
Abstract
Introduction:
Altered nasorespiratory function leads to altered craniofacial growth. Thus, airway evaluation is important for preventive, interceptive, and corrective orthodontic treatment. The aim of this study was to evaluate and compare adenoids, the upper airway, the tongue, and mandibular dimensions using “predictors of difficult airways” in class II division 1 and class II division 2 cases with class I cases.
Method:
Sixty subjects of age 15 to 18 years were divided into 3 groups (group 1: class I cases; group 2: class II division 1 cases; and group 3: class II division 2 cases) based on cephalometric parameters, with 20 cases in each group. Cephalometric evaluation of adenoids and the nasopharyngeal airway was done using the Handelman–Osborne area method. Upper and lower airway evaluation was done using McNamara’s linear method. “Predictors of difficult airways” were used for evaluation of the airway, which included nasal competency, the Mallampati scale, mandibular length, mandibular protrusion, and the thyromental distance.
Results:
The present study found a significant positive correlation between the grades of nasal competency and percentage adenoid wall area, and a significant negative correlation between the grades of nasal competency and the upper airway. There was a significant positive correlation between the grades of nasal competency and mandibular length, and a significant positive correlation between the grades of mandibular protrusion and mandibular length. There was a significant positive correlation between the grades of the thyromental distance and mandibular length.
Conclusion:
It was concluded that the “predictors of difficult airways” would be helpful in early diagnosis and identification of potential risk factors that may cause “breathing disorders”–related malocclusions and later on increase the risk of developing OSA.
Introduction
Growth of nasomaxillary complex and mandible is dependent on the function of oropharyngeal capsule and airway spaces. 1 Today, it is an accepted fact that respiratory functions alter craniofacial growth, especially that of mandible, which is most relevant for orthodontic diagnosis and treatment planning. Any obstruction in the airways results in mouth breathing and alters the growth of the jaws. 2 Obstruction in airway is also a matter of concern to orthodontists, pediatricians, otolaryngologists, and speech therapists, as it alters the overall growth and development of a child.
