
Abstract
Abstract
Objective: To evaluate the effect of rapid maxillary expansion (RME) on mandibular rotation.
Materials and Method: A systematic review of articles selected from 4 electronic databases—PUBMED, Cochrane Central Register of Controlled Trials, Clinical Trials Registry, and Google Scholar—was carried out. Additional studies were hand-searched and retrieved from the reference lists of relevant articles. Studies published till August, 2019, were included in this study.
Results: A total of 28 articles were identified through electronic database searching. 16 articles were obtained after elimination of duplicates which were then screened. Full-text articles were assessed according to the eligibility criteria. 2 randomized controlled trials (RCTs) and 14 clinical trials (CTs) were identified for inclusion in the review. These studies effectively highlighted the effect of RME on mandibular rotation, primarily in the clockwise direction.
Conclusion: There is a moderate sum of evidence to illustrate the effect of RME on mandibular rotation. It can be concluded that RME brings about clockwise rotation of the mandible, ie in downward and backward directions, thereby increasing the lower anterior facial height. This effect could be attributed to the vertical maxillary movement and the extrusion of the maxillary molars.
Introduction
Rapid maxillary expansion (RME), also termed as rapid palatal expansion, is a substantial treatment modality for constricted maxillary arches that aims to expand the maxillary arch in order to harmonize the balance between the width of the jaws. Transverse discrepancies of the upper arch have been treated over a century with a medley of orthopedic and orthodontic forces. The strategy was first introduced by E.C. Angell in 1860. 1 Despite the initial disapproval that the technique faced, it remains the mainstay in clinical orthodontic practice today for the correction of maxillary trans-arch deficiencies.
Although RME aims to split the mid-sagittal suture to separate the maxillary shelves, its effects are not limited to the maxillary bone. The aftermath is also experienced by other surrounding structures such as the mandible, pharyngeal assembly, nasal cavity, temporo-mandibular joint, middle ear, and the pterygoid process of the sphenoid bone. 2 Hence, treatment-induced widening of the maxilla directly or indirectly exerts an influence onto the contiguous anatomic structures.
