
Abstract
Introduction: Maxillary advancement (MA) with rigid external distraction (RED) to correct mid-face deficiency in adult cases with cleft lip and palate (CLP) may trigger velopharyngeal incompetency (VPI) post-surgically.
Aim and objectives: To determine pre-treatment factors affecting worsening of post-surgical VPI in patients with repaired unilateral CLP who underwent MA with RED.
Material and methods: Treatment records of 10 patients with unilateral CLP who underwent MA with RED were selected from institutional archives. All patients underwent clinical evaluation of velopharyngeal function at T1 (1 week before surgery) and T2 (3 months after surgery). Based on post-surgical VPI status, patients were divided into 2 groups: group 1 (no change in VPI) and group 2 (worsened VPI). Lateral cephalograms were manually traced at T1 and T2 to determine the changes in length of soft palate (LSP) and pharyngeal depth (PD) at T2. The information regarding amount of MA and presence of pre-surgical VPI was obtained from case sheets of patients.
Results: Mean LSP and PD at T2 were higher compared to T1 (p-value < .001). No significant difference was observed in mean pre-surgical age, gender, pre-surgical LSP, and pre-surgical PD between the study groups (p-value > .05 for all). The worsened VPI post-surgically was significantly associated with the presence of VPI pre-surgically and also with the amount of MA (p-value < .05 for both).
Conclusions: Amount of MA and presence of pre-surgical VPI are most important factors affecting post-surgical VPI. Prospective studies are recommended to validate the findings of this study.
Introduction
Background
Skeletal class III malocclusion is a common feature among patients with repaired cleft lip and palate (CLP). This skeletal deformity results from a deficient maxillary growth mainly in a transverse and sagittal direction. The fibrous scar resulting from repeated surgeries for lip and palate repair, alveolar grafting, etc., contribute to this deficient maxillary growth.1, 2 Studies indicate that about one-fourth of these patients require maxillary advancement (MA) surgery to restore favorable aesthetics and oropharyngeal functions.2, 3
Distraction osteogenesis (DO) with rigid external distraction (RED) and Le Fort I osteotomy are the commonly used procedures for MA in these cases. Apart from improving facial aesthetics, these procedures also alter the spatial relationship between pharyngeal hard and soft tissues.4, 5 Literature review indicates that MA by Le Fort I osteotomy of even 7 mm6 or 10 mm7 may trigger velopharyngeal incompetency (VPI) in such patients since the pharyngeal soft tissues get inadequate time to adapt and remodel themselves. The forward movement of hard palate brings soft palate along and results in increased separation from the posterior pharyngeal wall. This increased separation leads to a poor oropharyngo-nasal seal and hypernasality of voice.4, 8
Pre-distraction length of the soft palate (LSP) is an important criterion which determines VPI post MA in these cases. Literature suggests that among many factors which influence post-treatment VPI in patients with repaired cleft, the most important are amount of MA, presence of pre-treatment VPI, pre-treatment LSP, and pre-surgical pharyngeal depth (PD).8–10 Studies have shown that RED provides better adaptation and stability of soft tissues with reduced chances of VPI post treatment by virtue of distraction histiogenesis. But other studies have concluded deterioration of velopharyngeal function even after RED and a positive correlation has been observed between the amount of MA and increase in VPI.1, 8, 9 Recent Cochrane review concluded that the evidence comparing effectiveness of DO and conventional orthognathic surgery is of very low quality and further prospective studies with a larger sample size are required to confirm possible true differences between both interventions. 10
Literature is not consistent on the effect of MA on VPI and contradicting evidence has been reported. Therefore, this retrospective study was conducted to evaluate the same. This would assist the ortho-surgical team in predicting development of post-treatment VPI, deciding the type of surgery and need of alternate treatment plan to prevent worsening of VPI post-surgically.
Aim
The aim of this study was to determine factors affecting development of post-treatment VPI in patients with unilateral CLP treated with maxillary RED.
Objectives
The objectives were:
To determine changes in length of soft palate (LSP) and PD following maxillary distraction with RED. To ascertain the association of change in VPI post-surgically with age, gender, pre-treatment LSP, pre-surgical PD, presence of pre-surgical VPI and the amount of MA.