The prevalence rate of mouth breathing among 5 to 13-year-old North Indian children was reported to be 7.8% in boys and 5.3% in girls, respectively. 3 It was the most commonly reported oral habit (29.4%) among 4 to 13-year-old children in central Kerala, India. 4
Predisposing factors to nasorespiratory obstructions include the presence of hypertrophied adenoid, tonsils, nasal polyps, allergic conditions, and structural deformities of nose.
Evaluation of adenoids and airway is carried out by various methods such as lateral cervical radiographs, lateral cephalometric radiographs, rhinometry, nasal endoscopy, cone beam computerized tomography, computed tomography, and magnetic resonance imaging (MRI). However all these methods have some or the other limitations. McNamara’s cephalometric parameters have shown poor sensitivity as a screening tool. 5 Use of computed tomography (CT) is limited due to high irradiation, cost, and restricted accessibility, whereas MRI is not cost-effective for frequent usage. Cone beam CT (CBCT) cannot be repeatedly used due to radiation problems. 6
Analysis of adenoids and upper airway is carried out by ENT surgeons with a flexible fiberoptic nasopharyngography, which is out of reach of orthodontists.
“Predictors of Difficult Airway” 7 which include Mallampati scale, mandibular protrusion, mandibular length (ML), and thyromental distance are routinely used bedside clinical tests by anesthesiologists that require less armamentarium, are more feasible, cost-effective, and noninvasive; hence, they may be useful to orthodontists for airway evaluation and can be included in the diagnostic protocol. Hence, in order to evaluate the usefulness of these “Predictors of Difficult Airway” in Class II Div 1 and Div 2 cases and associate them with those seen in Class I cases, a study was planned and conducted utilizing the “Predictors of Difficult Airways” for diagnosing the cases of altered craniofacial growth so that further worsening can be prevented.
Material and Methods
This prospective observational in vivo study was approved by the ethical committee. Sixty subjects 20 in each group of age 15 to 18 years (mean age 16.5 years) who satisfied the inclusion criteria were selected to observe airway differences in growing adolescents with different skeletal patterns who had no history of prior orthodontic treatment or extractions, myofunctional therapy, maxillary