Baccetti et al and Macdonald et al have reported statistically significant counterclockwise rotation of the palatal plane.3, 4 This means that there is a greater degree of maxillary descent at it’s posterior end than the anterior end, which accentuates the downward and backward rotation of the mandible. This movement of the mandible is advantageous in Class III malocclusions with brachycephalic facial patterns, wherein the rotation blends harmoniously with the desired outcome. However, this effect is undesirable in vertically growing individuals pertaining a Class II jaw base relationship, with or without anterior open bite.
Giorgio Iodice et al aimed to quantify the sagittal and vertical changes in the jaws as a result of surgically-assisted RME (SARME) and have failed to find any statistical variation, both in the maxilla and the mandible. 5 On the contrary, some authors believe that the mandibular rotation seems to be a transient movement as the values observed 6 months post SARME tended to return close to the original values. 6
Because evidence-based medicine is crucial, it is imperative to report a well-designed systematic review that appraises all the scientific data and summarizes the current evidence. This systematic review covers all techniques employed to bring about RME, ie tooth-borne, tissue-borne, tooth and tissue-borne, and SARME. The reason for this strategy is to evaluate the influence of all kinds of expansion on mandibular rotation, irrespective of the technique.
The aim of this systematic review is, therefore, to evaluate the effects of RME on mandibular rotation.
Materials and Methods
Information Sources
Keywords
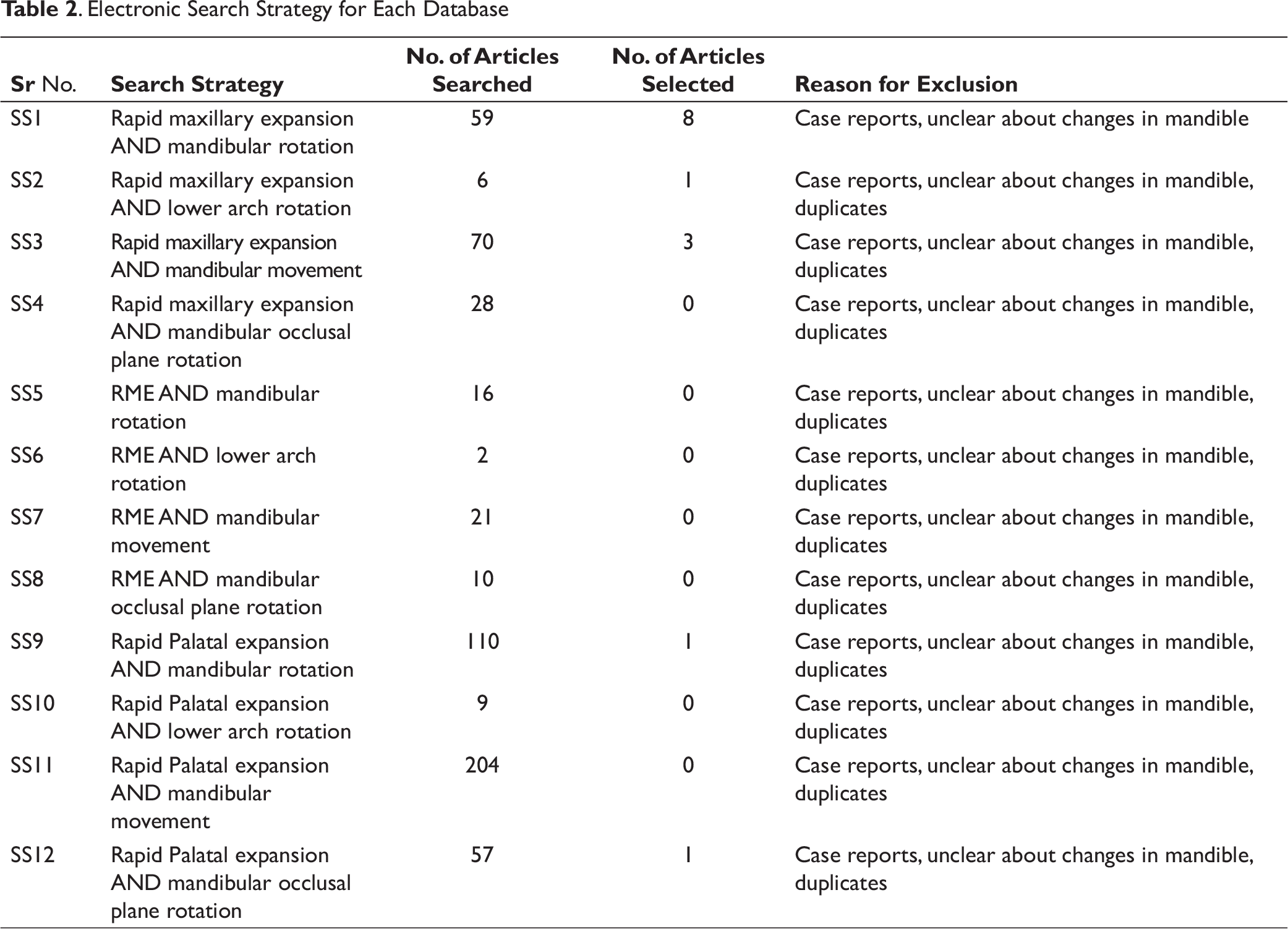
. Electronic Search Strategy for Each Database
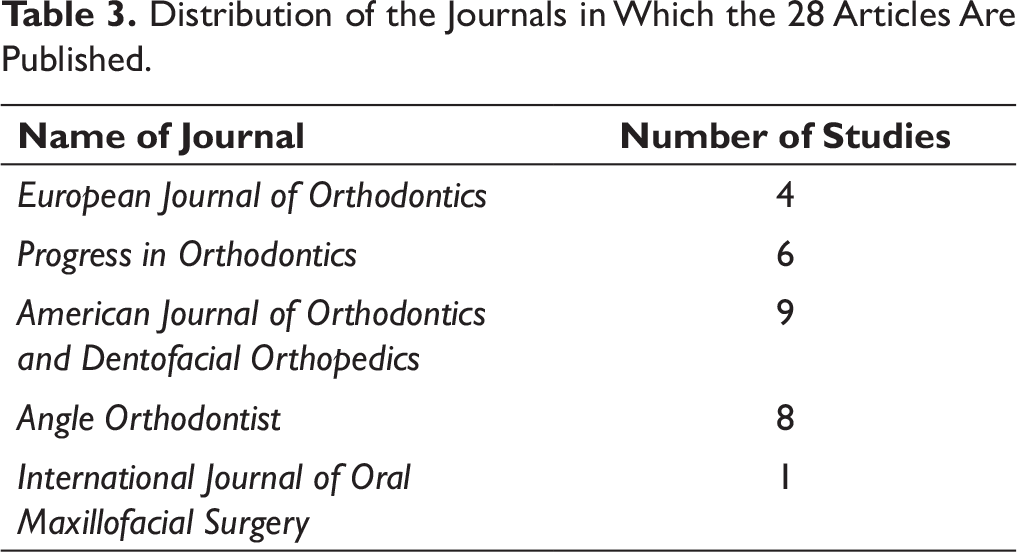
Distribution of the Journals in Which the 28 Articles Are Published.
Eligibility Criteria
Inclusion criteria:
Articles published till August, 2019. Articles providing information of the participants undergoing bonded, banded, or surgical RME. Study setting should be hospital based. All articles should be in English. Full text articles.
Exclusion criteria:
Articles that are narrative reviews, case reports, abstracts, letters to editorials, editorials, and animal studies. Articles that are unclear about the effect of RME on the mandible.
