
Abstract
ABSTRACT
Introduction: Finding a method to decrease orthodontic treatment time has been a concern for several authors. This study evaluated, clinically and radiographically, the influence of low-level laser therapy on the rate of orthodontic movement and dental tissue integrity.
Methods: The sample included 11 individuals with class I malocclusion, requiring extraction of 4 first premolars. Gallium aluminum arsenide diode laser with a wavelength of 780 nm was used once a month during retraction mechanics, to irradiate the maxillary and mandibular canines on one side and compare them with the nonirradiated contralateral side, after spring activation, until canine retraction was completed. This was followed by movement measurement. Periapical radiographs were used to check for possible modifications in the supporting tissues and root surface of the displaced canines.
Results: No differences in the rate of tooth movement were found between the irradiated and nonirradiated side on both dental arches. There was no resorption of the root and/or alveolar bone crest, maintaining the integrity of these tissues.
Conclusions: Low-level laser therapy did not promote an increment on the rate of tooth movement and did not cause greater root and alveolar bone crest resorption than on the nonirradiated side with the used protocol.
Introduction
Orthodontic therapy is a procedure that requires from 2 to 3 years to be completed. During this time, some side effects are involved in orthodontic mechanics such as root resorption, patient discomfort, gingival inflammation, enamel decalcification, and periodontal diseases.1-3 Consequently, it is desired to find a method to decrease treatment time and minimize the undesirable side effects. However, to decrease treatment time, it is necessary to increase the rate of tooth movement and to speed up the process of bone remodeling without causing damages to the periodontium and the teeth, or great discomfort to the patient.
Many authors have performed studies evaluating the influence of several methods in the acceleration of dental movement. These methods include injections of several substances, such as prostaglandins, vitamin D, and hormones, including thyroxine and nitric oxide. External electrical stimulus and surgical procedures, including dental distraction and alveolar corticotomies have also been used. These stimulants act by mediating the factors involved in bone remodeling, recruiting cells, and differentiating them into mature osteoclasts to accelerate bone resorption.4-8 One of the most accepted methods that demonstrate optimal results is local micro-osteoperforation. It works by recruiting precursor cells and stimulates its differentiation into osteoclasts, through increase of cytokines and chemokines.9, 10 Although these procedures increase the speed of orthodontic movement, they may cause discomfort to the patient, pain, and other side effects on alveolar bone and root integrity. Micro-osteoperforation could be painful or be rejected by patients because its traumatic characteristic. Injected substances and electrical stimulus could have unknown effects, cause inflammation, or may not be used in systemically compromised patients or under medical treatment. 11 Since these problems impair the use of these procedures it is necessary to search for methods with minimum side effects. Low-level laser therapy is an uncomplicated approach for accelerating tooth movement. It is simple, local, quick, and painless.12-17
The term “laser” is the acronym for “light amplification by stimulated emission of radiation.” This type of radiation is different from others. Its characteristics allow light to emit a unique color, with the same wavelength, giving it the ability to focus on a single point, and project over long distances without dispersing. This makes it useful for dental practice. Reports have confirmed the acceleration of dental movement by application of low intensity lasers, called “low-level laser therapy.” 12 After the cells absorb it, a chain of chemical reactions is produced within the cells, speeding up some metabolic process and slowing down others, promoting reduction of inflammation and increasing bone remodeling without generating discomfort to the patient.15, 18, 19
Studies have shown the low intensity laser efficiency in acceleration of bone turnover, and the consequent reduction in treatment time. However, the protocols used in these studies suggest laser application for several times in the same month, to obtain the desired results. This represents weekly appointments and a disadvantage when compared to the monthly appointments protocol normally used by orthodontists.12-14, 20, 21
Therefore, the aim of this study is to evaluate, clinically and radiographically, the influence of low-level laser therapy on the rate of orthodontic movement and tissue integrity of the alveolar bone crest and canine root, during initial canine retraction, using a single monthly dose and specific protocols for the mandible and the maxilla.