arch expansion, orthognathic surgery, adenoidectomy or tonsillectomy, and neuromuscular disorders. The groups were as categorized as follows: Group 1—Class I cases (Beta angle—28-33°; MP—32-36°; gonial angle—130°±7°; Jarabck’s ratio—62%-65%); Group 2—Class II Div 1 cases (Beta angle—<26°;MP—>36°—gonial angle—>137°; Jarabck’s ratio—<62%); and Group 3—Class II Div 2 cases (Beta angle—<26°; MP—<32°; gonial angle—<130°, Jarabck’s ratio—>65%). The cases in the study were evaluated with the help of lateral cephalogram and clinical examination.
Following methods were used for evaluation of breathing and airway space: Clinical method—Quinn’s nasal competency test Radiographic methods Handelman and Osborne area and McNamara airway analysis. Other clinical methods include “Predictors of Difficult Airway” Mallampati scale; ML; mandibular protrusion test; thyromental distance.
Quinn’s Nasal Competency Test 8
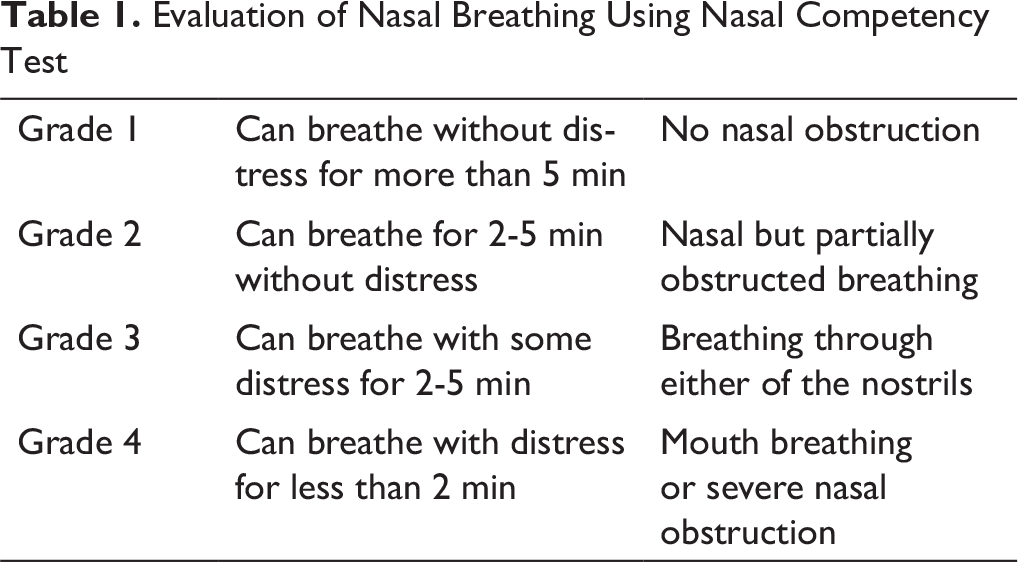
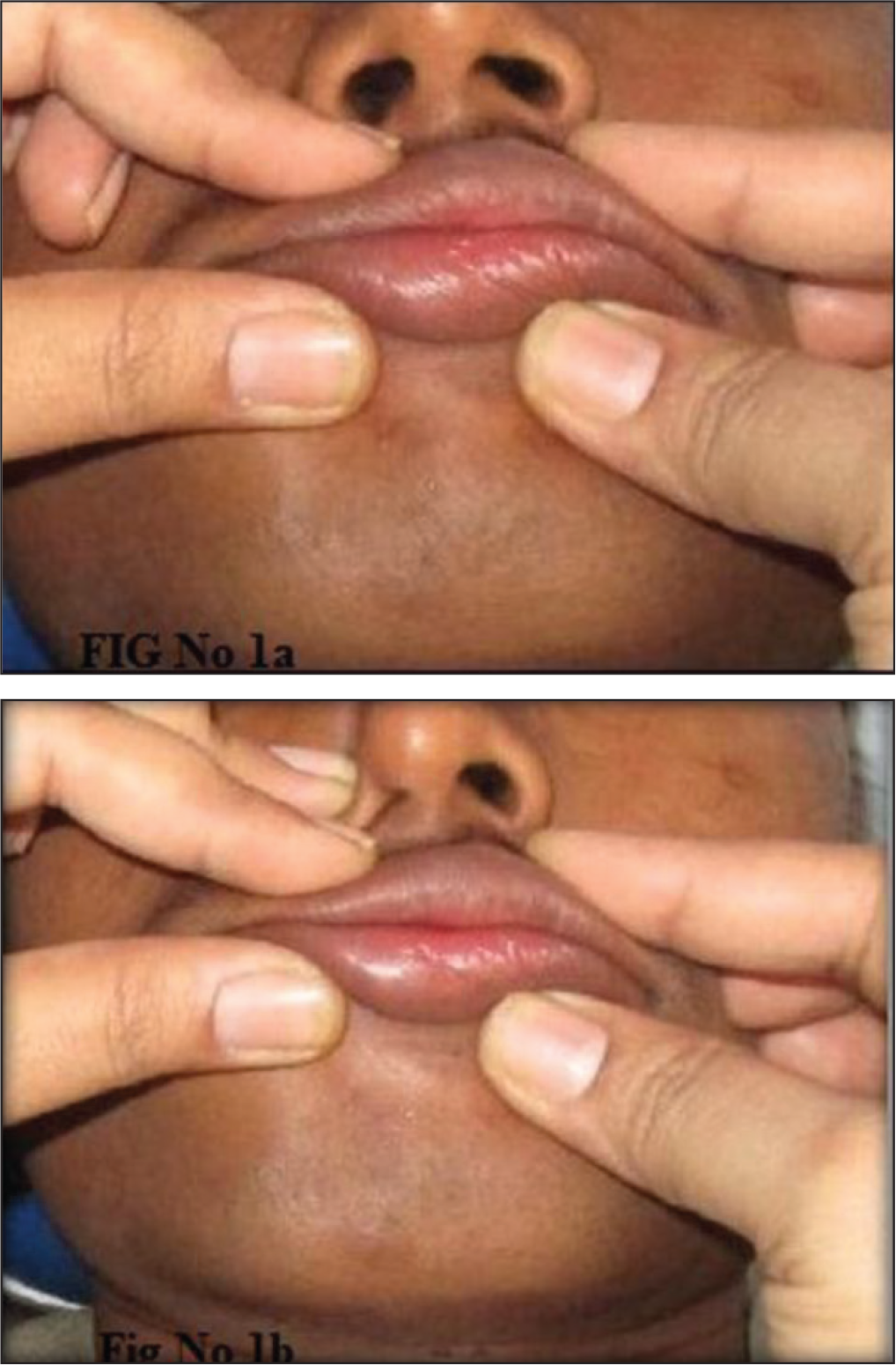
For this, patient’s lips were closed with light pressure of thumb and middle fingers for 2 to 5 min, and the patient was asked to breathe through nose. If a patient is a mouth breather and his/her breathing through mouth is stopped, he/she may become breathless and tries to open his/her mouth. This is indicative of nasal obstruction, either in the nostrils or the nasopharynx. Based on the observations, the categorization was done as given in Table 1 and Figures 1a and 1b.
Evaluation of Nasal Breathing Using Nasal Competency Test
Radiological Evaluation of Adenoids and Airway Space
Handelman and Osborne Area Method 9
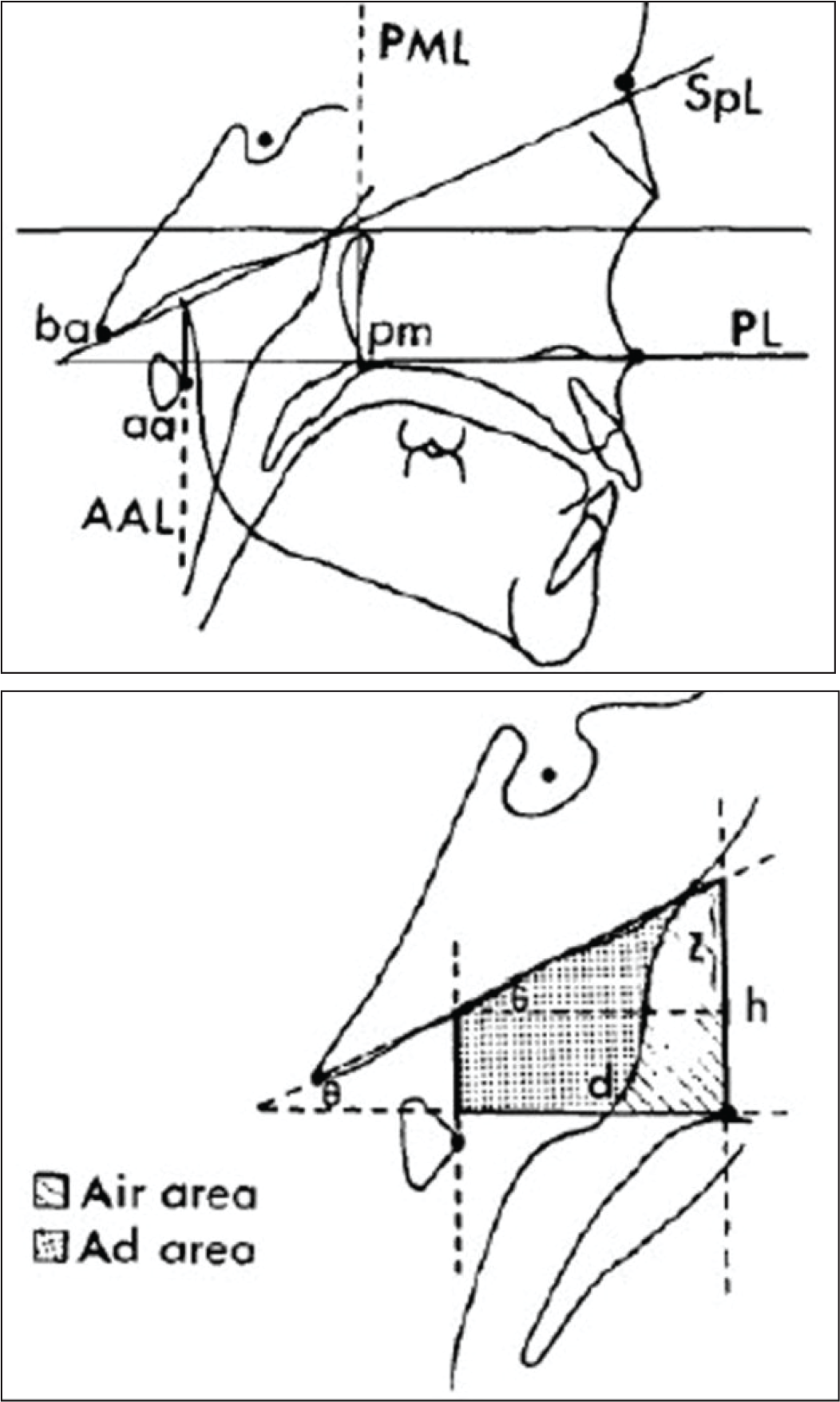
This trapezoid analysis was introduced for quantifying nasopharyngeal dimensions on a lateral cephalogram. The cephalometric reference points and lines used in this method were as follows: Ba: basion SpL: sphenoid line (tangent to the lower border of sphenoid registered on Ba) PL: palatal line (anterior to the posterior nasal spine) Pm: pterygomaxillare PML: pterygomaxillary line (perpendicular to PL registered on Pm) aa: anterior arch of atlas AAL: anterior atlas line (perpendicular to PL registered on aa)
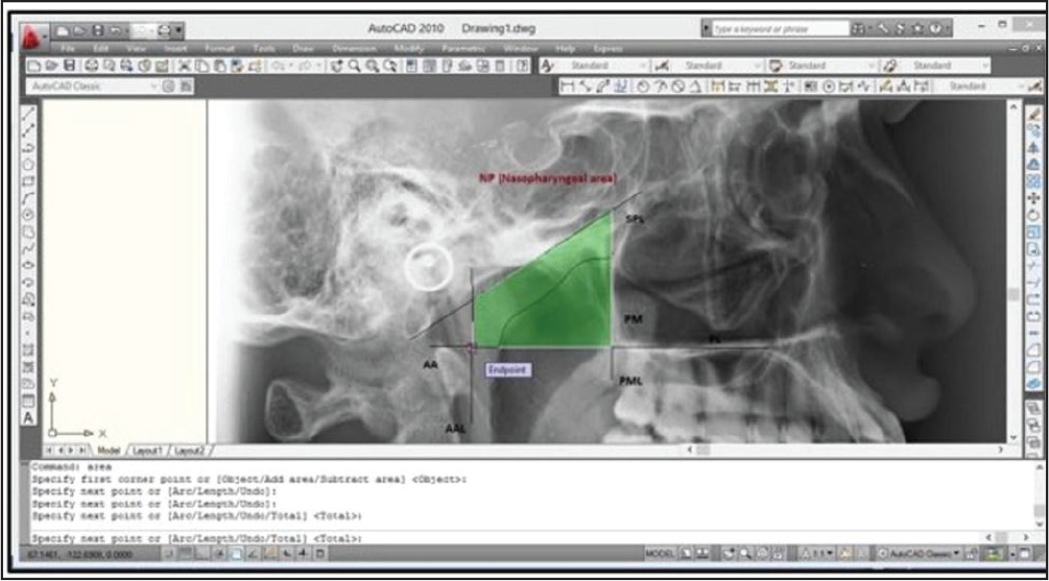