Material and Methods
Study Design
Retrospective study
Setting
This study was carried out on the patient archives at Department of Orthodontics and Dentofacial Orthopedics of a tertiary care post-graduate government teaching institute.
Participants
Treatment records of patients with unilateral CLP who underwent MA with RED were explored from departmental archive (period selected 2014–2019). Sample size for the study was 10 patients’ records and was calculated with 5 percent level of significance and 80 percent power to detect a clinically significant difference in the amount of MA. The final sample consisted of records of 6 male and 4 female patients who matched the inclusion criteria of this study.
Inclusion Criteria
Non syndromic patients with unilateral CLP.
Complete set of treatment records including medical case sheets.
Skeletally mature adult patients; age 15–25 years (CVMI [Cervical vertebrae maturation index] stage VI).
Skeletal class III malocclusion (maxillary deficiency) with ANB (Point A-Nasion-Point B angle) less than −4° and reverse overjet >2 mm.
Patients underwent MA with RED.
Good quality radiographs meeting the requirement of the study.
Exclusion Criteria
Syndromic patients.
Patients with systemic condition/disease affecting bone metabolism.
Incomplete records or poor quality/stained radiographs
Patients treated with Bi-jaw orthognatic surgery.
History of previous ortho-surgical treatment or trauma to jaw bones.
Variables
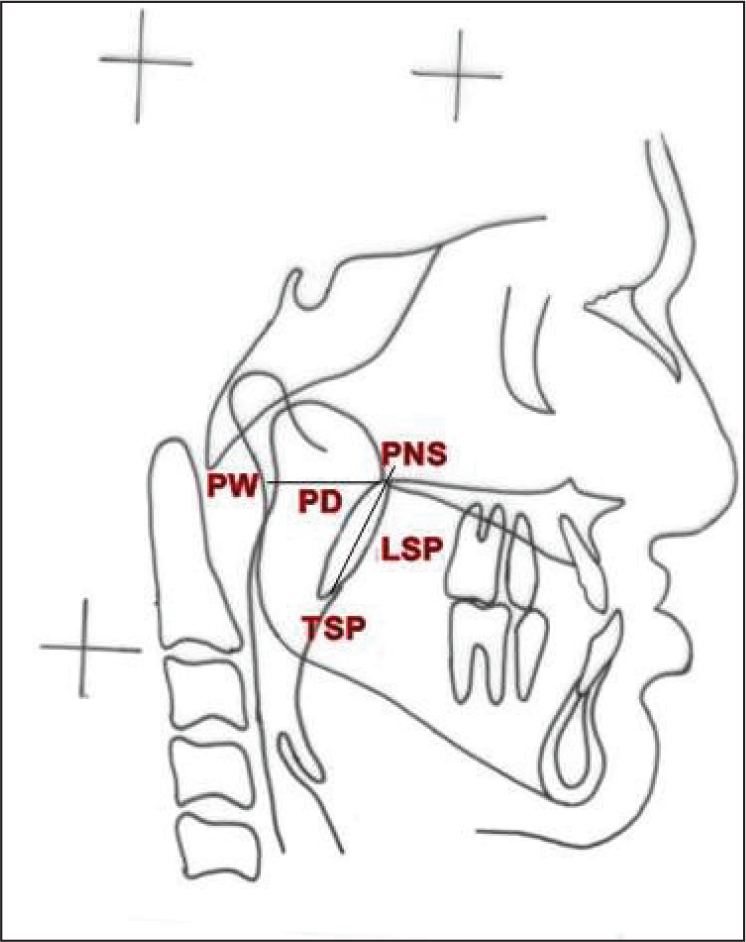
The variables measured were LSP (linear distance from posterior nasal spine [PNS] to tip of the soft palate [TSP]) and PD (linear distance from PNS to nearest pharyngeal wall) on the lateral cephalogram (Figure 1). The information regarding age, gender, amount of MA, and presence of pre-surgical VPI was obtained from the case sheets of the patients. The outcome variables recorded were change in LSP, PD, and VPI (ie, worsened VPI or no change in VPI) after MA.