PICO
P—Participants: Orthodontic patients requiring RME.
I—Intervention: Banded/bonded/surgical RME.
O—Outcomes: Mandibular rotation.
Study Selection
Randomized controlled trials (RCTs) and clinical trials (CTs) were selected; however, only articles which provided clear data about the effects of RME on the mandibular rotation were included.
Items and Criteria for Quality Assessment with the Newcastle–Ottawa Scale
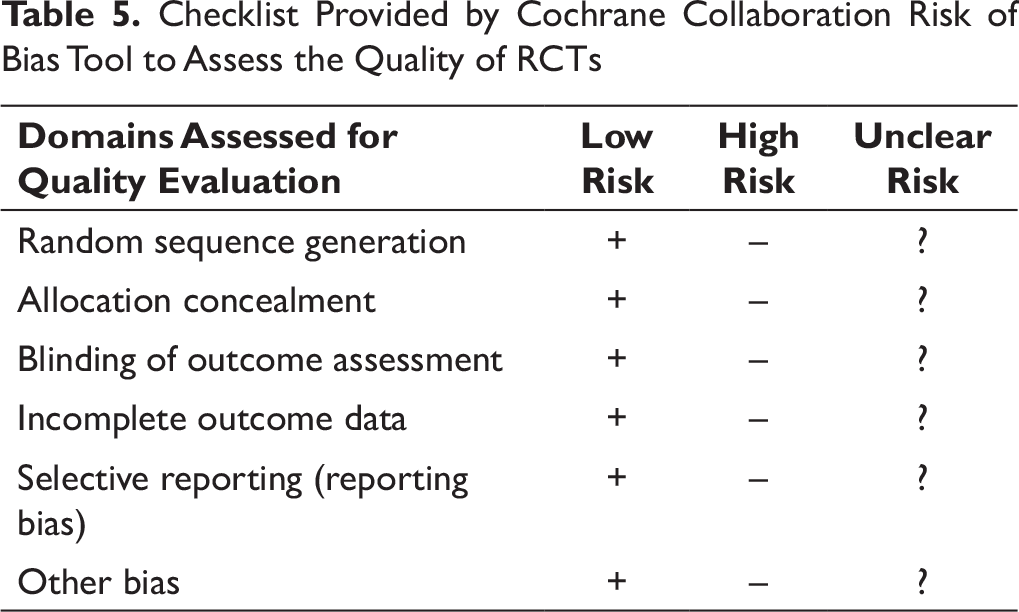
Checklist Provided by Cochrane Collaboration Risk of Bias Tool to Assess the Quality of RCTs
Quality Assessment
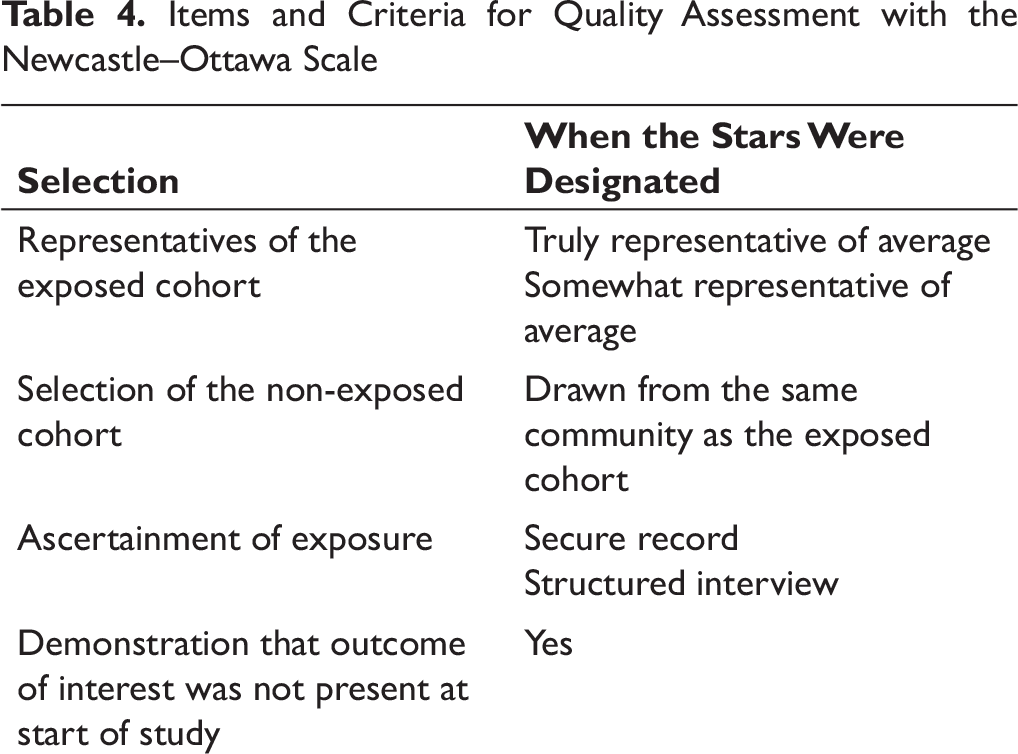
