
Abstract
Abstract
Over the years, several methods for delivering fixed lingual retainers have been introduced. However, the accurate and passive placement of the retainer in any clinical situation has always been a matter of concern. This article presents a precise method for placement of a fixed retainer using resin tubes formed from commercially available molds. This method ensures accurate, passive placement of fixed retainer in any clinical situation. Additionally, the same technique can be used for correction of minor crowding relapse by placing an active lingual retainer.
Introduction
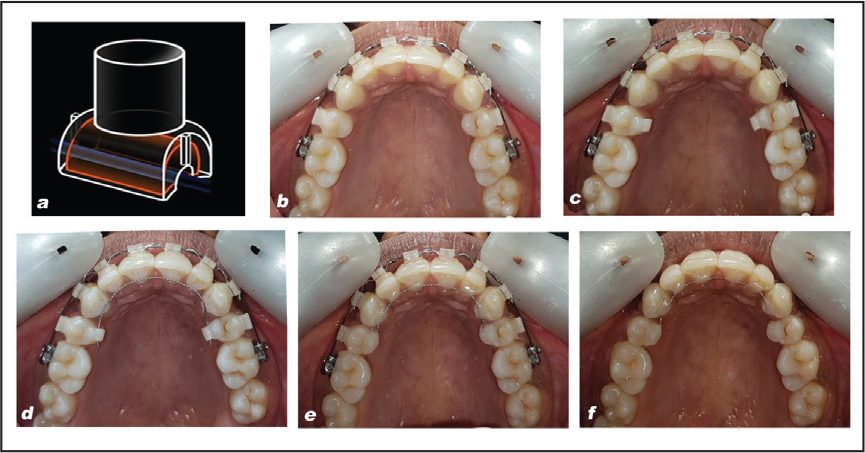
Since the introduction of fixed retainers, their use has steadily grown, and several methods1, 2 for delivering fixed retainers have been introduced. However, precise passive placement of the retainer has always been a matter of concern. To overcome this, a method for precise placement of fixed retainers in any clinical situation is described using resin tubes formed by tube molds (Figure 1[a]) supplied in Mini Molds™ kit (G&H orthodontics, Earlywood Drive, Franklin, IN, USA).
Bonding Procedure
Prepare the labial or lingual surfaces of the teeth to be retained for bonding. First, it is important to clean and optionally sandblast (Al2O3, particle size of 80-125 mm) teeth surface to be bonded. Rinse the sand off and etch with 35% phosphoric acid for 30 seconds. Rinse again, dry thoroughly and keep a dry oral environment (Figure 1[b]).
Resin tube is directly prepared on the last tooth to be bonded on each side using tube molds. The mold is filled with a flowable composite (e.g., Filtek Supreme XT from 3M Espe, Saint Paul, MN, USA) and with the help of an application handle it is secured as gingivally as possible on the tooth surface to be bonded. The same procedure is repeated on the other side of the last tooth to be bonded (Figure 1[c]).
A multistranded 0.0215- or 0.0195-in wire is placed through the lumens of both resin tubes and adapted to the remaining teeth passively (Figure 1[d]).
Excess wire is cut, leaving 1 mm to 2 mm extending from the distal end of each resin tube (Figure 1[d]).
Adapted wire is bonded to teeth using a good quality flowable composite (Figure 1[e]) (e.g., Filtek Supreme XT from 3M Espe, Saint Paul, MN, USA).
After bonding all the teeth between the resin tubes, the lumen of the tube is filled with flowable composite and light-cured.
The closed resin tubes are slightly bulky and need recontouring using finishing burs (Figure 1[f]).
(a) Tube Mold (b) Prepared Lingual Surface (c) Resin Tubes Formed Using Molds (d) Adapted Multistranded Wire (e) After Bonding With Flowable Composite (f) Finished and Polished Retainer.
Discussion
This method is quick and simple, requiring no additional custom-made devices for stabilization to keep the retainer wire from moving during the bonding process. The wire can be easily adapted directly in patient’s mouth; thus, there is no need of adaptation on model or any transfer jigs. This method can be used on any surface, lingual or buccal, and any number of teeth depending on need of the case. In every case, the last teeth on either side of the retention area receive resin tubes except in mandibular first premolar extraction cases where canines will receive tubes and extra distal wire is adapted in mesial fossa of second premolar. Because of its precise placement, bond failures are minimal compared to other techniques. This technique is especially useful in maxillary lingual area where placement of fixed retainer is difficult and prone to fracture. 3 In minor relapse of mandibular anterior crowding, a preformed nickel-titanium wire can be passed through the resin tubes placed on canines and bonded to malposed teeth to bring them in alignment. 4 The same wire can then be converted to a fixed retainer.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.