
Abstract
Abstract
Objective: To compare the effectiveness of blended learning versus traditional learning in a cephalometric learning module for undergraduates.
Materials and methods: This study was designed as a pre- and posttest trial. 150 undergraduates were randomly allocated to two groups: group 1 for traditional learning, and group 2, for blended learning. Pretest and posttest scores of both groups of 25 MCQs on cephalometrics were obtained. Feedback was obtained from the participants in this study and analyzed.
Results: In group 1, the mean pretest and posttest scores were 13.87 and 16.10, respectively. In group 2, the mean value for the pretest and posttest scores were 14.01 and 22.18, respectively. The mean improvement in knowledge score was significantly higher in group 1 (2.233) compared to the mean score of group 2 (8.171). The level of statistical significance was P < .001. Feedback analysis showed the participants found the experience with Dolphin software better than traditional learning (Dolphin Cephalometric Imaging and Management software [version 11.8.24 Chatsworth,CA,USA]). For over 50% participants, their overall opinion on the cephalometric module was very good (score = 5).
Conclusion: Blended learning increases the effectiveness of cephalometric learning by means of better student performance. Commercially available Cephalometric software can be used for e-learning instead of a specifically designed learning software.
Introduction
Orthodontic training for undergraduates involves understanding of the basics of growth and development, occlusion, diagnosis and treatment planning, branches of orthodontics, various appliances used, and retention. Cephalometric analysis has been a standard method of establishing orthodontic diagnosis, treatment planning, and prediction and monitoring of growth, and orthodontic treatment as such. 1 Because of its importance, cephalometrics forms a core part of undergraduate education in orthodontics. The traditional method of teaching cephalometrics for undergraduates has been by the use of seminars and demonstration of cephalometric tracing and analysis.
The traditional method of learning involves providing with specific learning milestones, logical reasons for the students and sharing individual preclinical or clinical experiences. The drawbacks of traditional learning include dependence on the knowledge, clinical, and communication skills of the teacher. Traditional learning also depends heavily on the imaginative perception of the students. 2
Numerous studies have been conducted on e-learning in the field of medical and dental training in which participants are asked about their attitudes toward a particular subject.3-7 With the advent of the use of computer-based learning in dentistry, it is only deemed necessary that software-assisted learning must be incorporated in the teaching method for generating interest for this tech-savvy generation of students. There are a few studies in the literature that have evaluated the effect of using software-based cephalometric learning.8, 9 Hence, this study was conducted to compare the effectiveness of blended learning versus traditional learning in a cephalometric learning module for undergraduates. The research questions framed were as follows: (1) Was there a statistically significant difference between the improvement in knowledge scores of students who received blended learning versus those who received traditional learning? and (2) What were the relative positive and negative feedback in the questionnaire given at the end of the cephalometric module?
Materials and Methods
The sample for this study involved undergraduates who were in compulsory rotatory residential internship (CRRI) or the fifth year of Bachelor of Dental Surgery curriculum. 150 CRRIs participated in this cephalometric module. During the fourth year in undergraduation, the participants had attended didactic lectures on the basics of cephalometrics, hard and soft tissue landmarks, and cephalometric analyses. The study was commenced in Dental College of Puducherry after the approval of the Institutional Ethical Committee. The study design was prospective, questionnaire based, and randomized 2-arm trial. Informed consent was obtained from the students and the details of the cephalometric module were explained prior to their participation in this study. The students were informed that their participation in the cephalometric module did not influence their course outcome or overall assessment during their CRRI period. Attempting both pre- and posttests, and filling the feedback questionnaire were prerequisites to participate in this study, and the same was mentioned in the informed consent.
Sample Size Estimation
A total of 150 CRRIs students were selected for this study and the sample size was arrived based on the previous literature.
8
Alpha (α) = 0.05, Beta (β) = 0.2
Organization of the Cephalometric Module
Mean, standard deviation in group 1(µ1) = 39.70 + 2.84, mean in group 2 (µ2) = 41.90 + 4.19, ration (group 1/group 2) = 1, minimum total sample required = 102.