Measurements on Lateral Cephalogram
Data Measurement
As an institutional protocol, the management of patients with CLP involves an interdisciplinary team. Initial evaluation of velopharyngeal dysfunction for all patients was done by the same speech pathologist. To grade VPI on a quantitative scale, Pittsburgh Weighted Speech Scale (PWSS) 11 was used which utilizes a uniform scoring system to evaluate and score a patient based on articulation, voice quality, nasal air emission, resonance, and facial grimace. The score was recorded at T1 (1 week before surgery) and T2 (3 months after surgery) and documented in the case sheets of the patients. The assessment of anatomical and functional bases for velopharyngeal function was ascertained with a fiberoptic nasoendoscope by the same team of otolaryngologists at T1 and T2.
Selected patients were treated with a standard protocol by the same ortho-surgical team on a comprehensive plan. MA was done with RED using titanium mini-plates and screws for anchorage. Distraction of the maxilla was initiated immediately after surgery at the rate of 0.5 mm twice/daily for all patients. Lateral cephalograms were recorded and traced manually at T1 and T2 to determine the changes in LSP and PD. Based on post-surgical (T2) VPI status, patients were divided into 2 groups:
Group 1: No change in VPI
Group 2: Worsened VPI
Bias
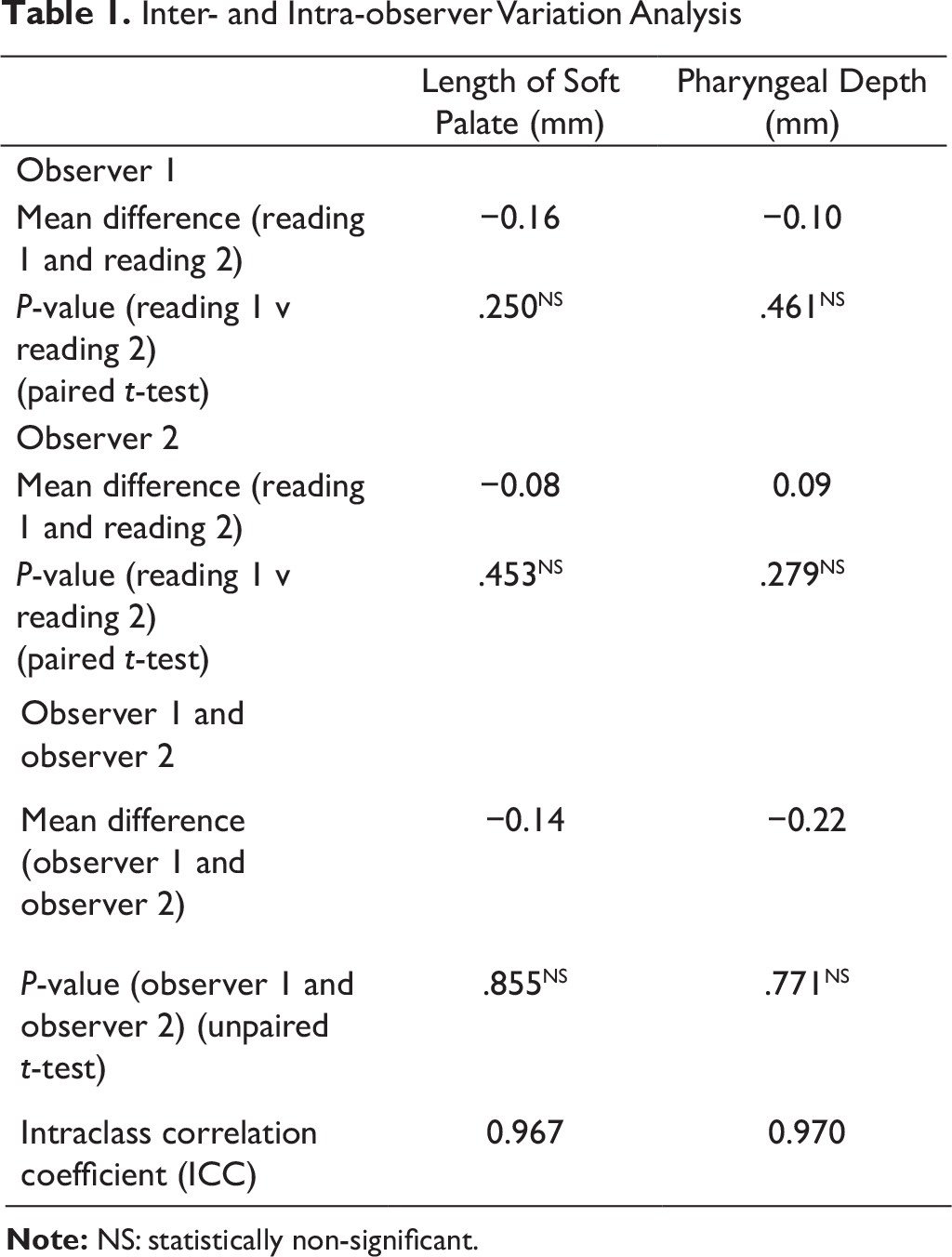
Five lateral cephalograms were retraced after a period of 1 week by the principal investigator (SSA) to ascertain intra-observer bias and also by a senior orthodontist (RM) to ascertain inter-observer bias.