The nasopharyngeal area (Np area) is defined by four lines which form a trapezoid. It is formed by palatal line (PL), sphenoid line (tangent drawn to the lower border of sphenoid registered on Ba [Basion]), anterior atlas line (AAL), and pterygomaxillary line (PML) which is drawn perpendicular to the PL registered on pm (pterygomaxillare) (Figure 2a). It is further divided into adenoid-pharyngeal wall (Ad area is that part of the Np area consisting of soft tissue, ie, adenoid or pharyngeal wall) and the nasopharyngeal airway area (Air area is that part of the Np area, ie, airway) (Figure 2b). Digital lateral cephalograms in JPG format were opened in AutoCAD 2010 software. The image was scaled in mm dimension. Using polyline command from the side bar menu, the required drawing was made, as shown in Figure 3. The first and last selected points of the image were joined, and a closed area formed representing an area. The areas were measured in millimeter square directly using area command. Ad area was derived by subtracting the nasopharyngeal airway area (Air area) from Np area. Then the percentage of air area and percentage of adenoid wall area were obtained and then compared for evaluation (see Figure 3).
Radiographic Analysis of Pharyngeal Airway Using McNamara Analysis 10
In this method, upper pharyngeal width was measured from a point on the posterior outline of the soft palate to the closest point on the posterior pharyngeal wall. The average value is 15 to 20 mm. If it is 5 mm or less, then it is an indicator of impaired airway.
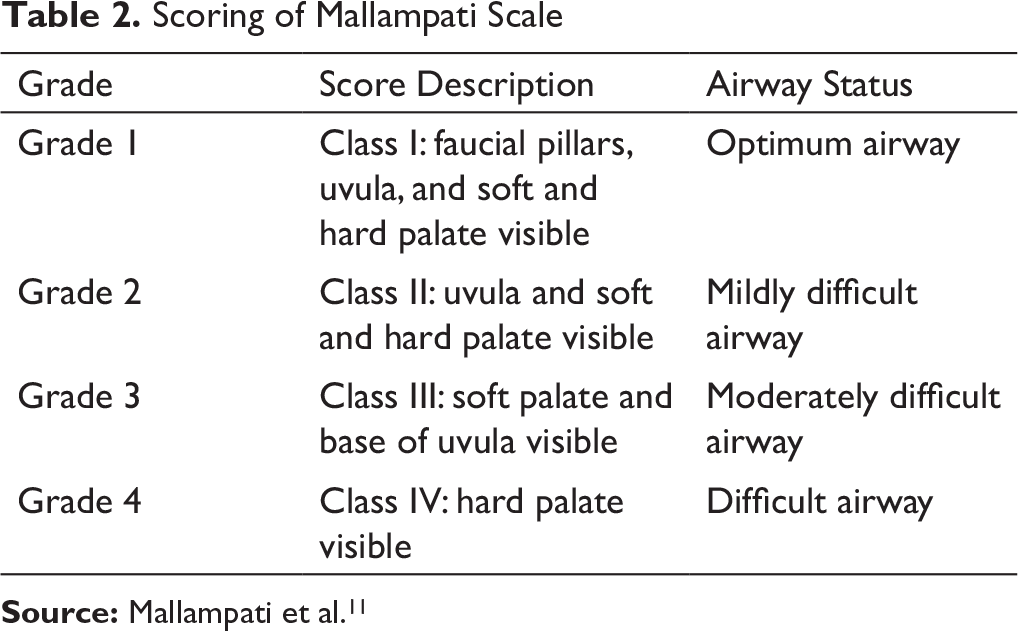
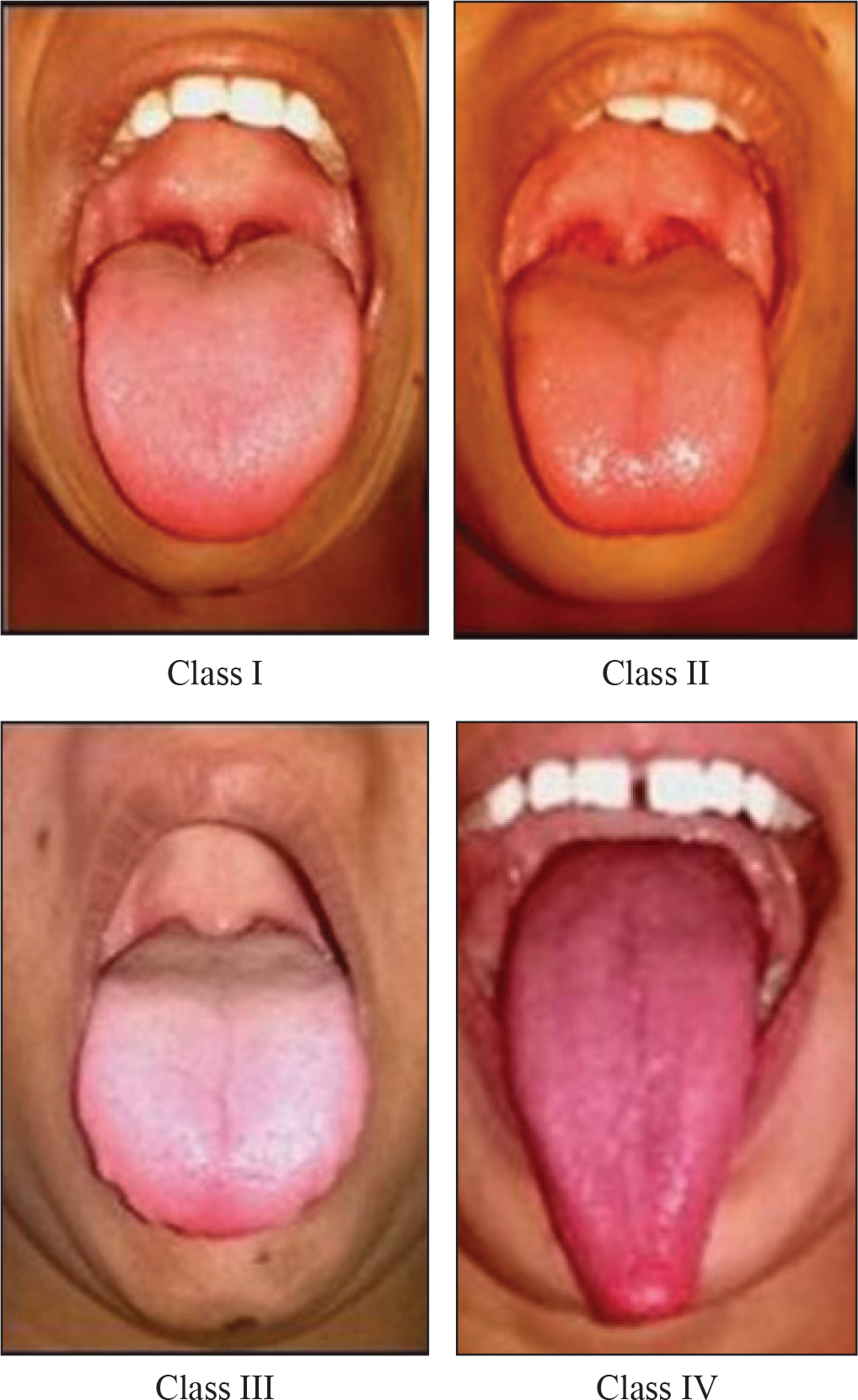
Evaluation of Tongue Position and Size Was Done Using Mallampati Scale 11
Scoring of Mallampati Scale
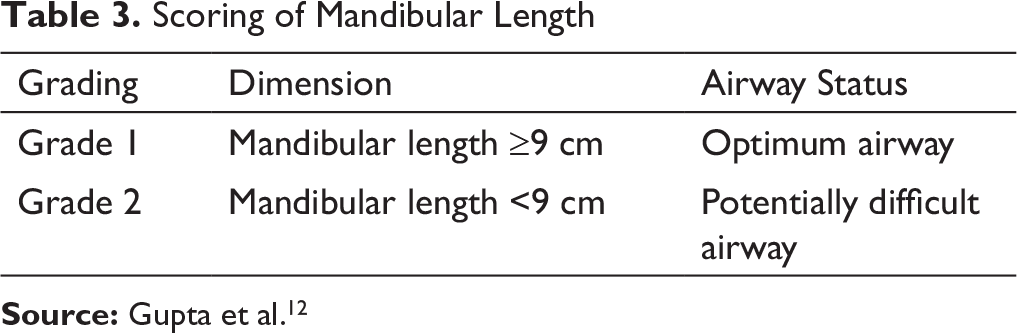
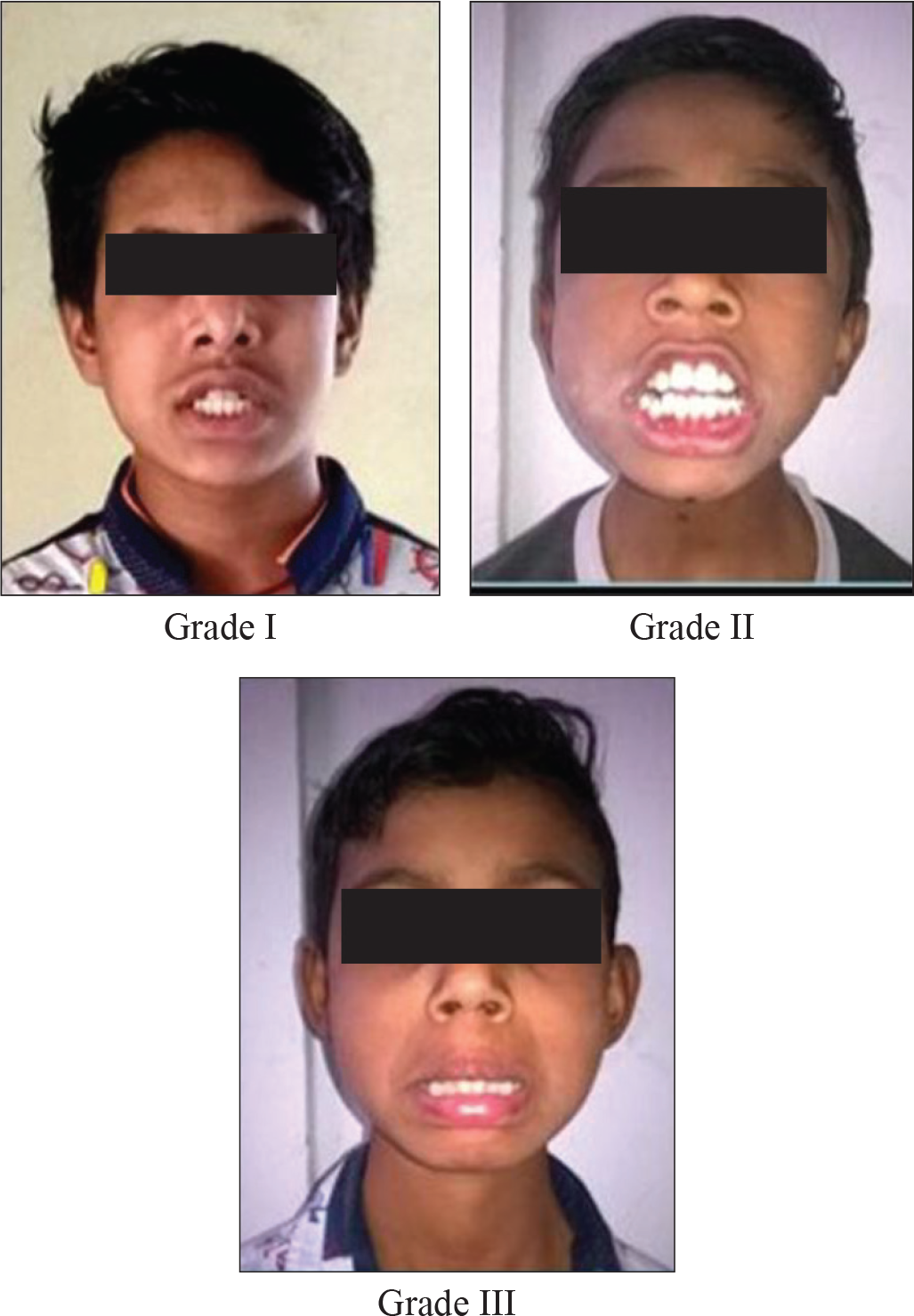
Evaluation of Mandibular Morphology Using Mandibular Length 12
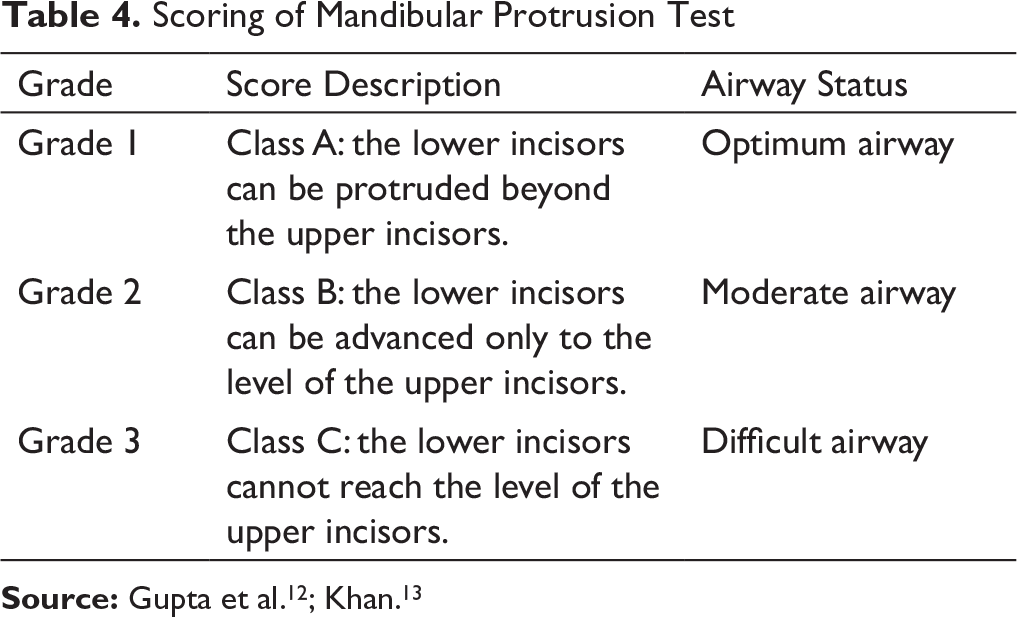
Mandibular Protrusion Test 12 or “Slux”/“Upper Lip Bite” Test 13
This test helps to evaluate the range of motion/movement of temporomandibular joint (TMJ) and analyze whether the mandibular retrusion was either due to distal location or due to small size. It was performed while assessing the temporomandibular function by asking the patient to advance the mandible as far as possible, and the grade was obtained as illustrated in Figure 6 and Table 4. If the patient is able to protrude the mandible only to the level of upper incisors, the cause of mandibular retrusion is forced posterior position. If he or she is unable to protrude to the level of upper incisors, it denotes small size of mandible as a causative factor for Class II malocclusion.


