
Abstract
Abstract
This article reports the successful camouflage of skeletal Class III malocclusion in a 20-year-old man through distalization of the mandibular dentition using miniscrew anchorage from the external oblique ridges of the mandible. In addition, maxillary face mask wear assisted in the closure of maxillary spacing without retroclination of maxillary incisors. This combination may be effective in the management of adult Class III skeletal malocclusions that are amenable to camouflage therapy.
Introduction
Skeletal Class III malocclusions in adults can be treated with orthodontic camouflage or orthognathic surgery depending on the severity of the case.1-2 Successful distalization of the mandibular dentition for Class III camouflage has been reported using inter-arch Class III elastics, 3 multi-loop edgewise archwire, 4 and lately, miniscrew anchorage from interdental sites 5 and retromolar region. 6
Jing et al 7 used the external oblique ridge of the mandible for miniscrew anchorage to distalize the mandibular dentition.
Following the work of Petit 8 and McNamara, 9 face mask therapy alone or in conjunction with rapid maxillary expansion has become a valuable tool for growth modification in children with Class III malocclusion due to maxillary deficiency.
As face mask therapy works through a combination of skeletal growth and dento-alveolar compensation, 10 it should theoretically be possible to obtain at least the latter effect in adults.
No previous reports have documented the combined use of face mask wear and mandibular miniscrew anchorage from the external oblique ridge for management of adult Class III malocclusion.
The case presented here illustrates the camouflage of skeletal Class III malocclusion in a man using miniscrew anchorage from the external oblique ridge for distalization of the mandibular dentition in conjunction with face mask wear.
Case Report
Diagnosis and Treatment Planning
A 20-year-old man reported to the clinic with the complaint of unsatisfactory facial appearance.
Frontal examination showed normal vertical proportions, inadequate incisor display, and maxillary midline diastema on smiling. The face appeared slightly asymmetric due to nasal deviation to the left. Soft tissue profile was concave with a deficient midface and protrusion of the lower lip. Chin projection appeared normal (Figure 1).
Pretreatment Extra-Oral Views

Pretreatment Intra-Oral Views

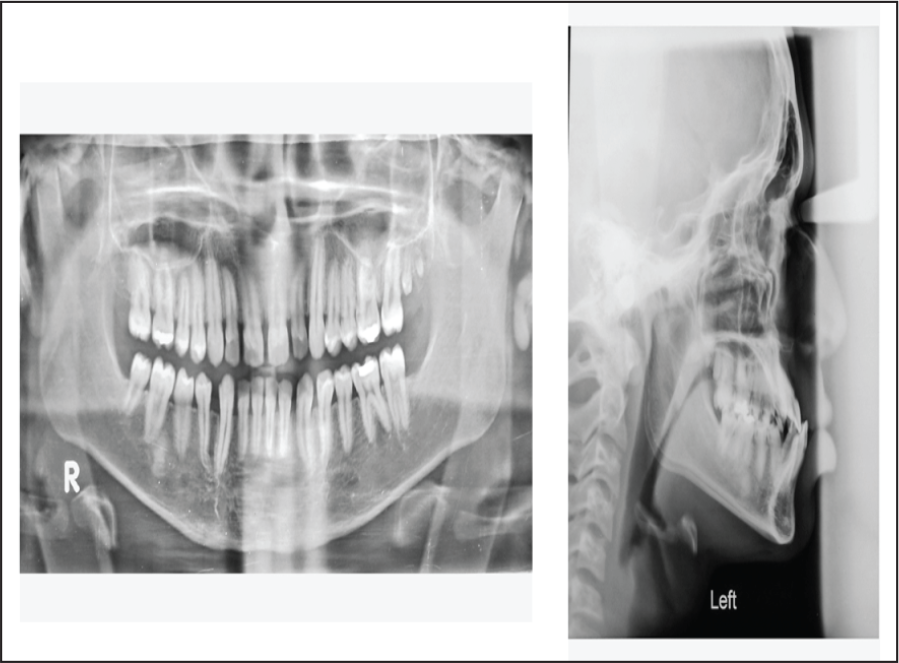
Pretreatment Radiographs
The incisors were in a crossbite relationship with reverse overjet of −2 mm and 50% overbite. Molar and canine relationships were super Class I on the right side and Class III on the left side, respectively. Spacing of 4 mm and 7 mm were present in the upper and lower arches, respectively. The mandibular midline was deviated 1 mm to the right of the facial midline; 3 mm curve of Spee was present in the lower arch. Amalgam restorations were present in 16, 26, 27, and 36 (Figure 2).
