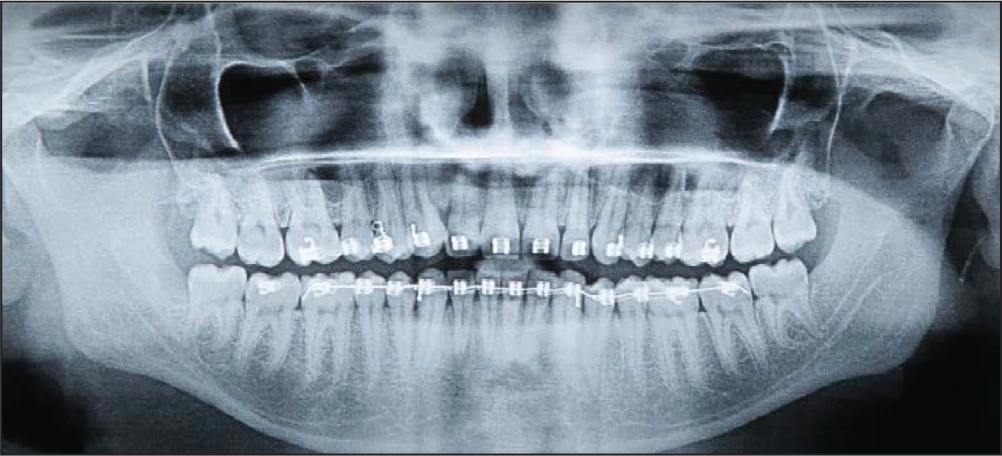
Root parallelism was achieved in all teeth with slight deviation in 32, 34. Alveolar bone heights were normal. Mildly reduced bone level was seen in the mesial of 13. The third molars were partially erupted even at the end of treatment (Figures 20 and 21).
Posttreatment Lateral Cephalogram

Posttreatment OPG
Posttreatment cephalometric findings (Tables 1 and 2) were interpreted as follows.
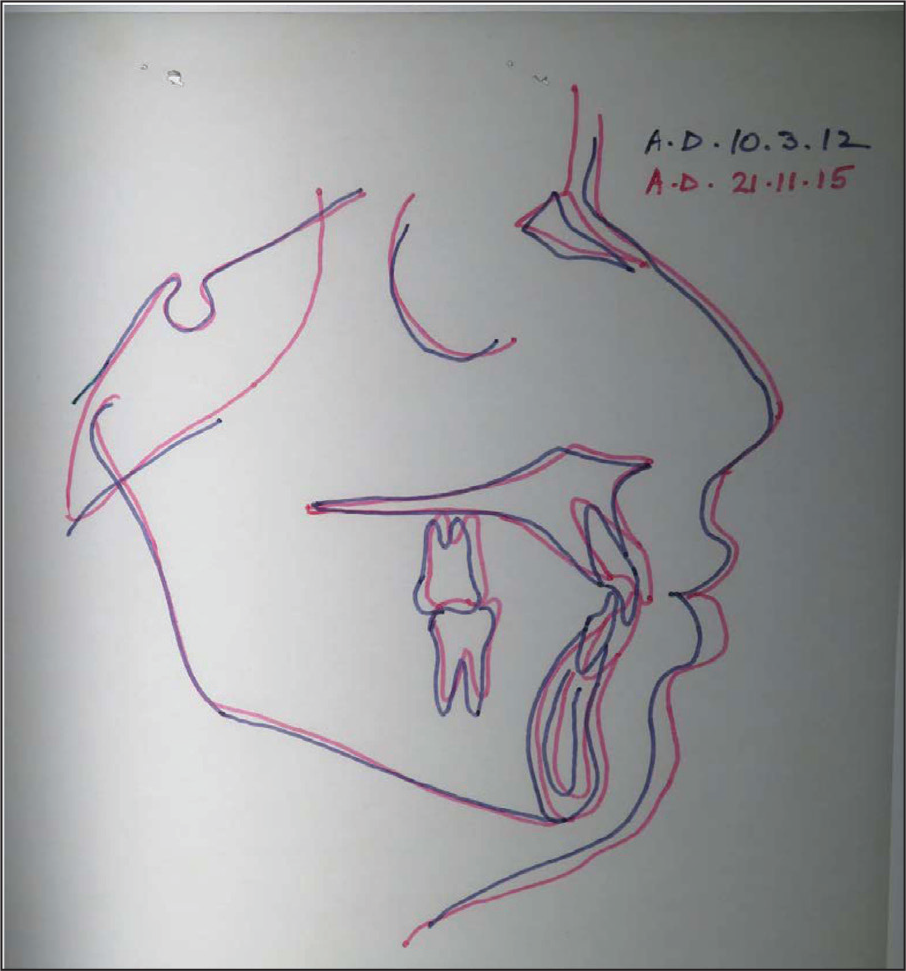
There was an improvement in the ANB angle along with the correction of the retroclination of the upper anteriors and some minor late mandibular growth. There was a marginal opening of the mandibular plane angle favoring the correction of the dental deep bite. The retroclined lower anteriors were also proclined slightly to achieve a favorable interincisal relation. The lip strain consequent to treatment was well within Holdaway’s acceptable limits. The upper incisor was intruded to reduce incisal exposure at rest. The superimpositions are shown in Figure 22.