The sample size was estimated to be 51 per group and adjusting for drop out the final sample size was 60 per group. Since all the CRRIs were interested in participating in this study, we achieved a sample of 75 students per group.
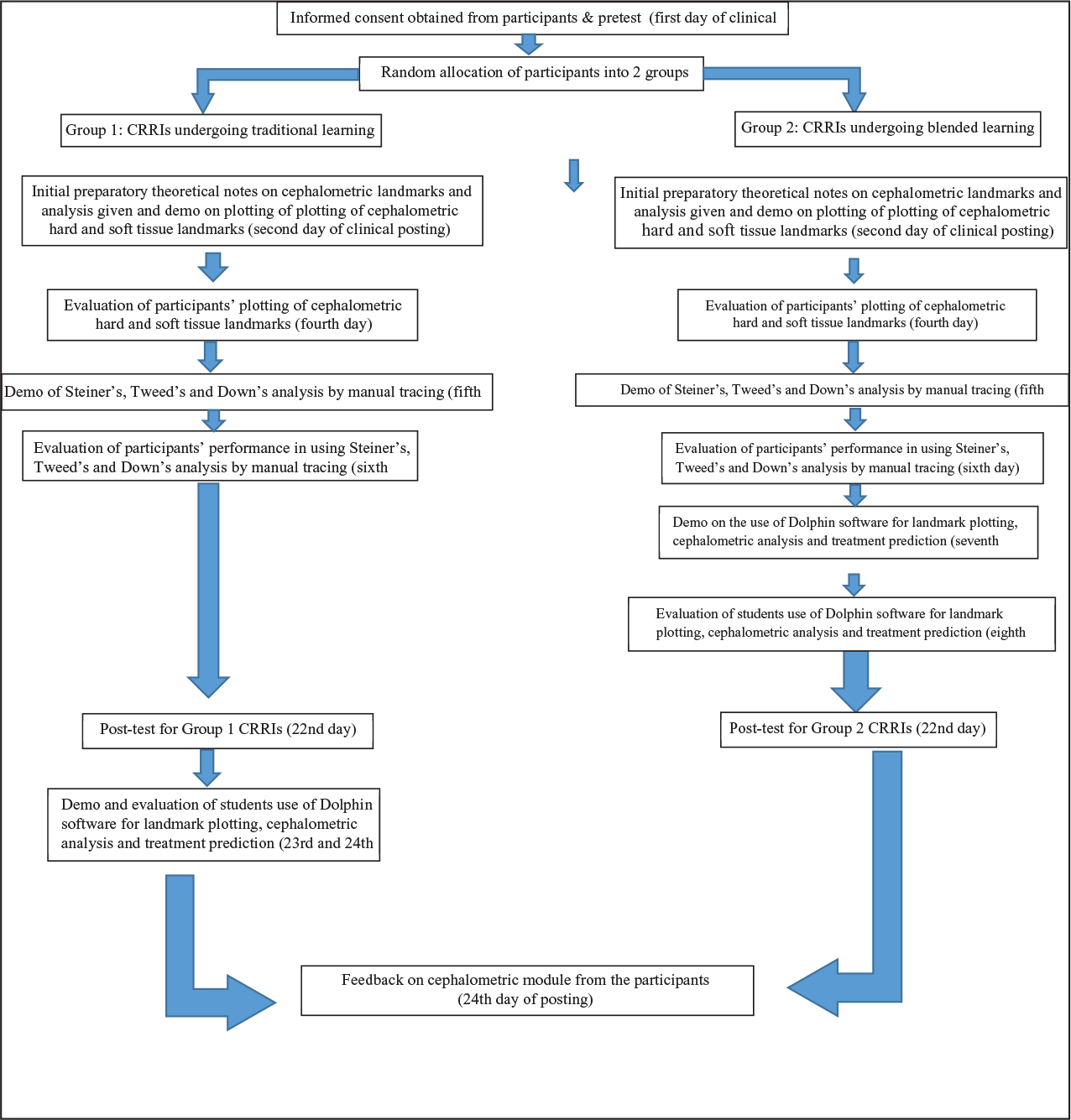
The participants (CRRI students) were randomly allocated one of the 2 groups on the first day of the clinical posting in the Department of Orthodontics. The allocation was double blinded and done using a concealed envelope. An independent assessor performed the allocation. 25 multiple-choice questions (MCQ) were used for designing the pretest and posttest questionnaire based on the cephalometrics from undergraduate orthodontic syllabus. The MCQ questionnaire was prevalidated by 4 orthodontists with a minimum of 4 years of teaching experience. The questionnaire was checked for content, and criterion-related and construct validity. The corrections suggested by the reviewers were incorporated into the questionnaire. Similarly, the same 4 reviewers validated the posttest feedback with ranked closed questionnaire, and open-ended questions and corrections were added.