Mandibular movements were within normal limits, and there was no evidence of CR-CO discrepancy, pain, or TMJ pathology. There was no history of mandibular prognathism in his family.
Orthopantomogram showed the absence of maxillary right and mandibular third molars. Two diminutive, unerupted teeth were present in maxillary left third molar region (Figure 3).
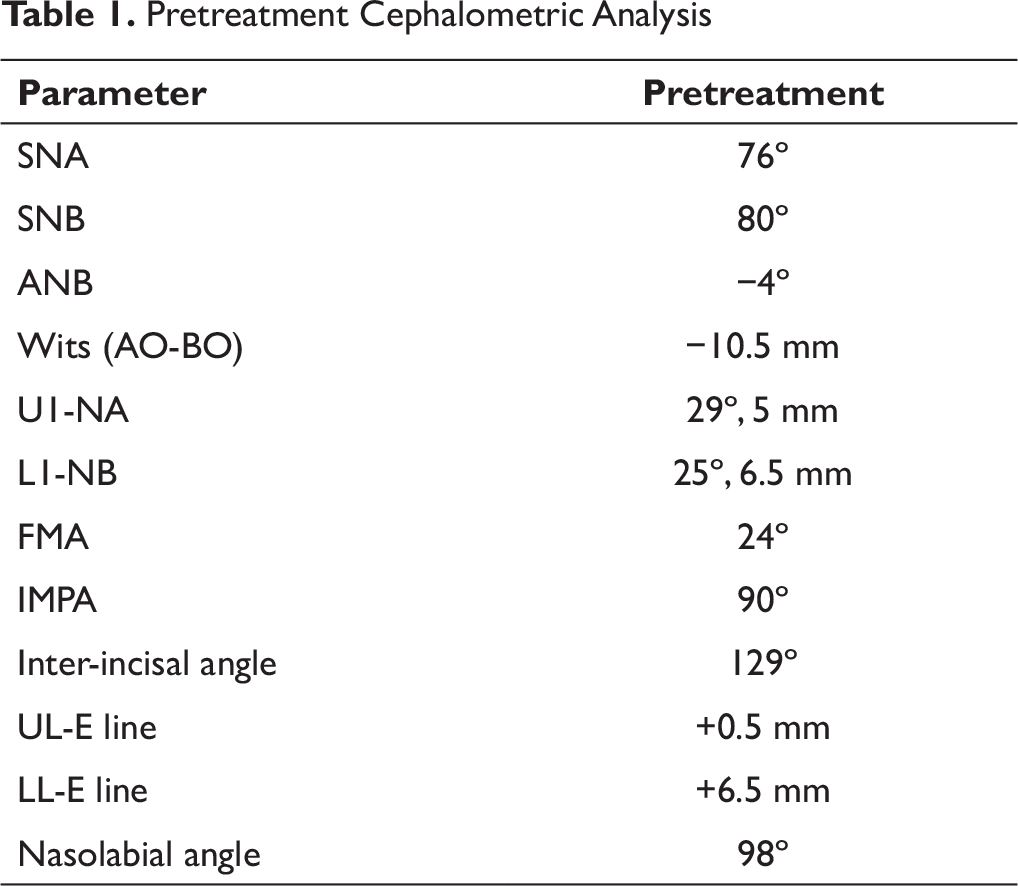
Cephalometric analysis indicated a Class III skeletal pattern (Table 1). The maxilla was retrusive (SNA = 76º) relative to the cranial base, whereas the mandible was normally positioned (SNB = 80º).
The upper incisors were mildly proclined, but the mandibular incisors were normal (IMPA = 90º). The skeletal pattern was normal (FMA = 24º). The lower lip was significantly protruded relative to the upper lip and chin (LL-E line = +6.5 mm), while the nasolabial angle was in the normal range (98º).