Statistical Analysis
The data was compiled in MS Excel work sheets and subjected to statistical analysis. The data on categorical variables is presented as n (% of cases). The data on continuous variables is presented as mean ± standard deviation (SD). The statistical significance of difference of distribution of categorical variables across the study groups was tested using Fisher’s exact probability test. The statistical significance of difference of distribution of mean of continuous variables was tested using independent sample t-test. The statistical significance of difference (T1 versus T2) of distribution of means of continuous variables was tested using paired t-test. The underlying normality assumption is tested before subjecting the study variables to t-test.
P-values less than .05 were considered to be statistically significant. All the hypotheses were formulated by using 2-tailed alternatives against each null hypothesis (hypothesis of no difference). The entire data was statistically analyzed using statistical package for social sciences (SPSS version 21.0, IBM Corporation) for MS Windows.
Results
Intra- and Inter-observer Reliability
Inter- and Intra-observer Variation Analysis
Parameters Correlating with Post-surgical VPI
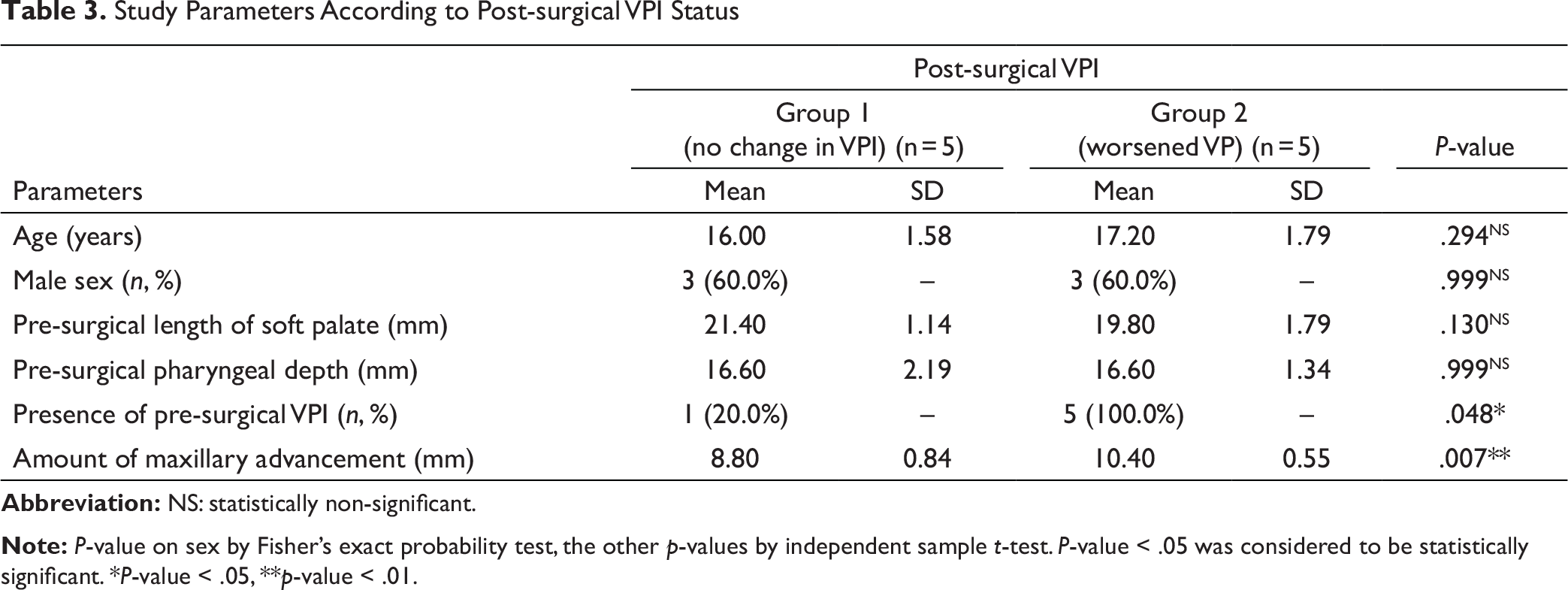
No statistically significant difference was observed in mean pre-surgical age, mean pre-surgical LSP, and mean pre-surgical PD among the study groups (p-value > .05 for all). No significant gender variation was observed between group of cases with no change in VPI and with worsened VPI (p-value > .05; Table 3).