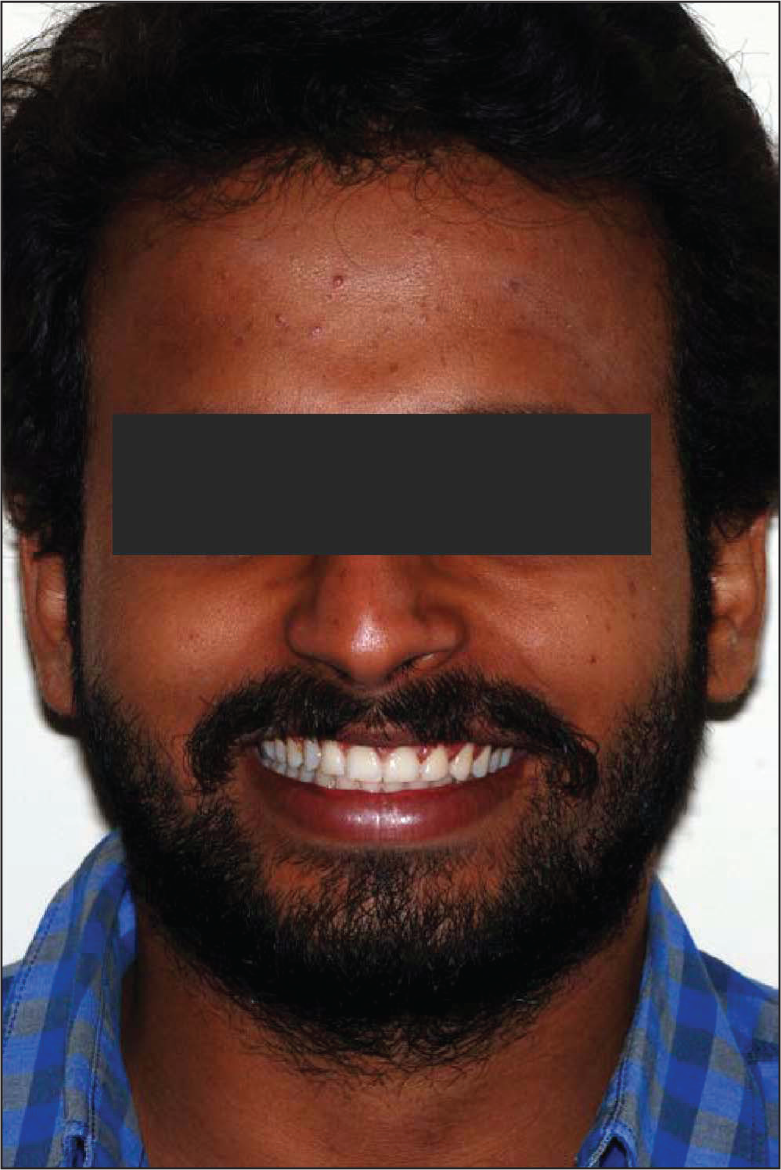
The patient and his parent were extremely satisfied with the results of the orthodontic treatment. All the stated objectives were achieved to satisfaction. The treatment not only vastly improved the facial and smile esthetics (Figures 23-25) but also did not cause any adverse effects on either the roots or the periodontium despite the long duration of treatment.