As the patient was an adult, the treatment options were restricted to camouflage orthodontic treatment or orthognathic surgery.
Factors in favor of attempting orthodontic camouflage were:
Favorable chin projection with absence of true mandibular prognathism. Normal vertical skeletal relationship. Greater amount of spacing in the lower arch. Normal inclination of mandibular incisors.
Pretreatment Cephalometric Analysis
Treatment Objectives
Distalization of the mandibular dentition.
Closure of the upper and lower spaces.
Attain positive overjet with Class I canine and molar relationships and attain midline harmony.
Improve maxillary incisor visibility and reduce lower lip projection.
It was decided to use miniscrew anchorage from the external oblique ridges buccal to the mandibular second molars for distalization of the mandibular dentition. Face mask wear would counter the expected retroclination of the maxillary anterior teeth during upper space closure. This was expected to assist in obtaining a positive overjet and improved maxillary incisor display on smiling.
Treatment Progress
An acrylic splint was bonded to the maxillary posterior teeth with glass ionomer cement. Maxillary dental protraction was then begun with extra-oral elastics (6.5 oz, 3/16") worn from a Petit-type face mask to bilateral hooks incorporated in the splint.
The direction of the pull was forward and approximately 30 degrees downward from the occlusal plane. The patient was instructed to wear it for at least 8 hours every night.
The mandibular dentition was bonded with the pre-adjusted edgewise appliance (0.022", MBT prescription). Lower leveling and alignment were begun with 0.014" HANT wire, initially bypassing the severely rotated 45 (Figure 4).
The lower arch was leveled up with a 0.019" × 0.025" HANT wire. Meanwhile, segmental alignment and consolidation of the maxillary incisors were initiated (Figure 5).
Maxillary Face Mask Wear and Lower Alignment With 0.014" HANT Wire

Upper Incisal Segment Leveling and Lower 0.019" × 0.025" HANT Wire

Distalization of the mandibular dentition was accomplished with a 0.019" × 0.025" SS wire using anchorage from titanium miniscrews (diameter 1.5 mm and length 11 mm) placed in both external oblique ridges.
In each case, buccal nerve block was administered and a short linear incision made through the alveolar mucosa down to the periosteum of the external oblique ridge, buccal to the mandibular second molar. A micromotor pilot drill (diameter 0.9 mm) was used to penetrate the cortical layer under copious irrigation, following which the miniscrew was manually inserted. The use of a relatively long miniscrew ensured that the head remained accessible for placement of attachments after primary stability was achieved.
To each miniscrew head was ligated a stainless steel ring (internal diameter 3 mm) manually fabricated from a hard round stainless steel wire (0.7 mm, Leone, Italy). Power chains were threaded through these rings and both ends attached to the soldered archwire retraction hooks, applying a distalizing force of 300 g on each side (Figure 6). The power chains were changed at monthly intervals.