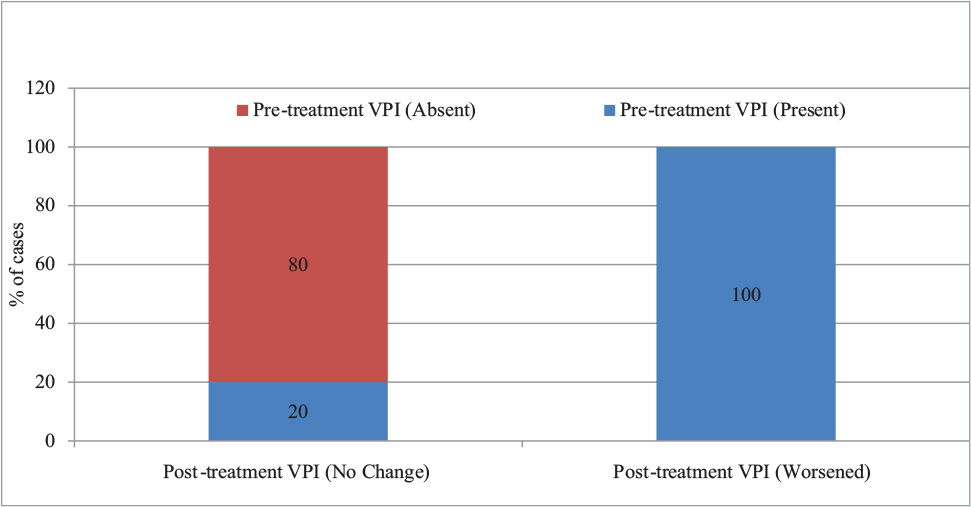
The worsened VPI post-surgically was significantly associated with the presence of VPI pre-surgically (p-value < .05).Out of 5 patients who had no change in VPI at T2, 1 (20.0%) had VPI at T1 and 4 (80.0%) did not have VPI at T1. Out of 5 patients who had worsened VPI at T2, all, that is, 5 (100.0%) had VPI at T1 (Table 3, Figure 3).
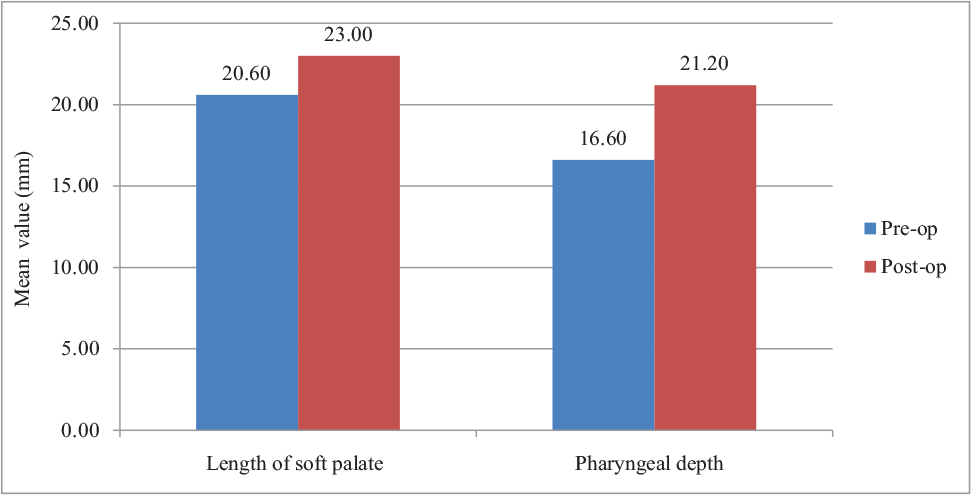
Pre- and Post-surgical LSP and PD
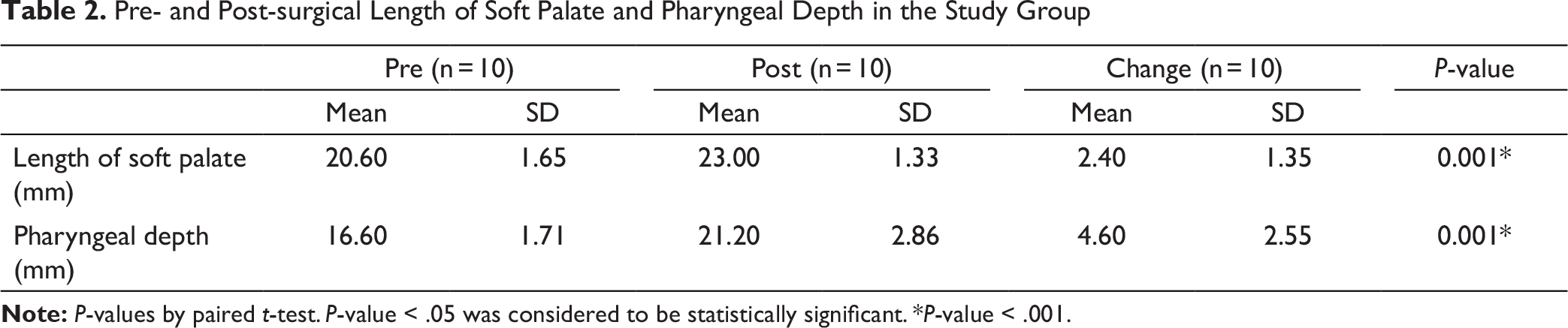
The mean LSP at T2 was significantly higher compared to mean LSP at T1 (p-value < .001). The mean increase in LSP at T2 was 2.40 mm (SD = 1.35 mm). The mean PD at T2 was significantly higher compared to mean PD at T1 (p-value < .001). The mean increase in PD at T2 was 4.60 mm (SD = 2.55 mm) (Table 2, Figure 2).
Pre- and Post-surgical Length of Soft Palate and Pharyngeal Depth in the Study Group
Study Parameters According to Post-surgical VPI Status
Pre- and Post-surgical Length of Soft Palate and Pharyngeal Depth in the Study Groups
Post-surgical VPI According to Pre-surgical VPI Status
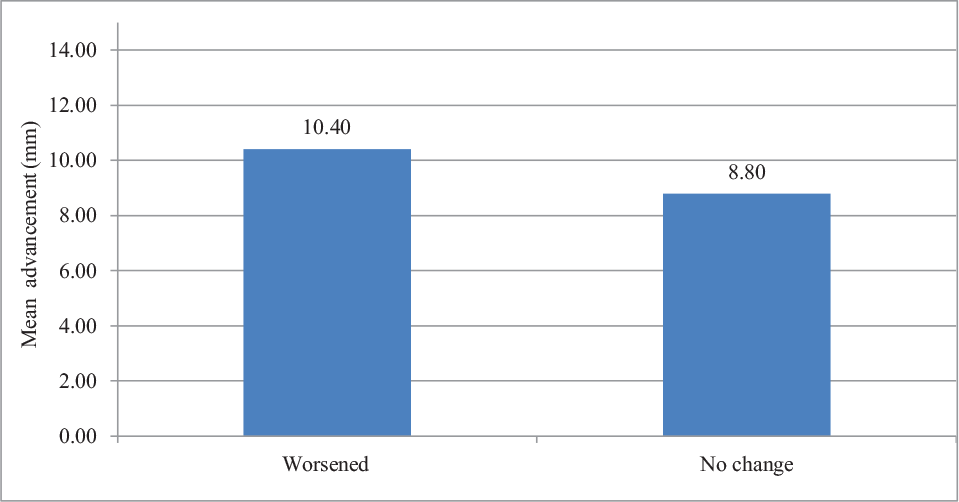
Post-surgical VPI According to Mean Maxillary Advancement
Discussion
Pre-surgical evaluation of velopharyngeal function is an integral part of diagnosis and treatment planning for patients with CLP. Naso-endoscopic evaluation assists in ascertaining the overall anatomy and physiology of the pharyngeal tissues. Pre-treatment speech assessment for hypernasality, nasal emission, and articulation is done by a speech pathologist. Clinical speech evaluation also suffices to ascertain VPI in these patients.8, 11 However, the quantitative assessment to grade VPI can be done with PWSS. PWSS utilizes a standardized scoring system to evaluate a patient based on nasal air emission, resonance, voice quality, articulation, and facial grimace. The individual scores of above parameters are summed up and the total scores are used to categorize patients into 1 of the 4 categories of velopharyngeal function as: competence, borderline competence, borderline incompetence, and incompetence. The same scale was used in the present study. 11