Cephalometric superimposition
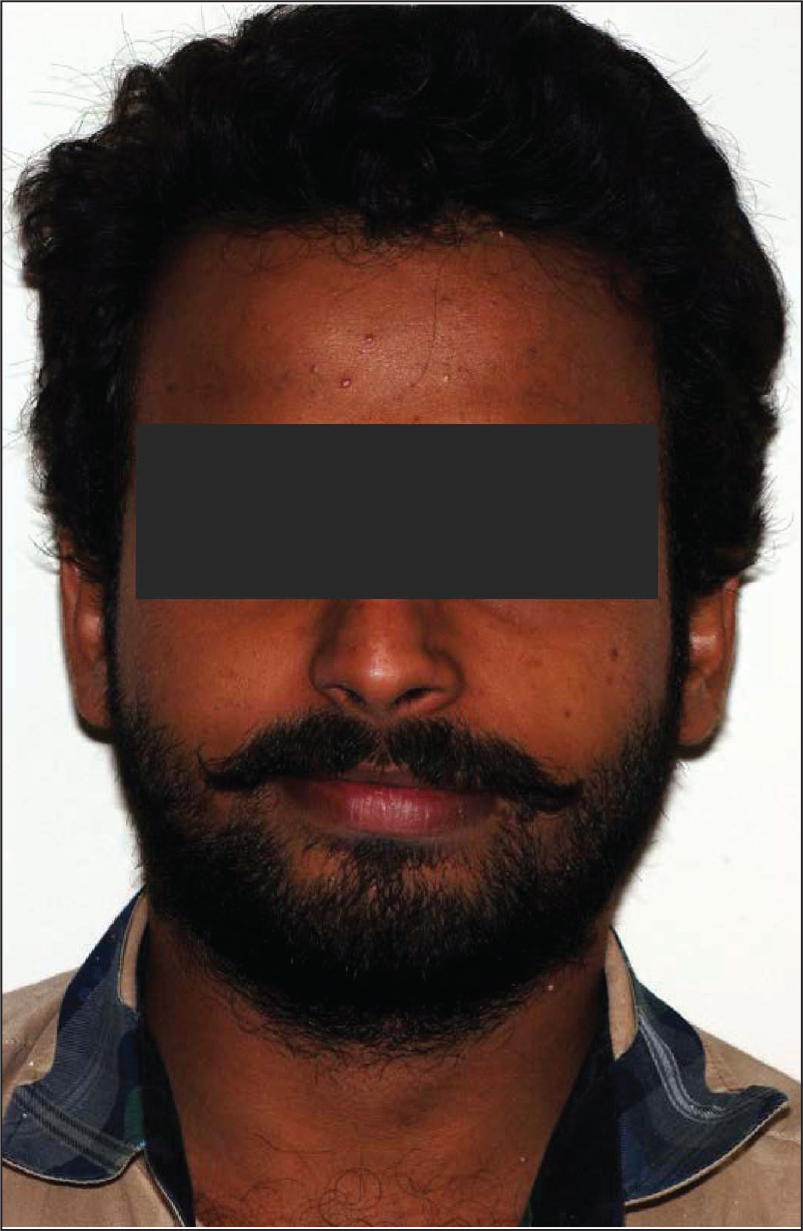
Extraoral Posttreatment Frontal
Extraoral Posttreatment Profile

Extraoral Posttreatment Smiling
Intraoral Posttreatment Left Lateral

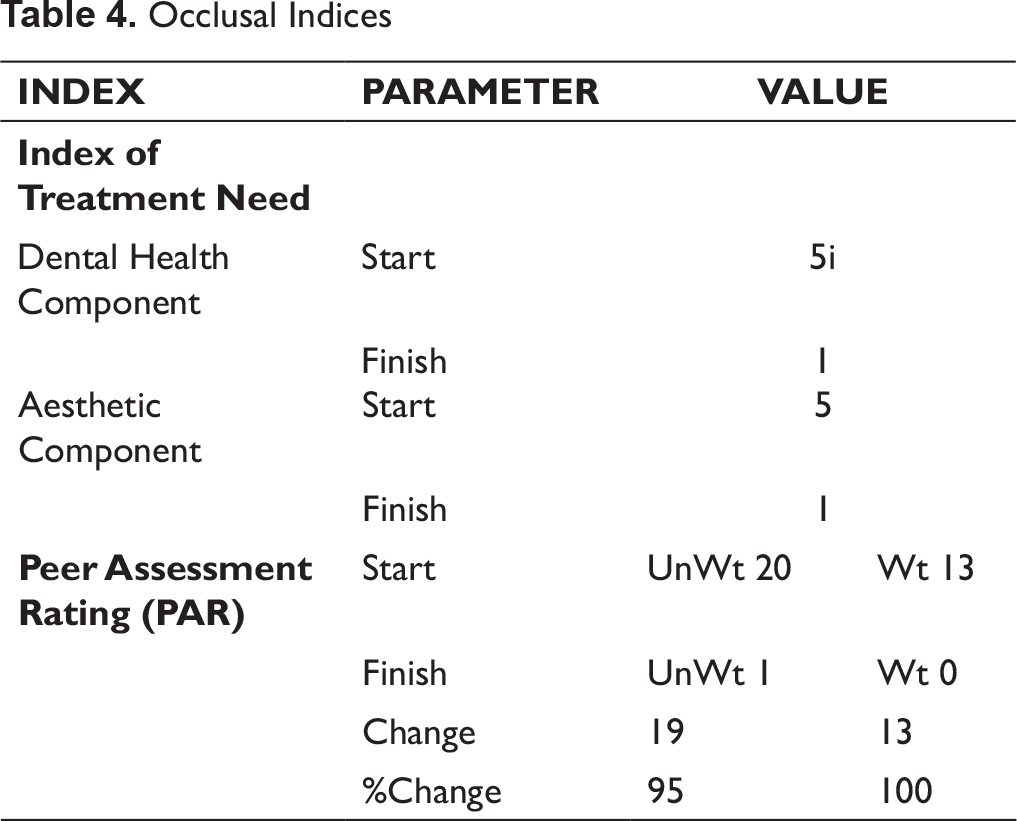
An overjet of 1.5 mm and an overbite of 2 mm were achieved. There was a slight shift of lower midline to the right by less than 0.25 mm. Class I canine and molar relations were achieved on both sides with excellent improvements in the Occlusal Indices. (Table 4). Crossbite of 34 was corrected (Figures 26-30).
There were no mandibular deviations during closure. A mutually protected occlusion with canine guidance during excursive movements was achieved. Excellent interdigitation of the upper functional lingual cusps into the fossae of the lower teeth was achieved. Enameloplasty was done on 13, 21, and 22 for microesthetics.
Intraoral Posttreatment Frontal

Intraoral Posttreatment Right Lateral

Intraoral Posttreatment Upper Occlusal

Intraoral Posttreatment Lower Occlusal
Intraoral Posttreatment Frontal After Laser Gingivectomy
Extraoral Posttreatment Smiling After Laser Gingivectomy
Complications Encountered During Treatment
The impacted 13 had pointed incisal edges with sloping marginal ridges. They were very prominent compared to the blunt edge of the erupted and functional 23. Esthetic recontouring of the incisal edge of 13 was therefore necessitated. The gingival margin of 13 was also way higher than 23. Therefore the 13 was extruded and 23 slightly intruded by bracket positioning. The extrusion of 13 complemented the recontouring of the edge. There was no resultant sensitivity in 13. Fluoride application was done consequently.