Scoring of Mandibular Protrusion Test
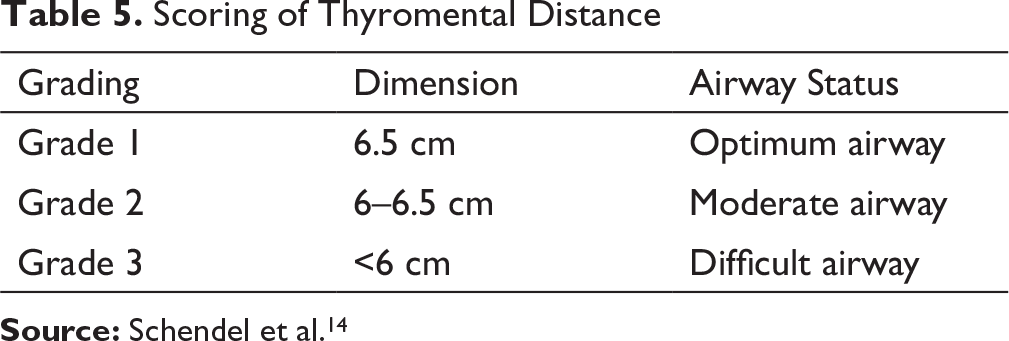
Assessment of Mandibular Space Using Thyromental Distance14.
Scoring of Thyromental Distance
Statistics
All the findings were tabulated and subjected to statistical analysis to determine their significance using software IBM SPSS version 17.0 and P < .05. Repeated measure ANOVA test was used for overall comparison of mean percentage adenoid wall area (Ad area), percentage air area, and upper pharyngeal airway. Chi-square test was applied for the following parameters: nasal competency test, Mallampati scale, ML, mandibular protrusion test, and thyromental distance.
Results
In the present study, we observed a significant positive correlation between grades of nasal competency and percentage adenoid wall area, which infers that the larger percentage adenoid wall area was correlated with poor nasal competency. Good nasal competency was associated with larger upper airway. There was a significant positive correlation between grades of nasal competency and grades of ML, grades of mandibular protrusion and grades of ML, grades of thyromental distance and both upper and lower airways, and grades of thyromental distance and grades of ML (Table 12).
Discussion
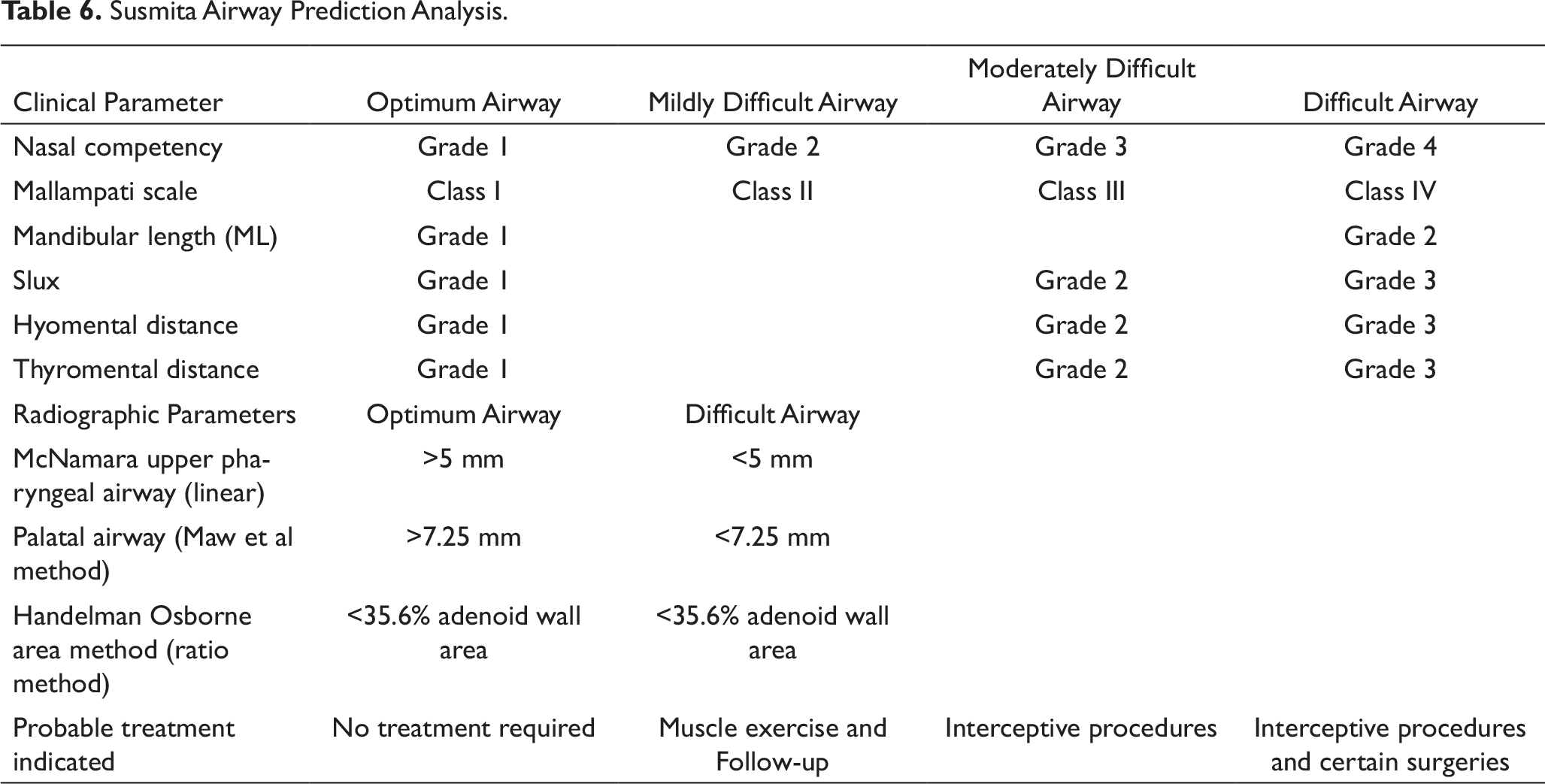
Susmita Airway Prediction Analysis.