Material and Methods
The research material was used after approval by the Ethics and Research Committee of the Bauru Dental School, University of São Paulo, under the protocol number 009/2012, on March 28, 2012.
Patient Selection
This was a randomized, double-blind, placebo-controlled, parallel-group study. The sample included 11 individuals (4 females; 7 males) with a mean age of 14.04 years. The selection criteria included the following: patients presenting with class I malocclusions treated with extraction of maxillary and mandibular first premolars; presence of all permanent teeth except the third molars; absence of previous orthodontic treatment, absence of periodontal disease, systemic diseases, tooth agenesis, supernumerary or impacted teeth, within an age range between 12 and 17 years. Before beginning, each legal representative signed an informed consent.
Sample size calculation was performed using an alpha error of 5%, and a beta error of 20% to detect a minimum difference of 1.20 mm, with a standard deviation of 0.84.12, 13 The result indicated that a minimum of 9 patients were necessary. Therefore, 11 patients were selected.
Orthodontic Treatment
Premolar extractions were performed with a week interval on each side, always starting with the right side. After the extractions, a transpalatal and lingual arch were installed, followed by fixed appliances bonding (0.022 x 0.028-inch metallic Roth prescription brackets) on the canines and second premolars. Passive stainless-steel 0.018-inch archwires with a U bend in the extraction area were placed to maintain the extraction spaces.
Initial canine retraction was initiated 30 days after the last extraction, using nickel-titanium (NiTi) closed-coil springs with 12 mm length at first, activated to deliver 150 gm forces, measured with a tension gauge (ORMCO). The passive 0.018-inch stainless steel archwires were removed and segmented 0.014-inch cinched-back NiTi archwires were placed during this stage. The springs were activated every 30 days, for 3 months, with the same amount of force. The first application of low-level laser therapy was performed at this stage, along with the first clinical measurement.
Laser Application
The twin laser, a Gallium aluminum arsenide (GaAlAs) diode laser of low intensity, was used emitting light at 780 nm, in a continuous-wave mode. The beam spot size was of 0.04 cm
2
. The application protocol was different for the maxilla and the mandible, according to the following dosimetry:
Mandible: Output power of 40 mW; dose (energy density) of 10 J/cm
2
; exposure time of 10 s; 0.4 J of energy by point. A total of 10 irradiations were carried out each time, 5 on each buccal and lingual side. The total energy application was of 4 J around the mandibular canine roots. Maxillary buccal side: Output power of 40 mW; dose of 10 J/cm
2
; exposure time of 10 s; 0.4 J of energy by point. A total of 5 irradiations were carried out each time. The total energy application was of 2 J. Maxillary palatal side: Output power of 70 mW; dose of 35 J/cm
2
; exposure time of 20 s; 1.4 J of energy by point. A total of 5 irradiations were carried out each time. The total energy application was of 7 J; a total of 9 J around the maxillary canine roots.
Once a month, after spring activation, only 1 randomly selected canine was irradiated, both in the maxilla and mandible, representing the experimental group. The irradiated mandibular side was the opposite of the maxillary arch. The canines of the nonirradiated contralateral sides were used as controls. The irradiated canines were randomly chosen. On the control canines a simulation of irradiation was performed; thus. the patient would not know which canine was irradiated.
All irradiations were performed by a single operator (JMS) distributed as follows (Figure 1): mesiolabial marginal gingiva; distobuccal marginal gingiva; a central point in the tooth root; at a distance of 8 mm from point 1 in apical direction; at a distance of 8 mm from point 2 in apical direction.
Laser therapy ended after 90 days of the initial irradiation. Orthodontic treatment time was of 24 months (±6 SD).