The impacted canine 13 was discovered to have a morphologically flat buccal contour and different hue. Therefore, an attempt was made to place it as buccal as possible within the constraints of the alveolar bone. Though from an orthodontic perspective it did not feel enough, the patient was more than satisfied with the final 13 position. A laminate mock-up that significantly improved smile esthetics was also shown to the patient but the patient chose to decide on it later.
At the time of debonding, poor gingival contour gave an appearance of canting of smile line, but this changed significantly with idealizing the gingival contours with a laser gingivectomy and minor incisal edge recontouring (Figures 31 and 32).
There was a loss of approximately 14 months of treatment time due to missed appointments in the course of treatment.
Critical Appraisal
Due to the original maxillary asymmetry, a slight cant of 1 deg of occlusal plane to interpupillary line existed at the end of treatment. However, it was not clinically significant to either the patient or his parents or his dental peers. This is supported by literature search which shows that a cant of up to 2 deg was esthetically accepted by orthodontists, general dentists, and laypersons. 4
There was a slight deviation of less than 3 mm of upper midline to upper face. In addition to the existing maxillary asymmetry, this was also caused due to the deviation of the nasal bridge and ANS to the patient’s right.
The 35 had a slight buccal contact with the first molar. However, it offered an excellent cusp-fossa relation with the antagonists.
Occlusal Indices
Conclusion
As envisaged at the start of the treatment, the duration of treatment was long. However, care was taken to ensure that the forces were light throughout the treatment. Therefore, despite the complexity of tooth movements involved in correcting the canine impaction, all treatment objectives were achieved with a conservative approach and without any significant adverse effect on the teeth or the periodontium.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.