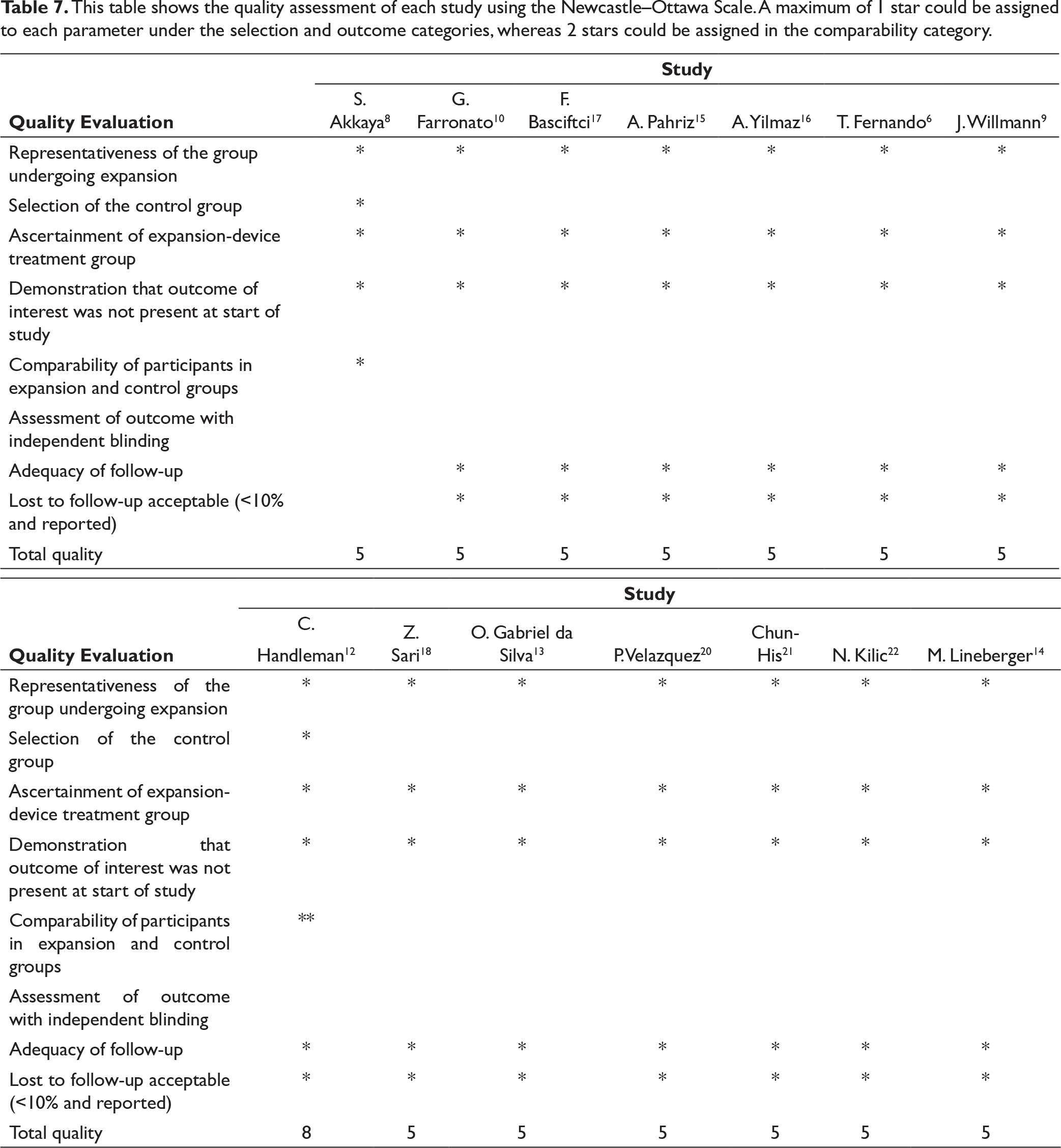
The Newcastle–Ottawa Scale was applied to assess the quality of the controlled CTs (CCTs).
21
The studies were appraised and were designated “stars” on the basis of 3 objectives:
Selection of study groups Comparability of groups Determination of outcome of study
The items and criteria of assessment are specified in Table 4.
The quality assessment of the RCT was done employing the checklist by Cochrane Collaboration risk of bias tool. 22 The checklist provided by Cochrane Collaboration risk of bias tool to assess the quality of RCTs is specified in Table 5.