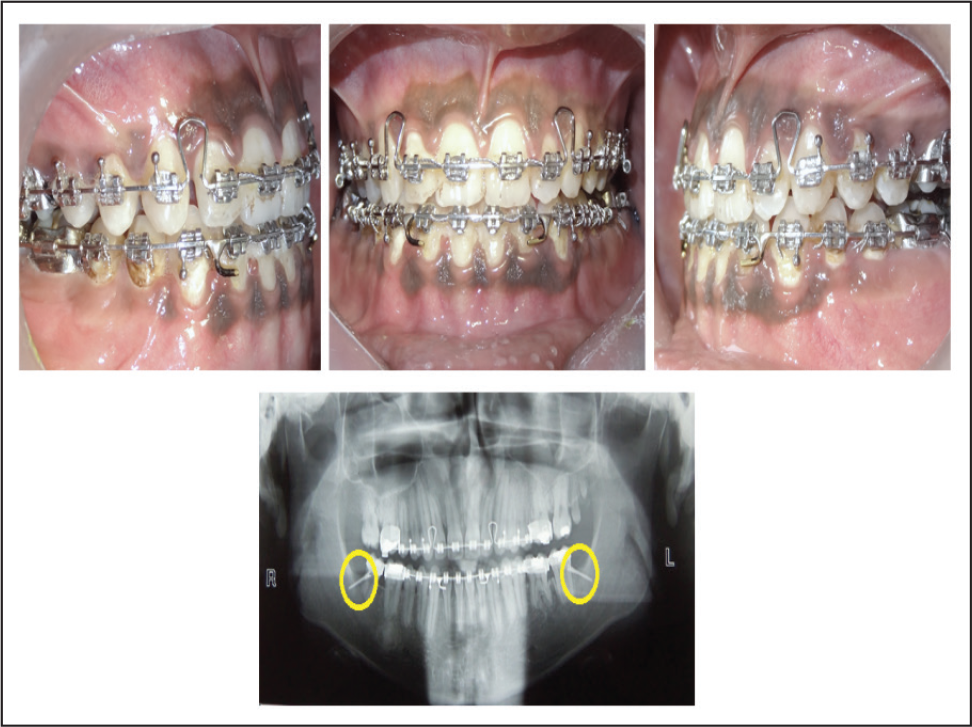
Lower Retraction on 0.019" 0.025" SS Wire With Miniscrew Anchorage From External Oblique Ridges (Miniscrews in the Radiograph Encircled in Yellow)

Upper Space Closure Using Tear Drop Loops With 0.019" × 0.025" SS Wire (Miniscrews in the Radiograph Encircled in Yellow)
Seventeen months following treatment initiation, positive overjet was obtained after which the acrylic splint was removed and the face mask wear temporarily discontinued. The maxillary arch strap-up was completed and alignment resumed with sequential placement of continuous HANT wires.
Following lower space closure, the miniscrews were unloaded but left in place in case of further requirement. Residual spaces distal to the maxillary lateral incisors were closed using tear drop loops bent into 0.019" × 0.025" SS wire (Figure 7). During this period, the patient wore intra-oral elastics (3.5 oz, 1/8") in a Class III configuration during the daytime and from the face mask to the tear drop loops at night to tax the posterior anchorage and thereby prevent retroclination of the maxillary incisors.
Lingual root torque was also incorporated into the incisal segment of the wire. Orthopantomogram taken at the end of space closure showed acceptable root positions and mandibular miniscrews still in place (Figure 7).
Following occlusal settling, the fixed appliances and miniscrews were removed. Total treatment time was 31 months. FSW lingual retainers were bonded to prevent reappearance of spaces, and a removable retainer wear was instituted for a period of 1 year.
Treatment Results
Class I molar and canine relationships with normal overjet and overbite were achieved. All spaces were closed, and the dental midline discrepancy was corrected. Lower lip protuberance was reduced. Overall, the facial appearance was enhanced with an improvement in the nose-lip-chin relationship and maxillary incisor display on smiling (Figures 8 and 9).
Posttreatment Extra-Oral Views

Posttreatment Intra-Oral Views

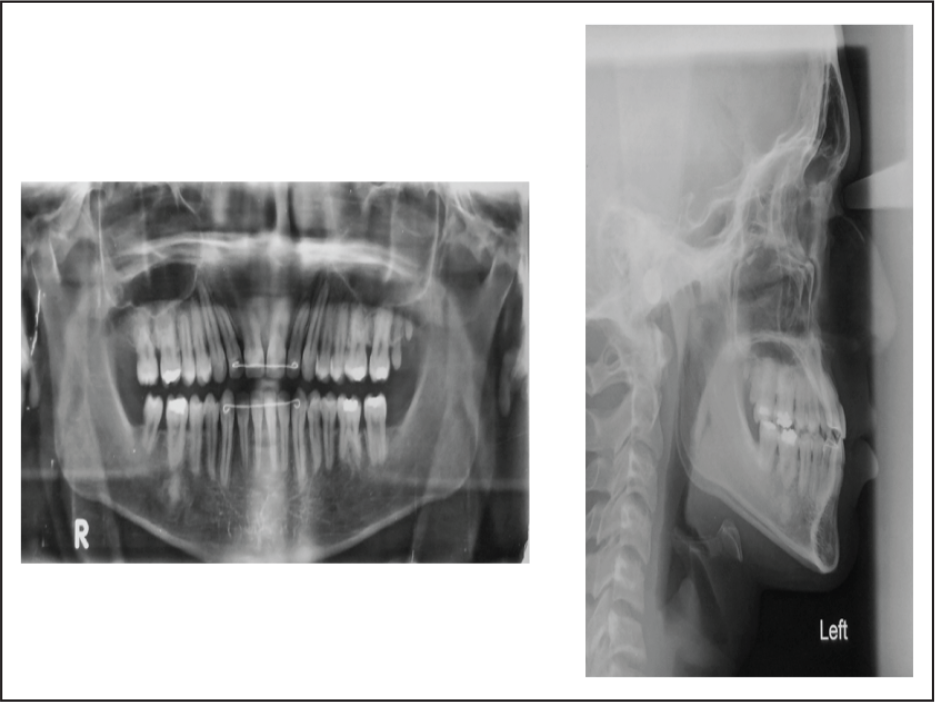
Posttreatment orthopantomogram showed acceptable root positions and no evidence of root resorption (Figure 10).