Retraction Speed
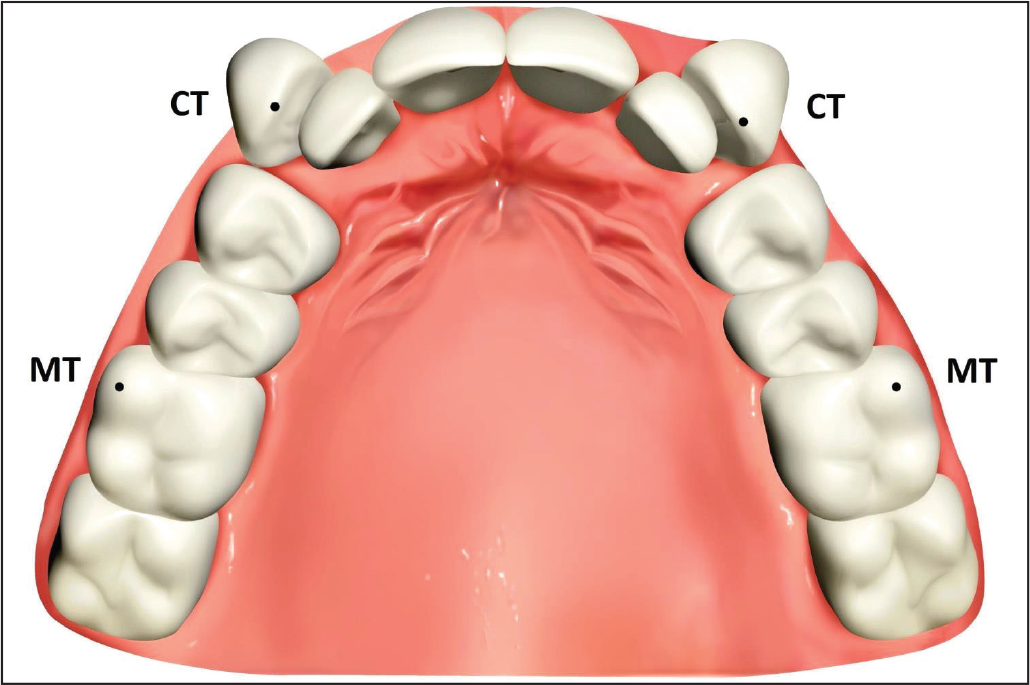
The amount of movement was measured by means of a digital caliper with an accuracy of 0.01 mm, sequentially, “in loco,” at the initial activation (T1), and after 30 (T2), 60 (T3), and 90 (T4) days. The amount of movement was represented by the distance between the canine (CT) and molar cusp tips (MT), respectively (Figure 2). In case of tooth wear, the mean portion of the wear was used. All measurements were made in millimeters by another examiner (SCCP), different from who performed the irradiations. This allowed a double-blind study. Each measurement was obtained 3 times, after 30, 60, and 90 days from the first irradiation.12, 22 The amount of canine movement was evaluated in 3 periods T1-T2, T2-T3, and T3-T4.
Buccal and Palatal Laser Application, Perpendicular and in Contact With the Gingival Tissue, on a Clean and Dry Surface. On the Left Side, the Buccal Central Root Point (BCP) and on the Right Side, the Palatal Central Root Point (PCP) Are Identified.

Periapical Radiographs
Forty-four periapical radiographs of the maxillary and mandibular canines on both sides, (E-speed Film, Eastman Kodak Company, Rochester, E.U.A), were taken prior to the initial activation and other 44 radiographs were taken 90 days after (T4) by the same operator.
The x-ray machine was the Gnatus, XR6010 model, operating with 70 kVp, 7 ma, focal distance of 30 cm and 0.5 second of exposure.
Reference Points to Measure the Amount of Retraction: Cusp Tip of the Canine (CT) and Mesiobuccal Cusp Tip of the First Molar (MT).
Radiographic Evaluation
Radiographic evaluation was performed by indirect digital reading. The radiographs were scanned (Microtek-Scan Maker i800) at 300 dots per inch (dpi) resolution, in a scale of 256 shades of gray and at a ratio of 1:1 (100%). The program used in the analysis and measurement of the images was the 3D Dolphin software (version 11.5 Chatsworth, California, USA).