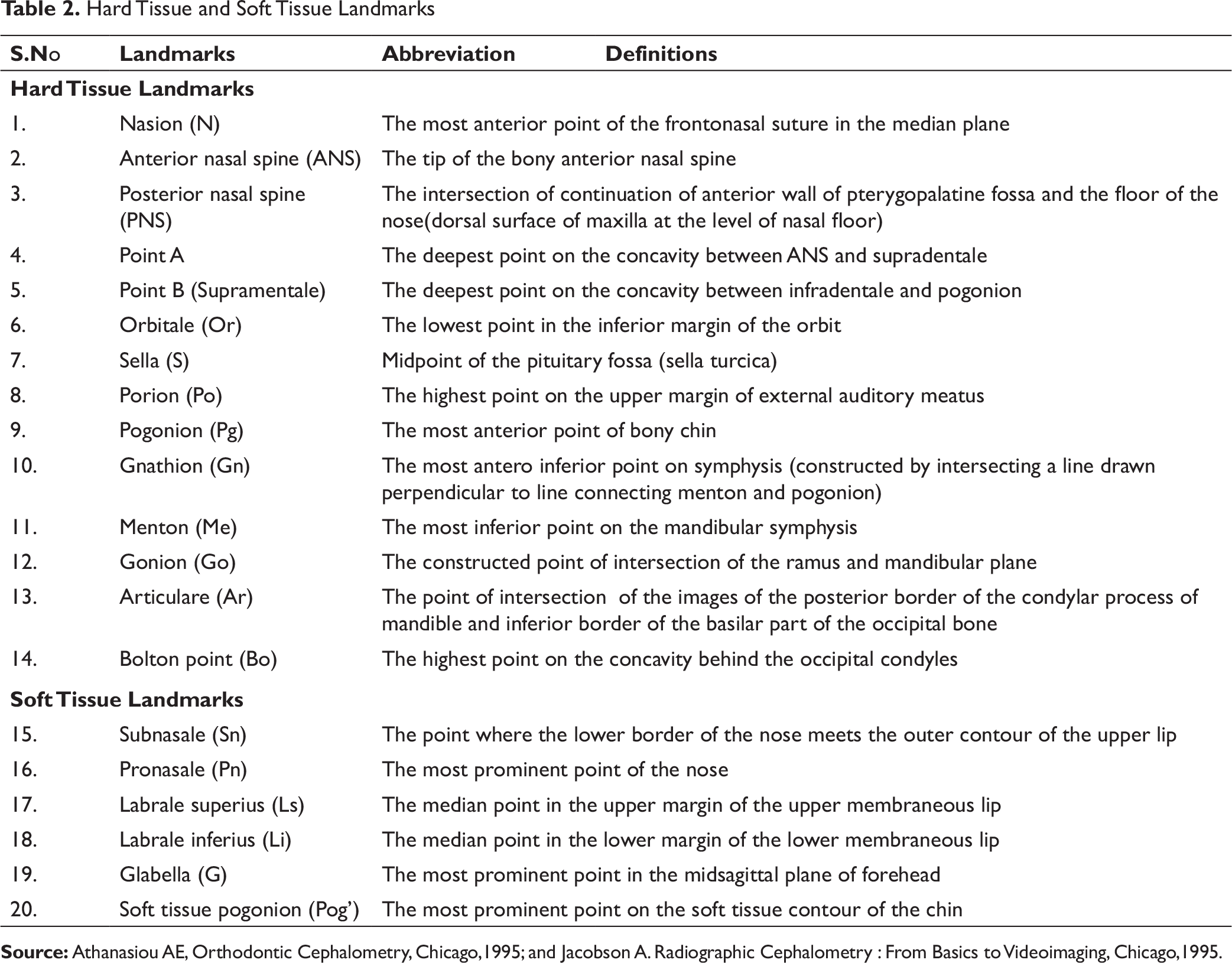
Hard Tissue and Soft Tissue Landmarks
Group 1 (Traditional Learning)
Initial preparatory material was provided to the participants which contained organization of the cephalometric course module, definition of hard and soft tissue landmarks and parameters with mean values, and inferences of Down’s, Steiner’s, and Tweed’s cephalometric analyses. After attending the pretest, demo was given for manual plotting of cephalometric landmarks and Steiner’s, Tweed’s, and Down’s analyses to the participants. The participants were then asked to plot the landmarks shown in Table 2 and perform the cephalometric analyses. The tracings were assessed and the errors in plotting of landmarks and performing the analyses were notified. The posttest was conducted on the 22nd day of the clinical posting following which demo was given on the use of the Dolphin software for tracing and analysis. Feedback on the entire cephalometric module was collected.