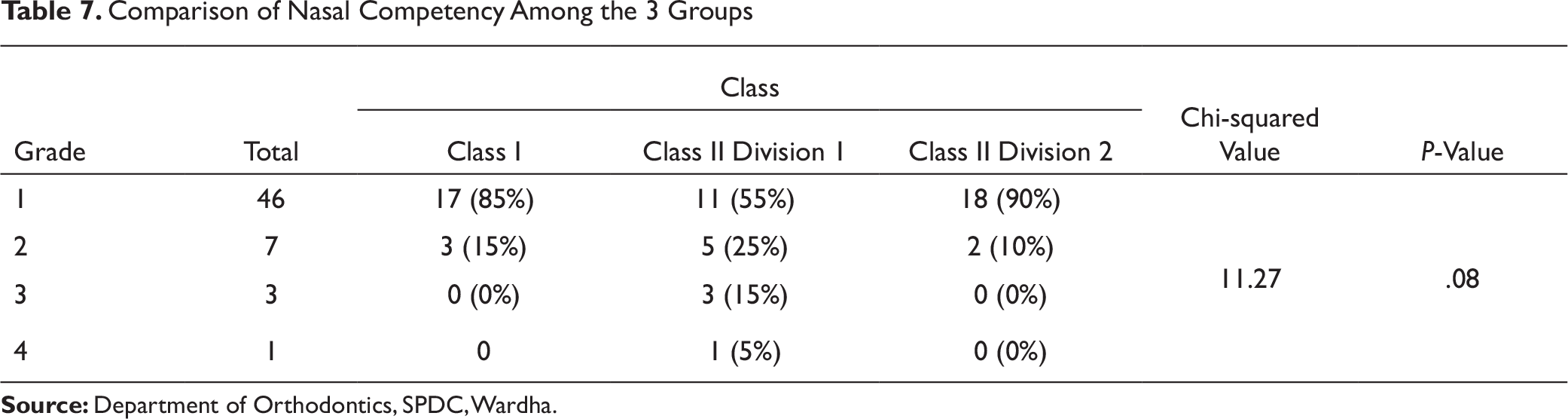
Subjects of age 15 to 18 years (mean age 16.5years) who satisfied the inclusion criteria were selected to observe airway differences in growing adolescents with different skeletal patterns. According to Schendel et al, the depth of upper pharyngeal airway increases with age. In the present study, most of the Class II Div 1 subjects had severe nasal obstruction and poor nasal competency 14 (Table 7). Nasal obstruction is one of the major etiologies of hyper divergent Class II Div 1 malocclusion pattern. Similar observations were obtained by Linder-Aronson 15 who had reported about the correlation between nasal resistance and increased mandibular plane angle. During mouth breathing, retroglossal airway is kept open by increased tonus of the suprahyoid muscles. The infrahyoid and post-vertebral muscles increase the tension to maintain a stable posture and often rotate the head upward and backward. The tongue is positioned lower. They had observed corrective structural changes after adenoidectomy in affected cases, such as increase in sagittal depth of nasopharynx and 4-degree reduction in mandibular plane angle. Lessa et al 16 had studied influence of mouth breathing on craniofacial development. They reported higher mandibular plane angle and vertical growth in mouth breathers. This was observed in our study also. 16
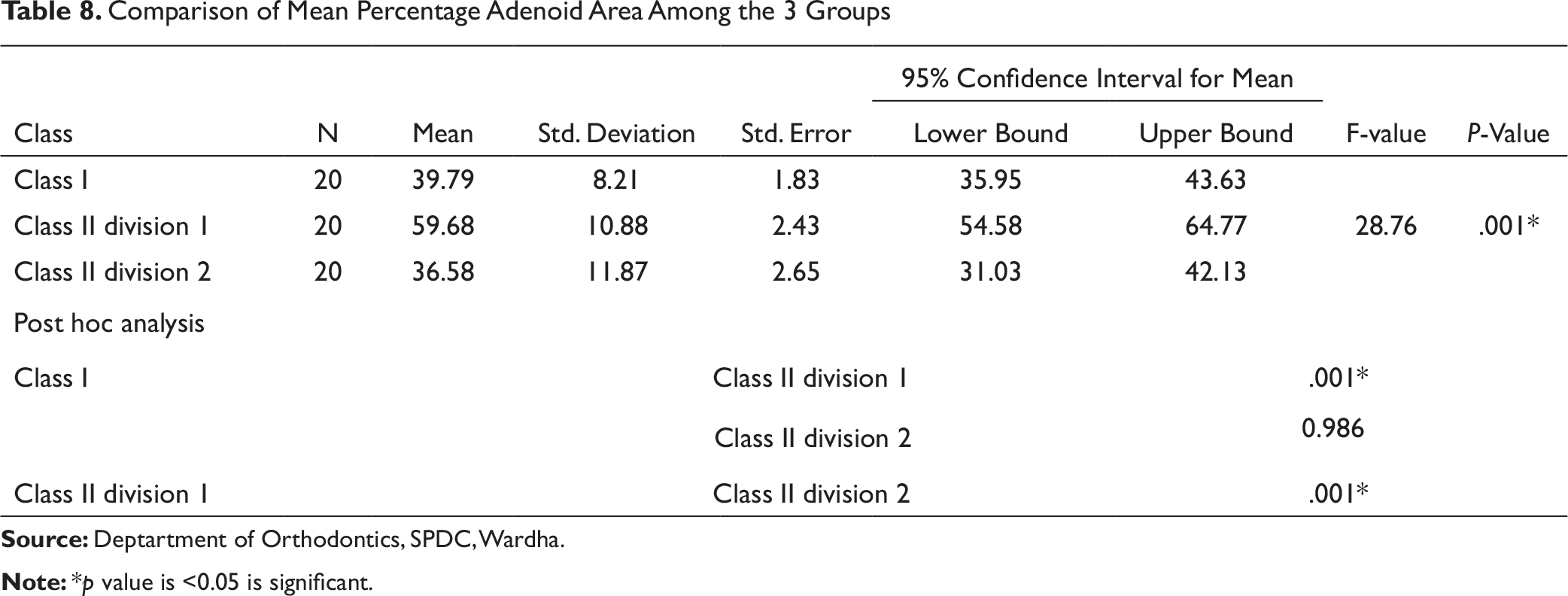
The percentage adenoid wall area was observed to be significantly highest in Class II Div 1 subjects among all groups (Table 8). The average values given by Handelman and Osborne 9 for percentage adenoid wall area at age 17 years 9 months were 35.6 ± 8.2 for males and 39.9 ± 11.3 for females, respectively. In our study, mean percentage adenoid wall area was observed to be higher (59.68±10.88) in Class II Div 1 cases, and equivalent percentage values were observed in Class I cases (39.79 ± 8.21). Adenoid vegetation is the most frequently quoted cause of airway obstruction. Persons with long face syndrome have smaller nasopharyngeal cavities; hence, even a small increase in adenoid bulk could easily cause airway obstruction. 