Alveolar Bone Crest Height Evaluation
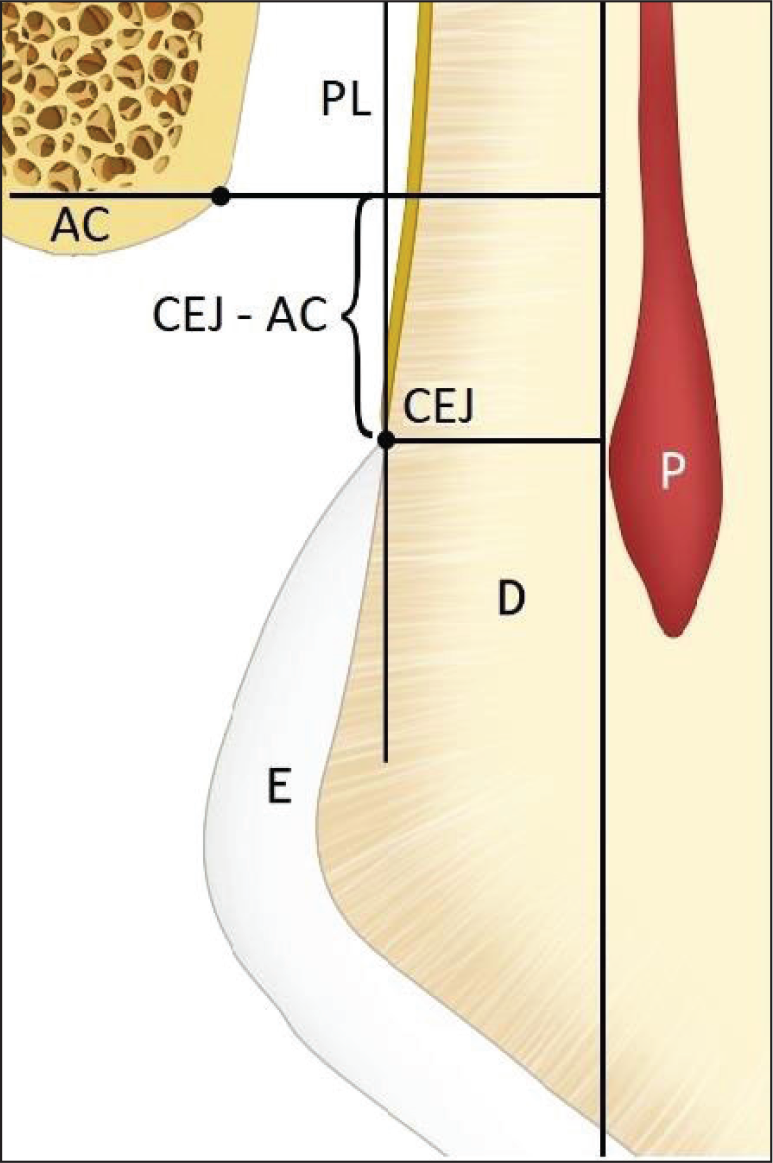
To assess the amount of resorption of the alveolar bone crest, the distance from the alveolar bone crest (AC) to the cemento-enamel junction (CEJ) was measured, parallel to the long axis of the tooth, both on the mesial and distal surfaces of the retracted canines (Figure 3). The AC point was defined as the bone crest most coronal point, with less bone tissue, where the periodontal ligament space remains constant. 23 The CEJ point was defined as the point located at the cementoenamel junction. After retraction, the alveolar bone crest height was measured, searching for possible modifications, and classified into 2 categories: CEJ-AC distance greater than 2 mm would be classified as periodontal aggression and values smaller than 2 mm, as periodontal health. 23
Schematic Representation of the Evaluated Areas: E, Enamel; D, Dentin; P, Pulp; PL, Periodontal Ligament; AC, Alveolar Bone Crest; CEJ, Cemento-enamel Junction; JCE-CA, Alveolar Bone Crest Height.