Group 2 (Blended Learning)
Initial preparatory material was provided on the 2nd day of posting, and students underwent similar training as group 1 students. The students had to show satisfactory performance in the manual tracing before undergoing software-aided cephalometric learning using the Dolphin software (Dolphin Cephalometric Imaging and Management software [version 11.8.24 Chatsworth,CA,USA]). Students with gross errors in cephalometric tracing and analyses were asked to repeat the manual tracing. The demo on the use of the Dolphin software for plotting and cephalometric analysis was given on the eighth day and the students’ performance on the use of the Dolphin software was evaluated on the next day. On the 22nd day of clinical posting, posttest was conducted and feedback was obtained from group 2 students.
The various features of the Dolphin software were explained to the students. While digitizing the landmarks in the Dolphin software, there were four machine-assisted learning features: (1) Definition of the landmark to be plotted, (2) position of the landmark in a sample cephalometric image and traced outline figure, (3) magnification of the area where the cursor is pointed for better accuracy in plotting the landmark, and (4) easier replotting of landmark in case of any discrepancy. Each student was asked to digitize the lateral cephalometric image using all of the machine-assisted learning features. The students then were taught to simulate the treatment plan and observe the cephalometric and soft tissue changes.
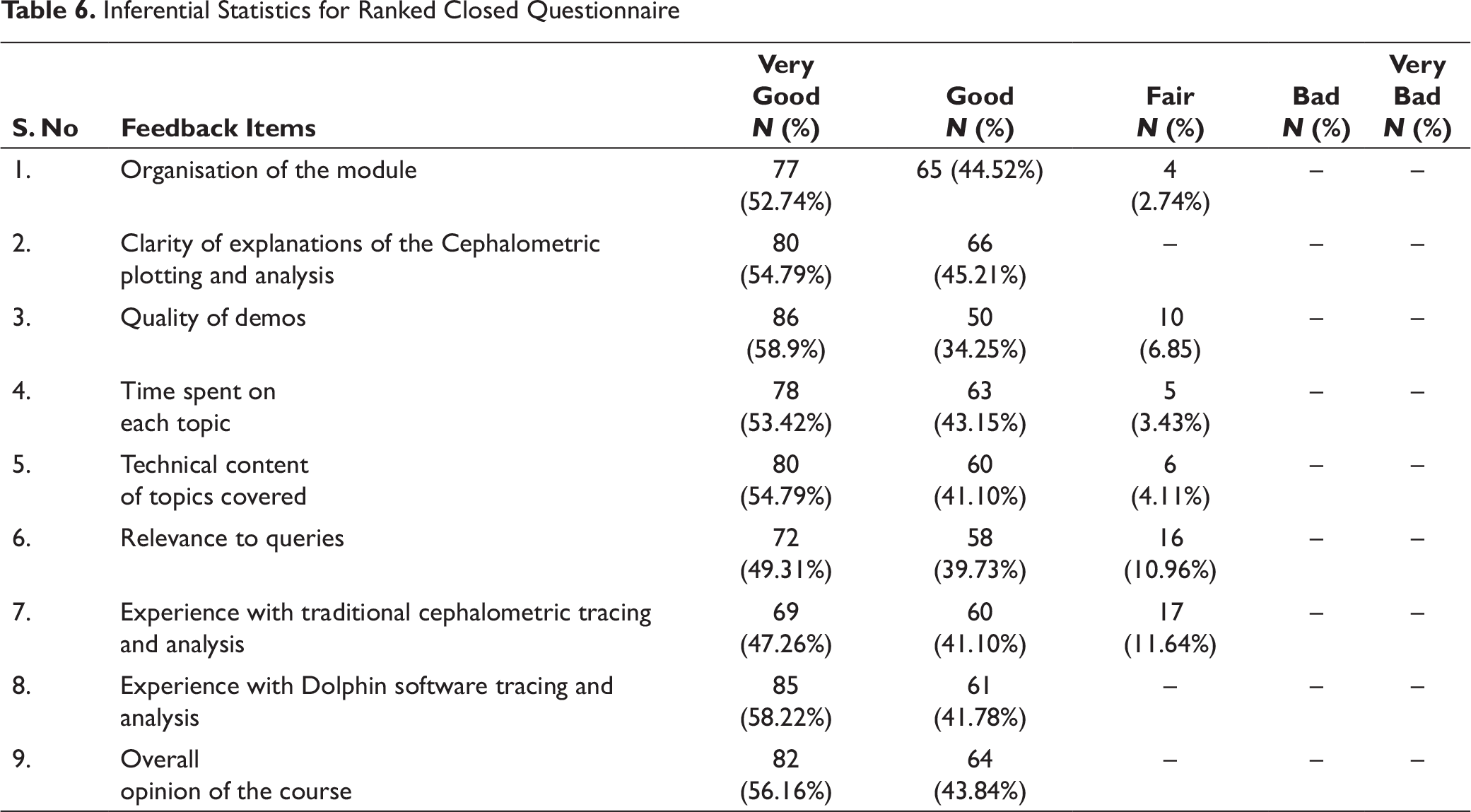
The feedback consisted of 9-item closed questionnaire and 6 open-ended questions on organization, quality of demos given, technical content and experiences with traditional, and software-aided cephalometric learning. The closed questionnaire was rating scale on a scale of very good (score = 5), good (score = 4), fair (score = 3), bad (score = 2), and very bad (score = 1).
The open feedback consisted of the following questions:
Did attending this module enhance your understanding of cephalometrics? If yes, how did it enhance your learning? Describe your experience with the Dolphin software learning. Which method of learning did you find easy to learn? Did you find any added advantage of using the Dolphin software? What were the hindering factors in learning in this module? What were the facilitating factors for learning in this module?
Comparison of Pre- and Post-test Scores of Group I and Group II Participants

Comparison of Pretest Score Between the Group I and Group II

Comparison of Improvement in Knowledge Score Between Group 1 (Traditional Learning) and Group 2 (Blended Learning)

Inferential Statistics for Ranked Closed Questionnaire
Results
Paired t test analysis was done to compare the pre (T0) and posttest (T1) scores of group 1 and group 2 students. The level of statistical significance was P < .001. In group 1, the mean value for the pretest score was 13.87 whereas the mean value for the posttest scores was 16.10. In group 2, the mean value for the pretest was 14.01, whereas the mean value for the posttest scores was 22.18 (Table 3). The mean posttest score of group 2 students was significantly higher than that of group 1 students.
The comparison between the pretest scores of group 1 and group 2 is shown in Table 4. There was no significant difference between the mean pretest scores of both groups.
Table 5 shows the comparison of improvement in knowledge scores between group 1 (traditional learning) and group 2 (blended learning). The mean improvement in knowledge score was significantly higher in Group 1 (2.233) compared to the mean score of Group 2 (8.171). The level of statistical significance was P < .001.
The feedback analysis was common for both the groups and hence tabulated in Table 6. The feedback analysis showed that more than 50% of the participants felt that the organization, technical content, quality of demos given, and the clarity of explanations given of the cephalometric module were very good (score = 5). The participants found the experience with Dolphin software better than traditional learning.