Results
Study Selection
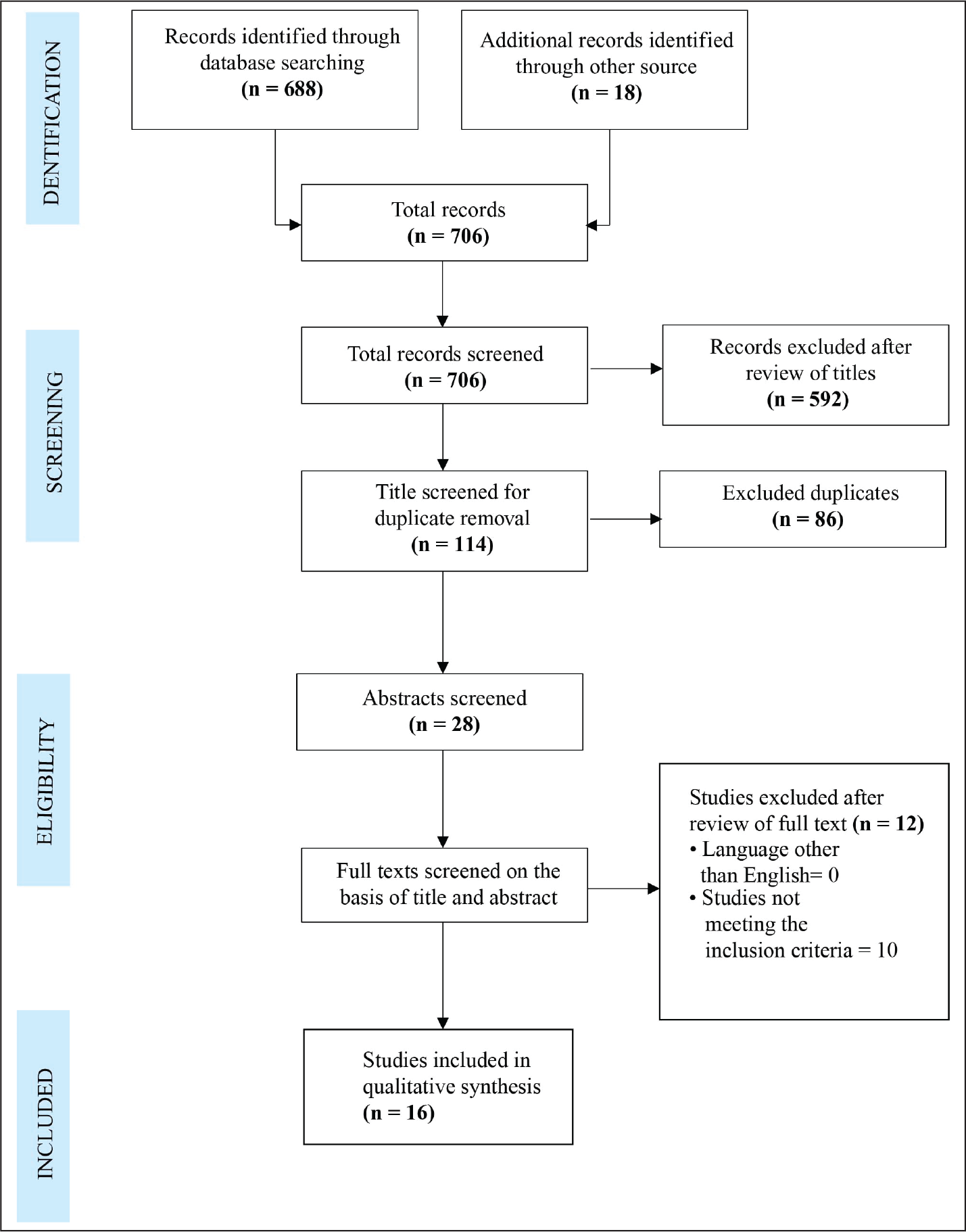
The data search was carried out based on the title relevant to the systematic review. A total of 706 titles were screened across various medical and dental journals, out of which 688 and 18 articles were obtained via online and manual hand-search, respectively. 114 titles were shortlisted. On duplicate removal and thorough reviewing of abstracts, 28 full-text articles were obtained to determine their compliance with the eligibility criteria. A final total of 16 articles satisfied the selection criteria and were selected for qualitative synthesis of the systematic review. This comprised 57.1% of the total articles obtained pertaining to the data search.
The present study was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA), the outline of which is illustrated in Figure 1.
PRISMA Flowchart Showing Study Selection Process
Study Characteristics
This table shows the quality assessment of each study using the Newcastle–Ottawa Scale. A maximum of 1 star could be assigned to each parameter under the selection and outcome categories, whereas 2 stars could be assigned in the comparability category.
This table shows the quality assessment of the RCTs using the Cochrane Collaboration risk of bias tool. A “+” sign indicates low risk of bias, whereas a “–” indicates high risk of bias. A “?” sign was assigned if the data provided was unclear.