8 Similar observations were made by Souki et al who had studied the prevalence of malocclusion among 401 Brazilian mouth breathing children of age 2 to 12 years. Adenoid/tonsil obstruction was detected in 71.8% of the children and was associated with Class II malocclusion and posterior crossbite. 17
Comparison of Nasal Competency Among the 3 Groups
Comparison of Mean Percentage Adenoid Area Among the 3 Groups
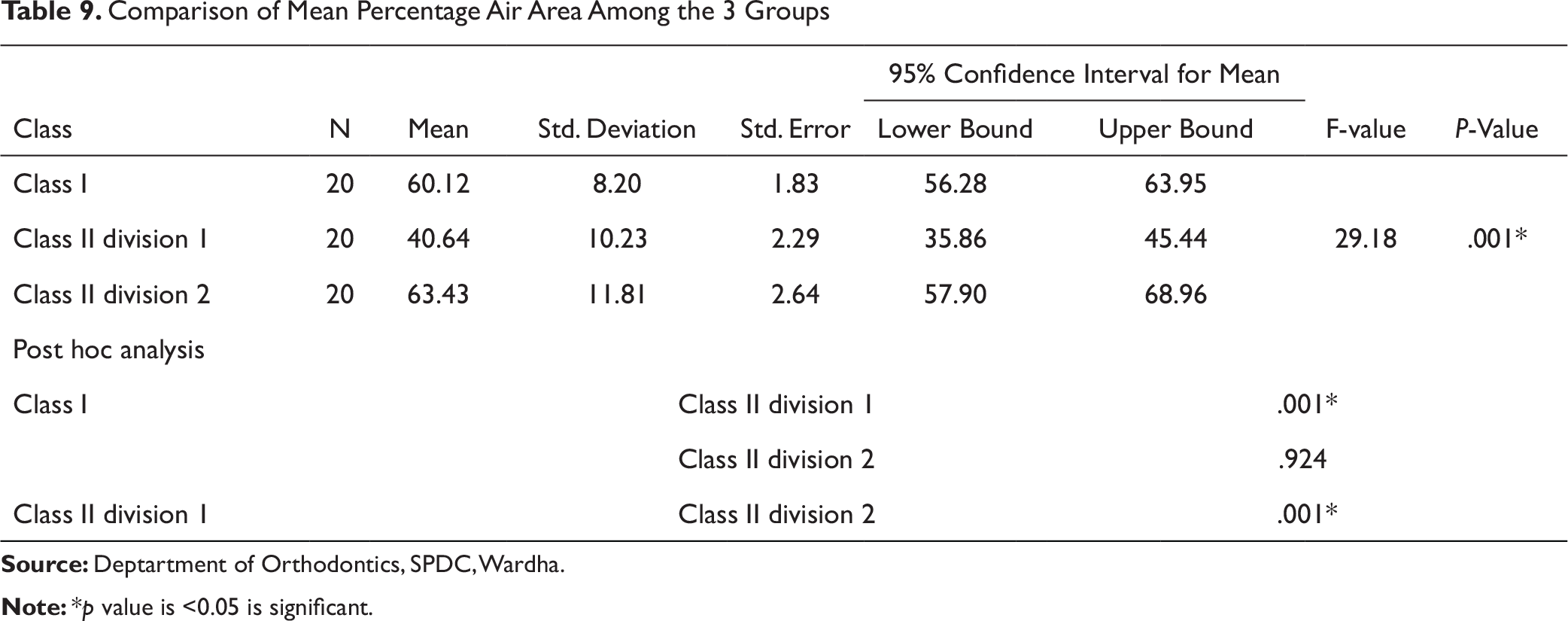
In this study, the mean percentage air area was significantly less in Class II Div 1 subjects compared to Class I and Class II Div 2 (Table 9). This might be attributed to larger percentage adenoid wall area. Handelman and Osborne 9 had found percentage air area in females of age 15 to 18 years was around 50%, while in males, it was 40%-70% in normal population. In our study, mean percentage air area in Class I cases was observed to be 60.12±8.20, which is in concordance with them. The findings of this study are similar to Feres et al 18 who had investigated adenoid hypertrophy and nasopharyngeal obstruction in 4 to 14-year-old children having nasal obstruction and history of mouth breathing. They observed mean percentage air area to be 36.80±10.75. In this study, Class II Div 1 cases had mean percentage air area of 40.64±10.23 for average age 16.5 years in a sample without history of mouth breathing.
Comparison of Mean Percentage Air Area Among the 3 Groups
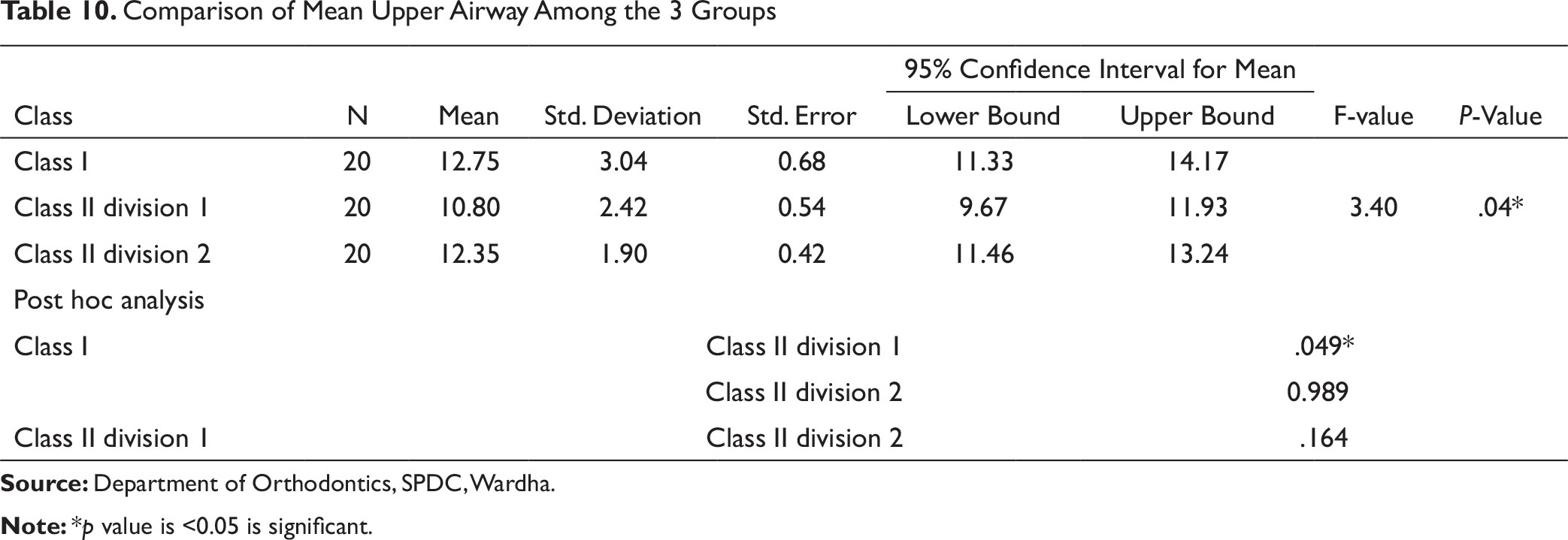
The present study showed that the Class II Div 1 subjects had significantly smaller upper airway compared to Class I (Table 10). This might be attributed to thinner nasopharyngeal airway and hyper divergent jaw bases in Class II Div 1 cases. Nanda et al 19 and Zheng et al 20 had also reported significant reduction in upper airway at the level of nasopharynx and oropharynx in Class II malocclusion cases compared to Class I and Class III cases.