Root Resorption Evaluation
The classification of root resorption levels, suggested by Levander and Malmgren,
24
was used. Initial and final periapical radiographs were evaluated. The initial radiograph was used to evaluate whether there was no previous resorption. The irradiated was compared to the contralateral side. For classification, the following scores were ascribed:
0—absence of resorption; 1—minimum resorption, with irregular apical contour; 2—moderate resorption, less than 2 mm; 3—pronounced resorption, up to 1/3 of root length; 4—severe resorption, greater than 1/3 of the root.
Error of the Method
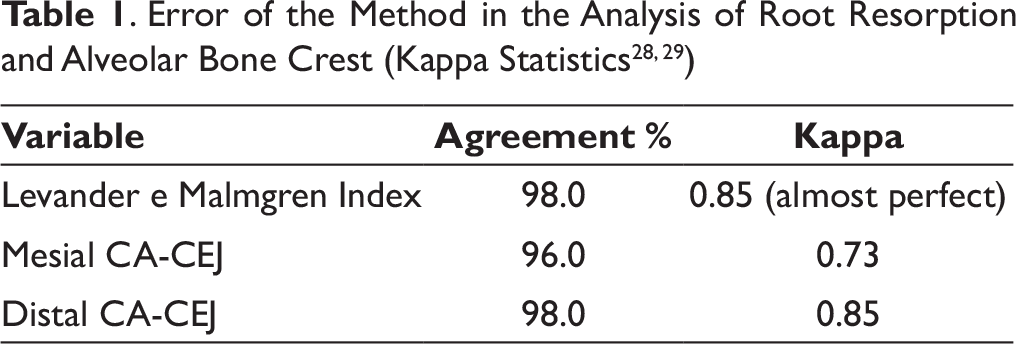
A month after the first measurements, 7 radiographs were randomly selected, and had root resorption and alveolar bone crest heights remeasured by the same examiner (SCCP). Intraexaminer reproducibility of root resorption and alveolar bone crest height measurements between double evaluations by the same examiner was calculated with Kappa statistics. 25
Statistical Analyses
To evaluate whether the tooth movement variables presented normal distribution, Kolmogorov-Smirnov tests were used. All variables were normally distributed. Therefore, comparison of tooth movement amount between the irradiated and nonirradiated sides and between the evaluated periods was performed with repeated measures ANOVA, followed by the Tukey tests.
To compare the amount of root resorption and the alveolar bone crest height between the irradiated and nonirradiated sides, Wilcoxon tests were used.
The statistical tests were performed with Statistical software (Statistical for Windows 7; Statsoft, Tulsa, Oklahoma, USA). Results were considered significant at P < .05.