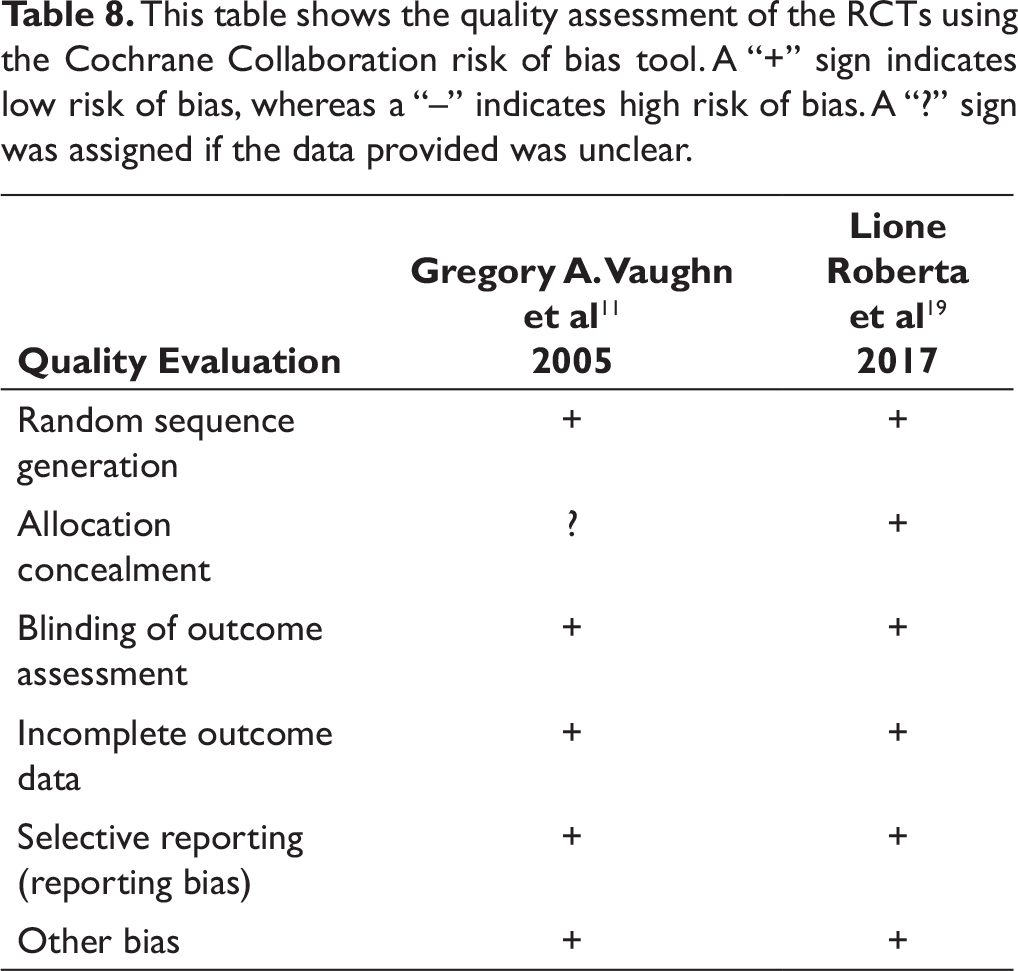
Methodological assessment of the quality of the included CTs were assessed using the Newcastle–Ottawa Scale. 23 The scores ranged between 5 and 8, indicating that the quality of the studies were moderate to high. The detailed quality assessment of all studies is tabulated in Table 7. The analysis of the checklist by Cochrane Collaboration risk of bias tool is shown in Table 8, indicating that the RCTs pertained a low risk of bias. 24
Discussion
The objective of RME is to controllably breach the mid-palatal suture, causing widening of the maxilla. The procedure has evolved over the years, especially after Hass put forth his concepts of expansion and illustrated the effects of his designed expander in 1961. 7 The multiple effects of RME on the maxilla and its contiguous structures have been studied since its inception. However, a detailed evaluation of its effect on the mandible is not well-recognized. The aim of this review is to collect, appraise, and compile all the available data related to the effect of RME on mandibular rotation. Although the results of the 14 studies included in this review could not be compounded statistically due to their heterogeneous nature, the outcomes of all studies remain invariable.
Sevil Akkaya et al aimed to compare the sagittal and vertical effects of rapid and slow maxillary expansion techniques. 8 The study employed the use of bonded Hyrax appliance in the former group, whereas a mini-expander in the latter one. At the end of active treatment, i.e. the desired expansion being obtained which was 0.7 to 1.6 months in the RME group and 1 to 5.6 months in the SME group, the appliance was worn for an additional 3 months for the purpose of retention. The study reflected an increase of 1.9° in the mandibular plane angle which was found to be statistically significant in the RME group. The mandible showed downward and backward rotation which the authors attributed to the accompanied maxillary rotation and molar extrusion. These findings coincide with those of Willman et al who investigated the skeletal outcomes of the Hybrid-Hyrax appliance in conjugation with facemask in Group 1 and with mentoplate appliance in Group 2 on the maxilla and mandible. 9 RME was carried out by activating the Hybrid-Hyrax appliance by 90°, 4 times daily until the desired expansion was achieved. The study revealed postero-inferior relocation of Point B in the facemask group, suggestive of a clockwise rotation in the mandible.