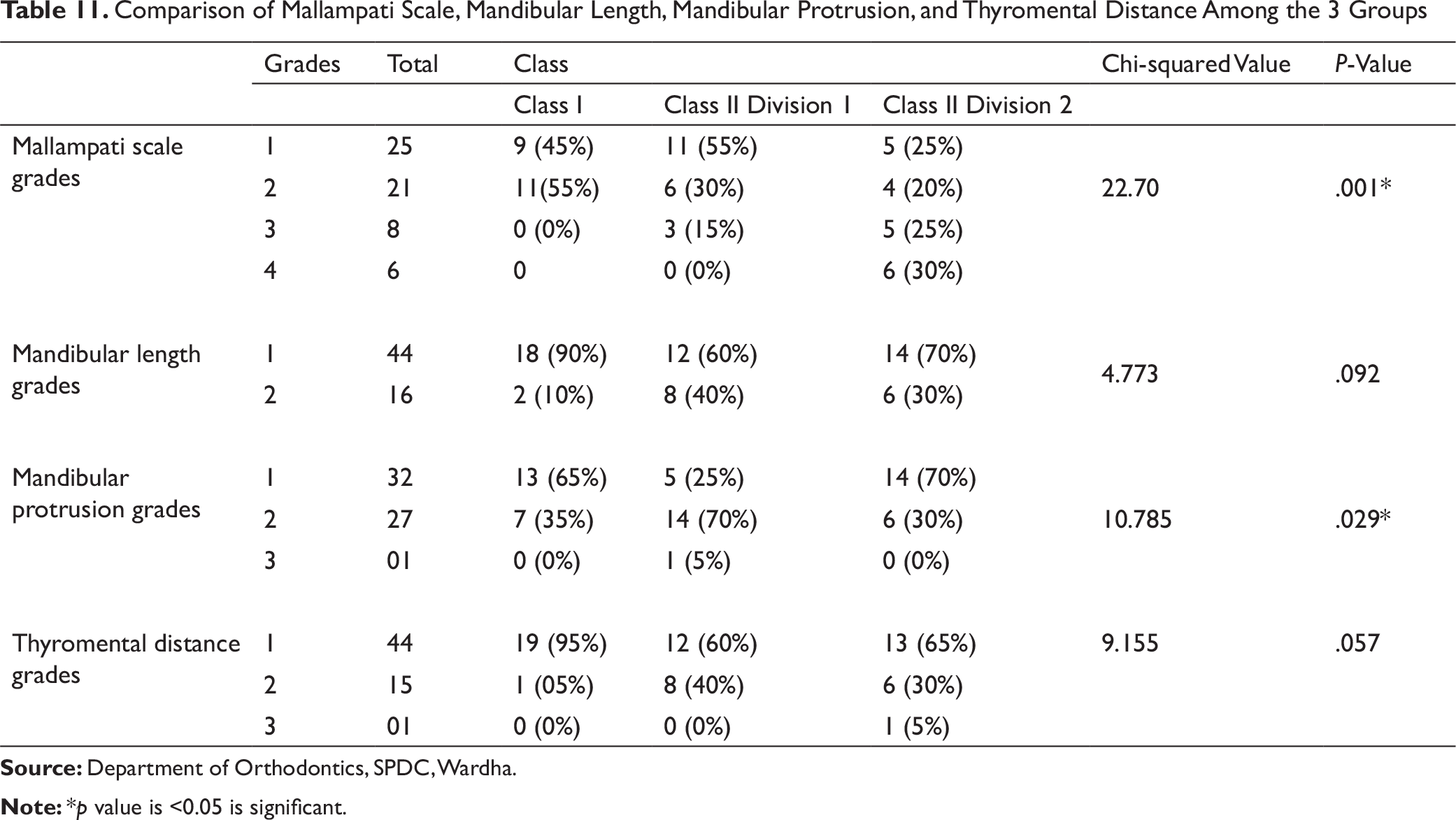
Tongue contributes to the airway obstruction due to its size and position. Only few methods are known in the literature for evaluation of tongue size and oropharynx. The present study evaluated the relationship between tongue morphology, its position, and other airway variables. Based on Mallampati scale, Class II Div 2 subjects had a significantly large tongue size causing difficult airway, which is attributed to hyperactive musculature (Table 11). Similar observations are made by Liistro et al 21 who had found a significant association between Mallampati score and apnea/hyperpnoea index and had concluded that a high Mallampati score represents a predisposing factor for obstructive sleep apnoea (OSA).
Comparison of Mean Upper Airway Among the 3 Groups
In the present study, a large number of Class I subjects had ML measurements suggestive of optimum airway. This might be because of normal functioning matrices (larger airway space). Class II Div 1 subjects had reduced ML due to reduced airway space and development of smaller size mandible (Table 11). Reduced ML was observed in Class II Div 2, which might be caused by distally locked mandible and inadequately expressed growth potential. Similar observations were made by Karm et al 22 who had found that the retrognathic patients with short ML had difficult airway.
In this study, mandibular protrusion test was done to evaluate range of movement of TMJ, which also helps to analyze mandibular retrusion either due to “Distal location” or “Small Size.” This test helps to assess neuromuscular role in mandibular protrusion. Class II Div 1 subjects had significant difficulty in mandibular protrusion compared to Class I and Class II Div 2 (see Table 11). This might be because of distal position, small size, as well as altered neuromuscular orientation and programming, which gets more aggravated with downward rotation of mandible. Similar observations were reported by Sahin et al 23 who had stated that the mandibular protrusion was the most sensitive test for predicting difficult airway. This information can be used to initiate interceptive measures where the neuromuscular response can be addressed so as to allow normal mandibular growth.
Comparison of Mallampati Scale, Mandibular Length, Mandibular Protrusion, and Thyromental Distance Among the 3 Groups
Correlations of Different Parameters
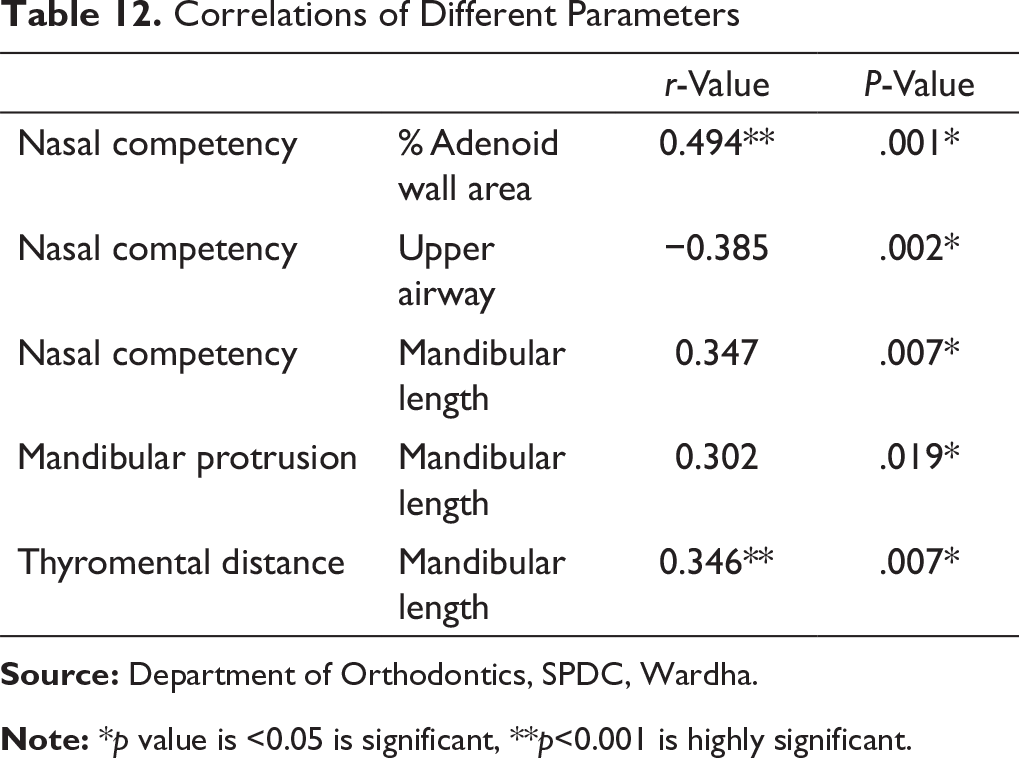
Note: *p value is <0.05 is significant, **p<0.001 is highly significant.
Clinical Implications
This study proposes an innovative clinical diagnostic protocol for airway evaluation which would be beneficial for orthodontists, pedodontists, and general dentists so that early diagnosis of cases of sleep disordered breathing (SDB), OSA, and respiratory syndrome can be done to carry out preventive, interceptive, and corrective measures to normalize optimum craniofacial development and general health.
Conclusion
It was concluded from this study that a diagnostic protocol which includes the “Predictors of Difficult Airways” will be helpful in early diagnosis and identification of potential risk factors that may cause “Breathing Disorder”-related malocclusions and later on increase the risk of developing OSA.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.