Studies have shown that soft palate which is smaller in dimensions, is stretched more with lesser remodeling after MA and predisposes a patient to higher chances of VPI post surgery. Assessment of antero-posterior dimension (depth) of pharynx pre-surgically can be used as a predictor for post advancement VPI. Patients with greater PD are at greater risk for development of VPI post-surgically.8, 10 In the present study, both LSP and PD dimensions showed a significant increase following RED at T2. However, pre-surgical LSP and PD dimensions were not significantly associated with development of VPI at T2. These findings disagree with some earlier studies in literature8, 11–13 that reported lesser LSP and higher PD dimensions pre-surgically as an important determinants in development of post-surgical VPI. Our study is in agreement with a study which found no correlation between pre-surgical VPI and PD and worsening of VPI post treatment. 14
Most studies in the literature are in agreement that presence of pre-surgical VPI in patients with CLP poses a greater risk of worsening of velopharyngeal function post MA,15–17 due to poor remodeling and adaptation of soft tissues with pre-existing surgical scars. It was hypothesized that by incremental advancement at 1 mm/day, the oropharyngeal tissues get sufficient time to adapt and hence there is no worsening of VPI post MA. 14 The present study is in agreement with these findings as a significant association was observed between worsening of post-surgical VPI and presence of pre-surgical VPI. However, contradicting to other studies which observed no association between pre- and post-surgical VPI in patients with CLP.18, 19
A forward distraction of hard palate during MA moves the soft palate along and disturbs the velopharyngeal seal, causes VPI and hypernasality of voice. Studies have shown that advancement as less as 4 mm20 or 7 mm6 can cause deterioration of speech and velopharyngeal function and may require post-surgical pharyngoplasty. These