
Abstract
Orthodontists play an important role in the management of deleterious oral habits. Lip biting has a multitude of adverse effects on the stomatognathic system. A new appliance has been suggested to manage this habit. It is efficient and has got high patient acceptability.
Introduction
Lips play an important role in deglutition, speech, and maintenance of normal occlusion. Lip biting and lip sucking most often involve the lower lip. It can result in proclination of upper anteriors, flattening and crowding of lower anteriors, increase in over jet, and cracking of lips. When the habit becomes pernicious, the lip itself shows the effects of this abnormal habit.
Lip biting has been traditionally treated with lip bumper, oral screen, or bonding of brackets to palatal surface of upper anteriors.1, 2 A simple and efficient alternative is demonstrated with a clear aligner/retainer. This particular appliance helps to treat lip biting with minimum discomfort to the patient and is esthetically appealing. This can be done as a part of an aligner/retainer or as an individual appliance.
Procedure
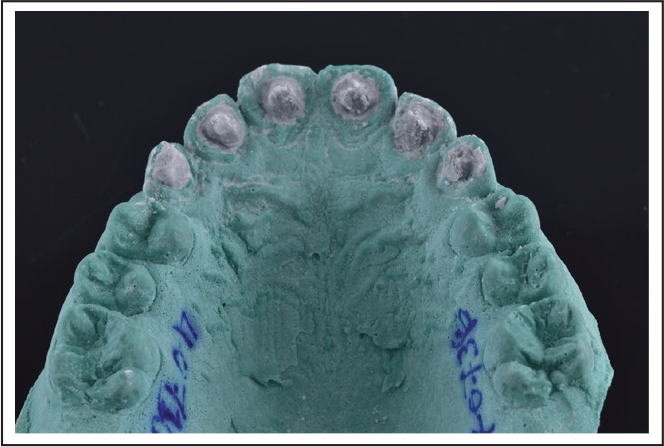
The cast is fabricated using patient’s upper impressions. Button-shaped elevations of around 1 mm to 2 mm diameter and 2.5 mm height are made on the palatal surface of incisors. They could be of smooth round edge or sharp depending on the intensity of habit/need of the individual case (Figures 1–3). Angulation of spikes should be set at 45 to 65 degrees to the long axis of incisors. The clear retainer/aligner is fabricated over this. Advice the appliance full time except during meals and brushing. The spikes make the habit of lip biting uncomfortable for the patient (Figures 4–7). The sharpness of the spikes can vary depending on the need of the case.
Preparation of cast
Clear retainer with elevations

Clear retainer with elevations

Lip biting habit

Clear retainer with elevations in patients mouth

Clear retainer with elevations in patients mouth

Post treatment

Discussion
The success of any habit breaking treatment depends on patient conviction and faithful wearing of the appliance. Even though this is a removable appliance, it is clear, invisible, and transparent. It is much more comfortable than traditional appliances and easily removable and does not affect eating habits. Better oral hygiene maintenance is feasible, and issue of breakage is virtually free compared to other techniques. Patient acceptance is better due to the aesthetic advantage. Even though bonding of brackets to the palatal aspect of upper incisors is also used as a reminder appliance in lip biting, it may require bite raising, which is not encountered in this particular appliance. If required, habit control can be carried out simultaneously with aligner therapy or as a part of retainer phase.
Conclusion
This appliance is not only efficient but also esthetically pleasing and better accepted by the patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.