Posttreatment Radiographic Views
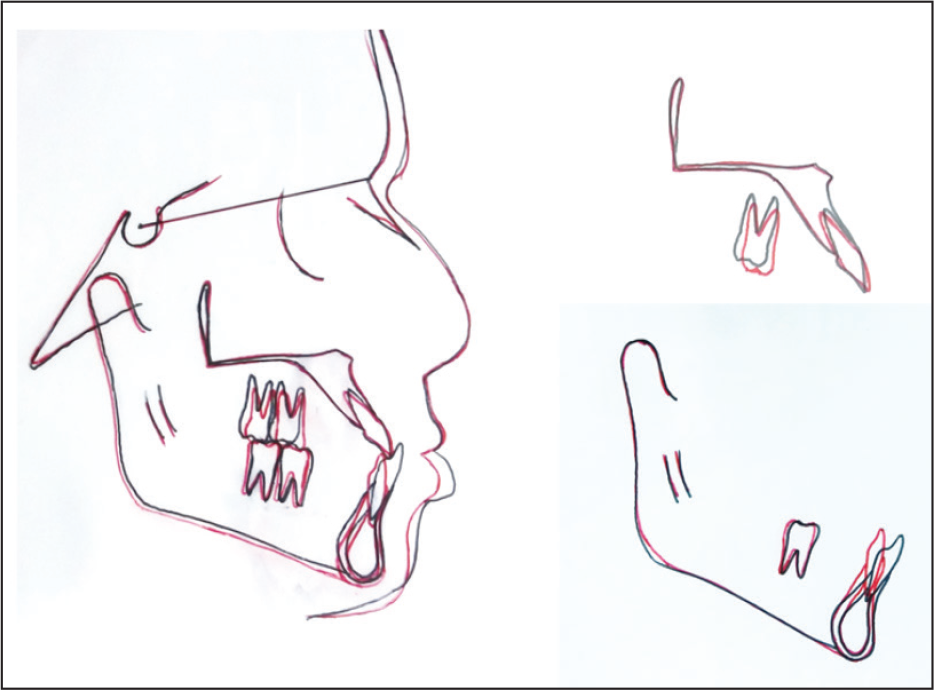
Cephalometric Superimpositions
Posttreatment Cephalometric Comparisons
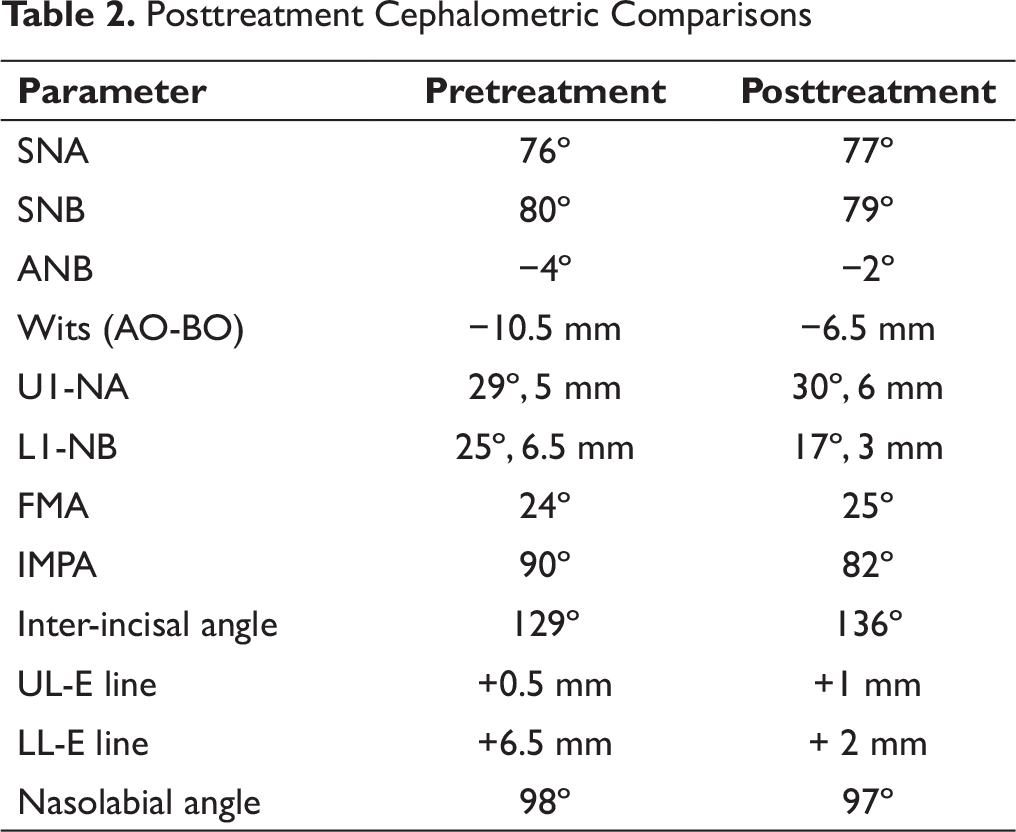
Superimpositions of pre- and posttreatment cephalometric tracings are shown in Figure 11. Cephalometric changes are summarized in Table 2.
ANB and Wits relationships were improved, upper incisors tipped labially, lower incisors were uprighted, and FMA angle increased by 1º. The upper lip was slightly protruded, whereas the lower lip protuberance was reduced.
Discussion
Class III malocclusions are among the most challenging orthodontic cases to treat. While growth modification may be successfully attempted in children and adolescents, adults are usually treated with surgery or camouflage depending on the severity of the skeletal discrepancy.
Chung et al 5 described the use of an interdental C-implant and sliding jig for distalization of the mandibular dentition. Sugawara et al 6 described the use of retromolar miniscrew with titanium coil springs for distalization of the mandibular dentition.
Lee et al 11 cautioned that during miniscrew placement in the retromolar area, there is a possibility of inadvertent injury to nearby anatomic structures such as the mandibular canal and lingual nerve. Opposing teeth or the maxillary tuberosity can also restrict the vertical clearance available for miniscrew placement. They mentioned the external oblique ridge or buccal shelf of the mandible as a possible site for miniscrew placement due to its thick cortical bone and abundant mesio-distal space, which does not restrict tooth movement. It is also a safe area due to the absence of anatomic structures such as nerves, vessels, or dental roots.
In this case, miniscrew anchorage from the external oblique ridge was successfully used to distalize the mandibular dentition for correction of anterior crossbite and establishment of normal overjet.
Class I molar relationships were achieved through mesial movement of the maxillary molars and some distal uprighting of the mandibular molars, as suggested by cephalometric superimpositions. Slight clockwise rotation of the mandible still occurred, possibly due to extrusion of maxillary molars.
Conclusions
Successful camouflage treatment of this adult patient with skeletal Class III malocclusion may be attributed to the use of absolute anchorage for distalization of the mandibular dentition, as well as excellent compliance with face mask wear.
Orthognathic surgery may have achieved a better overall esthetic result, but it would have involved greater cost and morbidity risk.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.