findings are similar in our study wherein a significant association was observed between amount of MA and worsening of VPI post-surgically. Our findings are contrary to Chanchareonsook 21 who concluded that a shorter LSP and larger PD pre-surgically are better predictors of post-surgical worsening of VPI than the quantum of MA. Various authors have emphasized the need of adjunctive procedures such as pharyngoplasty and pharyngeal flaps after MA to improve worsened speech post MA in patients with CLP.1, 8
Limitations
The present study is a retrospective study. A prospective study would be more desirable to conclude the research question. 3D modalities like cone beam computed tomography (CBCT) and magnetic resonance imaging (MRI) would provide more accurate assessment of the hard and soft tissues required over 2D modality (lateral cephalogram) used in this study, as the later has its own limitations.
Conclusions
Interpretation
A comprehensive evaluation of pre-treatment and prediction of post-treatment velopharyngeal function is an important aspect during diagnosis and treatment planning for patients with CLP requiring MA. Among various factors studied affecting VPI post RED MA, most contributing are amount of MA and presence of pre-surgical VPI. Other factors like LSP, PD, age, and gender were not statistically associated with development of post-surgical VPI in the present study, but their importance cannot be clinically ruled out unless prospective studies with a larger sample size validate these findings. The consideration of pre-surgical factors mentioned in this study should be emphasized at diagnosis and treatment planning stage, and alternate modalities like pharyngoplasty and pharyngeal flap procedures may be considered to prevent adverse effects on speech.
Generalizability
Prospective studies with a larger sample size are recommended to validate the findings of this study. However, the results of this study may act as a base line for further studies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval obtained from Institutional Ethical Committee.