Results
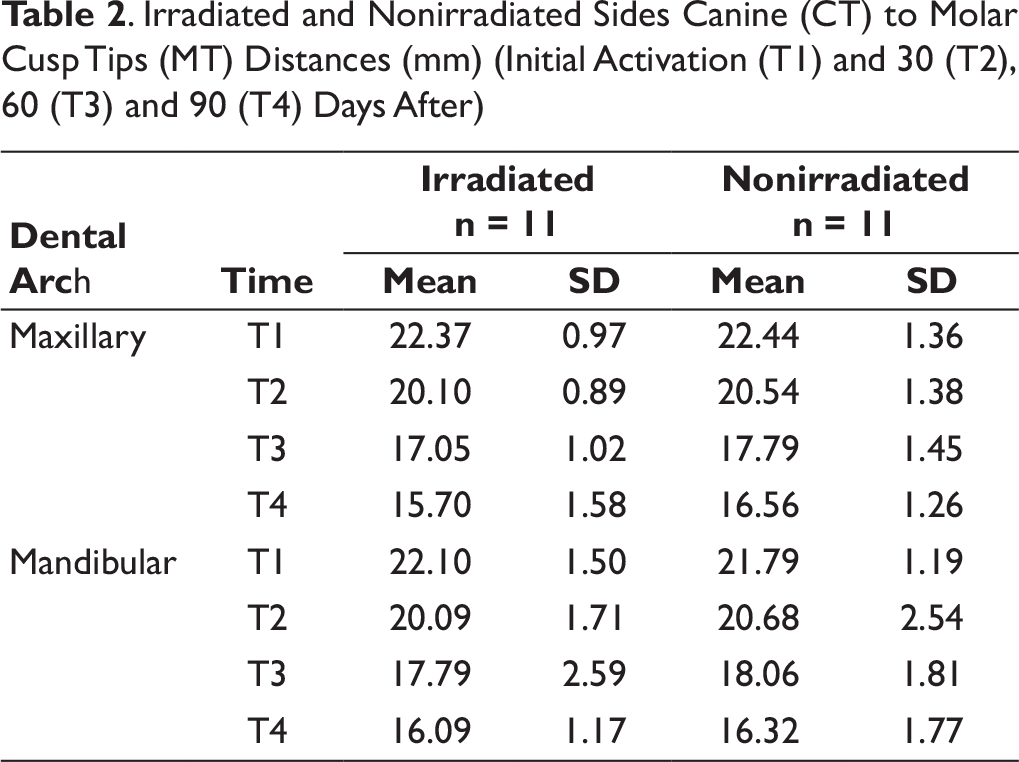
. Irradiated and Nonirradiated Sides Canine (CT) to Molar Cusp Tips (MT) Distances (mm) (Initial Activation (T1) and 30 (T2), 60 (T3) and 90 (T4) Days After)
Maxillary Arch Tooth Movement Amount Comparison Between the Irradiated and Nonirradiated Sides and Between the evaluated periods (Repeated Measures One-way ANOVA, Followed by the Tukey Tests)