Giampietro Farronato et al evaluated and compared the skeletal changes of the Hyrax expander in the sagittal and vertical dimension in all types of malocclusions, ie, Class I, Class II, and Class III types. 10 On activation of the Hyrax appliance for 15 days with an additional retention period of 6 months, statistically significant mandibular changes were noted in the Class III group. In this group, there was an increase in the total anterior facial height and a decrease in the SNB, suggesting the downward and backward rotation of the mandible. No significant differences were found in the GoGn-SN readings in the Class I and Class II groups. In skeletal Class III patients, the ANB increased by 2.16° which was a resultant of the anterior positioning of the maxilla and the downward and backward rotation of mandible.
Gregory Vaughn et al in their RCT included 46 subjects with Class III malocclusion and subjected them to RME with or without facemask therapy. 11 A statistical increase was seen in the SN-MP, Pal-MP angles, and the lower anterior facial height in the former group, whereas no change in the latter was seen. This suggests that molar tipping and extrusion have shown to be the cause of bite-opening and increase in vertical dimensions after conventional RME treatment. As a result of the downward and forward movement of the maxilla with the use of RME, buccal tipping of the maxillary molars and extrusion of the palatal cusps lead to downward and backward rotation of the mandible. Vertical chin-cap application minimizes this effect.
Several authors used the Hass-type of palatal expander to achieve RME in orthodontic patients and evaluated its dentoskeletal effect in the vertical and sagittal dimensions.12-16 One study conducted by Chester S. Handelman, on the contrary, obtained disparate results. 12 In this study, RME and standard edgewise treatment insignificantly influenced mandibular rotation. The mandibular plane angle remained unchanged and no significant mandibular rotation was noted.
Omar Gabriel da Silva et. al. reported that rapid maxillary expansion brought about by Hass type palatal expander provokes a clockwise rotation of the mandible. A distinguishable increase in the GoGn-SN, GoGn-Pal angles and lower anterior facial height is suggestive of this mandibular movement. 13 There was an increase in the Go-Gn angle from 35.70° to 37.61°, GoGn-Pal from 27.64° to 28.98°, and Ans-Me from 62.97 mm to 63.94 mm. They concluded that there was an increase in vertical dimensions of the face because of the maxillary and mandibular downward and backward rotation. The increase in the LAFH (lower anterior facial height) is mainly due to this clockwise rotation of the mandible. Hence, the mandible displays significant postural alterations in response to RME and is the result of the maxillary molar extrusion caused by the buccoversion.
Matthew W. Lineberger et al conducted a study which evaluated the effects of RME on hyperdivergent patients. 14 This study subdivided the subjects on the basis of opening or closing in the mandibular plane angle during treatment. The opening group was comprised of 23 patients who displayed a clockwise rotation of mandible, whereas the closing group were 26 in number who depicts an anti-inclination of the mandibular base. The results of this study indicate that RME can be carried out successfully in patients with increased vertical dimensions without detrimental effects on the vertical skeletal relationships. With regard to the mandibular plane angle, the long-term changes in response to RME appear favorable because they express a tendency toward reduction in the angle.
A. Pahriz et al emphasized on the effect of SARPE on mandibular rotation and showcased changes brought about in the SN-MP and the Pal-MP angles. 15 The pre-treatment SN-MP angle, ie, 40.05° ± 7.67° increased to 41.16° ± 8.19°, whereas the Pal-MP angle showed a minor increase from 34.66° ± 8.47° to 34.88° ±7.78°. The authors suggest that the mandible shows some amount of downward and backward rotation of the mandible leading to a bite-opening effect. The findings of this study remain consistent with those in a study conducted by Talles Fernando Medeiros Oliveria which validates a clockwise rotation of the mandible immediately after SARME. 6 This is well-represented by an increase in the values of FMA as well as the downward and backward displacement of Menton. However, the mandibular rotation seems to be a transient movement as the values observed 6 months post SARME tended to return close to the original values.
Alev Yilmaz et al compared the short-term effects of mini-implant-supported maxillary expansion appliance with two conventional expansion protocols, ie, bonded and banded RME. 16 There were insignificant changes observed in mandibular rotation in subjects undergoing MARPE, although the conventional approaches displayed upper molar tipping and extrusion resulting in bite-opening and increase in vertical dimensions. As a result of the downward and forward movement of the maxilla, buccal tipping of the maxillary molars and extrusion of the palatal cusps led to downward and backward rotation of the mandible. It was noted that vertical chin-cap application minimized this effect. This study concluded that RME has a serious bite-opening effect due to the downward and backward rotation of the mandible. In this study, skeletal vertical measurements indicate this posterior rotation of the mandible. However, this change was not seen in the MARPE group and was only shown by the other two groups.