Discussion
In this study, the effect of e-learning resource on the outcome of cephalometric learning of undergraduate students was assessed. Although being a time and resource-consuming process, e-learning, as an adjunct to traditional lecture-based learning, aims at improving students’ theoretical and manual skills in various fields of education. 10
Development of a software exclusive for computer-assisted learning might be expensive and time consuming as shown by previous studies.11, 12 Moreover, the efficacy of the computer-assisted learning software would depend heavily on the expertise of the technical and subject material experts. Hence, in this study, a commercially available Cephalometric software was used for blended learning. Dolphin Cephalometric Imaging and Management software (version 11.8.24 Chatsworth, CA, USA) was used for software-aided cephalometric teaching. Dolphin software is one of the popular software used by dentists and orthodontists for cephalometric diagnosis and treatment planning. Dentists can contour a patient’s profile, use drawing tools, plot cephalometric landmarks, and overlay images from other cases to produce a finished image that illustrates various treatment options.13, 14
In this study, only students who had attended didactic lectures on cephalometrics (as a part of fourth year undergraduate syllabus) were included. The contents of the cephalometric module were structured according to the syllabus for cephalometrics as provided for orthodontics by the Dental Council of India. Findings of previous research on e-learning on student performance have shown that e-learning produces similar impact on student performance as traditional learning.15, 16 In previous studies by Luffingham JK, 17 Irvine NR et al, 18 Komolpis R et al, 19 Lowe CI et al, 20 and Turner PJ et al 21 it was observed that e-learning amounted to small but statistically significant improvement of knowledge. The present generation of students is more tech-savvy and wishes to relate learning with technology. Time spent on learning and perception toward e-learning play an important role in student performance.
Time spent on learning is dependent upon the students’ prior knowledge of the subject and degree of motivation, learning style, and the students’ perceived difficulty of the learning material or e-learning aid.22, 23 With regard to perception toward e-learning, it should be noted that e-learning offers better perception by means of more possibility of interactive learning.24, 25
The results of this study showed that e-learning when incorporated with traditional learning as part of a module improved the knowledge retention of the students. This was evident from higher mean posttest value of students in blended learning group (22.18) as compared to traditional learning group (16.10). There was also statistically significant increase in improvement in knowledge scores of students who underwent blended learning (2.233) than students who underwent only traditional cephalometric learning (8.171) (P < .001 level of statistical significance). This correlated with the findings of previous studies where student groups, for whom e-learning was used in blended learning, showed better performance and knowledge in cephalometry.8, 26 Group 1 (traditional learning students) were given demo on the use of the Dolphin software tracing and analysis and also were evaluated for the same at the end of the clinical posting.
The feedback from the students obtained for the cephalometric was generally positive and the students showed increased interest while using the Dolphin software. When asked to choose as to which method of training was easier, 60% of the students preferred Dolphin software. 10% of the participants wanted to use both the methods of training for better learning. For 60% of the participants, the e-learning module provided for better understanding on cephalometrics. 80% of the participants, when asked about the advantage of software-assisted learning, mentioned that Dolphin-software-assisted learning “had features of magnifying the area where landmark is to be plotted”, “was more accurate”, and “had less chances of errors while plotting landmarks”.
The limitations of this study were that only a small sample of students were chosen for participating in this cephalometric module and only knowledge retention with respect to cephalometrics alone was considered. A further study would be required to compare the cephalometric tracing skills of the students who received traditional learning with students who receive blended learning. The modalities in blended learning have now also extended with the use of smartphones. Recent studies in health profession education have shown that smartphone applications used for e-learning have been positively received by students.27, 28, 29
Conclusion
From the results and feedback obtained in this study, the following can be concluded:
Computer software (commercially available such as Dolphin) assisted learning should be incorporated as a part of regular cephalometric teaching. E-learning provides with self-directed learning and generates interest on the topic thereby accounting for better student performance in cephalometrics. Commercially available cephalometric software can be put to use for blended learning instead of developing special cephalometric learning software and presentations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.