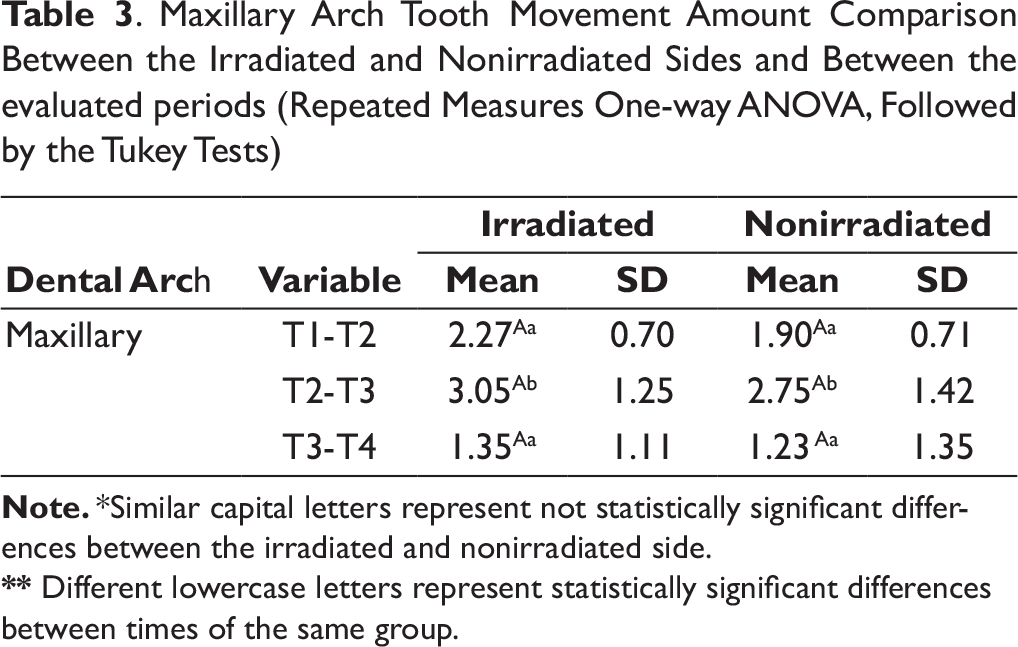
**Different lowercase letters represent statistically significant differences between times of the same group.
Mandibular Arch Tooth Movement Amount Comparison Between the Irradiated and Nonirradiated Sides and Between the Evaluated Periods (Repeated Measures One-way ANOVA, Followed by the Tukey Tests)
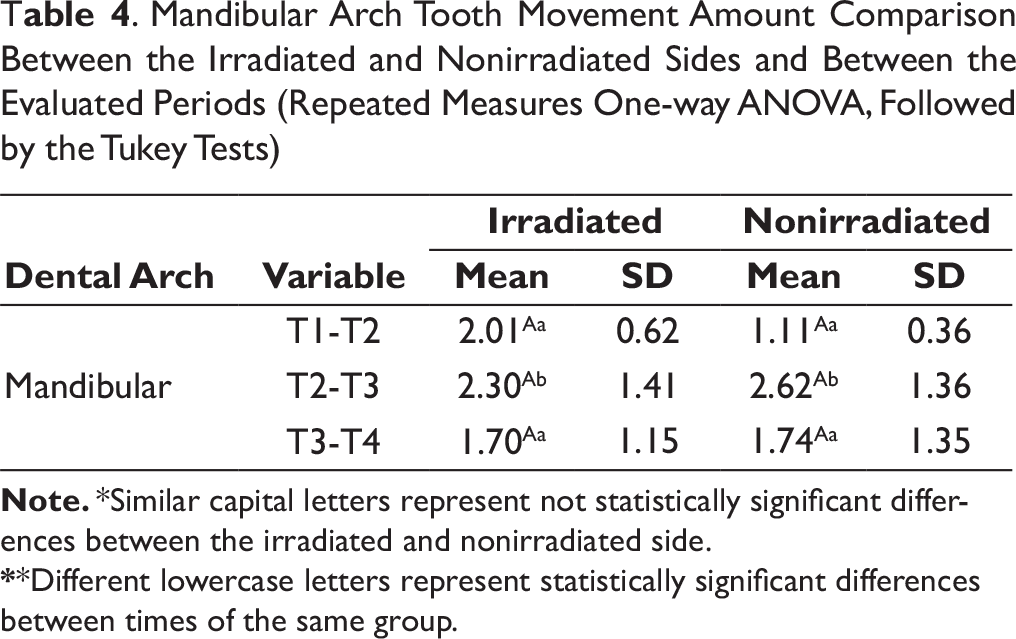
**Different lowercase letters represent statistically significant differences between times of the same group.
There was no difference in movement between the irradiated and nonirradiated sides (Tables 3 and 4). Tooth movement in the second evaluated period (T2-T3) was significantly greater than in the other periods.
There were no significant differences regarding the amount of root resorption or the alveolar bone crest height between the irradiated and nonirradiated sides (Tables 5 and 6).