Two groups of authors used modified acrylic-bonded RME devices.17, 18 F.A. Basciftci et al in their study reported that, the mixed dentition subjects displayed an increase in the mean SN-MP angle from 37.75° to 39.64° and showed a tendency to decrease to 38.6° after a retention period of 25 weeks. 17 The lower anterior facial height showed a millimetric increase of 2 mm and a decrease by 1 mm after retention. In the permanent dentition group, the mean SN-MP angle increased from 39.9° to 40.9° and showed a tendency to decrease to 39.6° after the same retention period. The lower anterior facial height in this group showed a millimetric increase of 3 mm and a significant decrease by 6 mm after retention. This reflects that RME incited an increase in the vertical dimensions of the face because of the maxillary and mandibular downward and backward rotations. This is possibly due to the greater buccal tipping of the anchoring molars in this group. The values, however, suggest that the mandibular rotation seems to be a transient movement as the values observed 25 weeks post RME tended to return close to the original values.
In the latter study conducted by Zafer Sari, there were statistically significant changes seen in the SN-GoMe, SNB angles, ANS-Me linear, all pertaining to the aforesaid mandibular rotation. 18 There was an apparent increase in the mean SN-GoMe from 39.93° to 41.08° and the SNB angle from 73.63° to 74.16°. The anterior facial height, however, remained constant. The study highlighted that the downward and backward rotation of the mandible and the vertical increase in the facial skeleton resulted in a small but statistically significant increase in the overjet and decrease in the overbite.
Roberta Lione et al conducted a randomised controlled trial to evaluate mandibular response to banded and bonded RME. 19 The study included 30 growing patients exhibiting skeletal Class II malocclusion having a mean age of 8.1 ± 0.6 years. The samples were blindly assigned using a computer-generated randomization list and allocated into 3 groups: banded, bonded, and a control group. The study revealed no statistical differences in the sagittal position of the maxilla and the mandible. However, vertical changes included a statistically significant increase in the gonial angle in the banded RME group as compared to the other groups. These findings remain consistent with the work of other authors who demonstrated a decrease in overbite due to a downward and backward rotation of the mandible, incited by RME. 20, 21, 22
A meta-analysis could not be carried out due to the heterogeneity encountered among the studies included in this literature review. The data provided by all studies was evaluated qualitatively to affirm the influence of RME on mandibular rotation. However, a quantitative evaluation could not be implemented because the measurements inspected to ascertain mandibular rotation varied among all studies. Some studies suggested a clockwise mandibular rotation on the basis of an increase in GoGn angle, whereas others on the basis of an increase in FMA angle, SN-MP angle, inter-basal angle, lower anterior facial height, postero-inferior relocation of point B. Thus, quantitative agglomeration of the data could not be achieved, ie, the data could not be mathematically combined.
All studies displayed heterogeneity with regard to the treatment modality used, the duration of treatment, retention protocol, and follow-up. The duration of treatment varied between 7 and 14 days in studies using bonded or banded forms of RME, although some continued expansion until the desired posterior intercuspation was achieved. 7 out of 14 studies extended their observation of the effect of RME on mandibular rotation after a retention phase. Three studies evaluated post-retention records to portray the long-term effects of RME on mandibular rotation.14, 16, 18 On the other hand, other studies contemplated the clockwise mandibular rotation as an additional finding and evaluated it only in the short term.
A limitation noted during the course of compiling this systematic review was the limited number of studies fulfilling our selection criteria, indicating that the vast majority of published studies have inherent design flaws in the conduct and reporting of their scientific investigations upon which results are based. Although several case reports and CTs have been carried out, there was a limited number of RCTs to substantiate the accuracy of this effect. All CCTs had high risk of bias. Lack of sample size calculation and fewer samples were some of the flaws of the studies. Further studies must be conducted to determine which type of RME, whether bonded, banded, or surgical produces a more pronounced mandibular rotation. This enunciates the importance of developing well-researched RCTs to derive definite conclusions.
Conclusion
RME brings about a downward and backward rotation of the mandible, thereby increasing the mandibular plane angle and the lower anterior facial height. This phenomenon is most likely due to the extrusion of the maxillary molars accompanied by their buccoversion, which accounts for the mandible’s clockwise rotation. However, the variation in the degree of mandibular rotation in different types of RME is not evident.
This rotation does not however, have detrimental effects because the phenomenon is transient in nature.The mandibular plane rotates to its original position in the long term, taking into account that molar extrusion can be controlled by appropriate measures. Therefore, RME is not a contra- indication and can be successfully carried out in skeletally vertical patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.