Discussion
Effects of Low-level Laser Therapy on Dental Movement
. Com parison of the Amount of Root Resorption and Alveolar Bone Crest Height of the Maxillary Canines During the Experimental Period Between the Irradiated and Nonirradiated Sides (Wilcoxon Tests)

. Comparison of the Amount of Root Resorption and Alveolar Bone Crest Height of the Mandibular Canines During the Experimental Period Between the Irradiated and Nonirradiated Sides (Wilcoxon Tests)

Using segmented 0.014-inch NiTi archwires for canine retraction may be criticized because it may allow some canine tipping movement. However, this should not interfere with the results because the irradiated and nonirradiated sides were subjected to the same type of movement. Besides, similar methodology has been previously used. 27 Additionally, measurement of canine movement rate during initial canine retraction with 0.014-inch NiTi archwires was performed to avoid the bone remodeling process and presence of inflammation mediators prior to laser application, which could interfere in the canine movement rate and mask the laser effect. 28
According to the results, the LLLT protocol used in this study was not efficient in accelerating tooth movement during retraction of the maxillary and mandibular canines, similar to Limpanichkul and Heravi studies (Tables 3 and 4).2, 29 Limpanichkul et al used a higher dosage and attributed the inefficiency in increasing the rate of orthodontic movement to the high LLLT dosimetry used. Other studies also concluded that greater energies induce a null effect.16, 30 Oppositely, Heravi used a smaller dose (total energy of 6 J with energy density of 21.4 J/cm 2 per point), similar to those used in studies that were efficient in accelerating tooth movement.12, 13, 21 However, there was no significant increase in tooth movement. A possible cause could be the age factor, because his patient’s age was significantly greater than in the other studies. Adult patients have a slower bone turnover.31, 32 This would not be a plausible justification for the present study since the monthly total energy used was low, and patient ages were similar to other studies that found an increment in the rate of tooth movement.12, 14, 21
The energy density in this study and the total energy in each application (TE = 4 J for the mandible and TE = 9 J for the maxilla) increased according to the monthly single irradiation protocol, in relation to other studies. Other studies used similar monthly doses divided into various applications and similar daily doses with an increased number of monthly applications, both obtaining acceleration of movement,12, 14, 33 different from the present study, where it seems that the lack of tooth movement acceleration may be related to the laser application frequency and not specifically to the dosimetry. 34
There was acceleration of orthodontic movement using output powers of 100 mW and 200 mW,20, 21 suggesting that the increment of power was not responsible for the lack of acceleration in this study, but the smaller amount of laser exposure, consequent to the single laser application per month, different from other studies that presented a greater frequency of laser application, of at least 3 times in a month after retraction activation.12-14, 20, 21
The reason for evaluating the time factor is that some studies have shown greater laser effects in the first applications, after activation of the device. Cruz et al 12 observed a decrease in laser effects after the 14th day of application.
Some studies did not demonstrate any laser influence in the maxilla and the mandible, separately, and only compared the irradiated to the nonirradiated side, which may impair comparison with this study. 21 The greater thickness of palatal gingiva in the maxilla, in comparison to the mandible and to the maxillary buccal gingiva, lead to the use of higher doses in this area. Nevertheless, the negative results may be consequent to the used protocol or may have been influenced by the frequency.
Effects of Low-level Laser Therapy on Tissue Integrity
The results showed no statistically significant difference between the sides regarding the level of integrity of root apex and bone crest after initial canine retraction mechanics, demonstrating that the laser application protocol maintained the integrity of these tissues (Tables 5 and 6). These findings corroborate all existing clinical trials evaluating the effects of LLLT in root and alveolar bone crest after orthodontic movement.12, 13, 17, 21 These results disagree with those of Cossetin et al, 35 who observed acceleration of tooth movement, followed by a significant increase in osteoclastic activity, which caused a failure in alveolar remodeling and a higher degree of root resorption.
The current results demonstrate that the dose used seems to behave as a neutral or slight modulator for cell biostimulation. The biomodulation effect is dose-dependent and even with the correct wavelength and the appropriate dose, phototherapy may still not be effective in all systems and/or situations. Biomodulation was produced by the same laser dose on different functions of osteoblasts, in vitro.36, 37
Clinical Considerations and Suggestions for Future Work
The protocol used in this study did not result in a positive laser acceleration of tooth movement. A suggestion for future works would be to investigate other protocols such as the use of the same dose, but with a frequency of 2 monthly applications.
Conclusions
Low-level laser therapy did not increase orthodontic movement during initial canine retraction, using a single dose per month.
Low intensity laser did not cause greater root and alveolar bone crest resorption than on the nonirradiated side.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance CODE 001.