
Abstract
Abstract
The present paper describes a technique for intermittent replacement of missing anterior edentulous spans which in simple, logical, less time consuming and cost-effective. The objective was to incorporate a rigid framework as a long edentulous span had to be replaced, along with miniscrews at two different angulations, thus restricting the effect of perioral and masticatory forces in an effective manner
Introduction
A beautiful and attractive smile is a primary concern not only at the end of an orthodontic treatment but also during the treatment. It is a substantial clinical problem to replace congenitally missing or accidently lost anterior teeth in young patients.
There are two basic treatment options for patients with missing teeth: space closure or space opening and maintenance of that space for prosthetic replacement. 1 Various methods can be used for the temporary restoration of missing anterior teeth. They are as riding pontic on archwire, acrylic cantilever flange supporting a prosthetic tooth, prosthetic tooth directly bonded to the adjacent tooth, or Maryland bridge. 2
Patients with remaining facial growth are not recommended osseointegrated implants for an obvious reason that, unlike natural teeth, these implants will submerge as the surrounding dentition erupts.3,4 An arbitrary age for the placement of osseointegrated implants was suggested as 15 years for girls and 18 years for boys notwithstanding the growth pattern variations in individuals.5-7
The use of orthodontic miniscrews for interim restorations of missing anterior teeth was first advocated in the 1997 followed by many case reports in the subsequent years. 3 Miniscrews were placed along the long axis of teeth8,9 as well as perpendicular to the palatal mucosa of the edentulous area. 10 This method has obvious retentive, hygienic, and aesthetic benefits as the patient does not need to remove the artificial teeth, the patient can brush as well as floss normally, and they are esthetically acceptable. It is also said to prevent ridge atrophy while averting adjacent roots from drifting into the edentulous space. 11 Pontic does not create unwarranted forces on the archwire due to accidental biting and avoids distortion of unsupported archwire segment.
Case Report
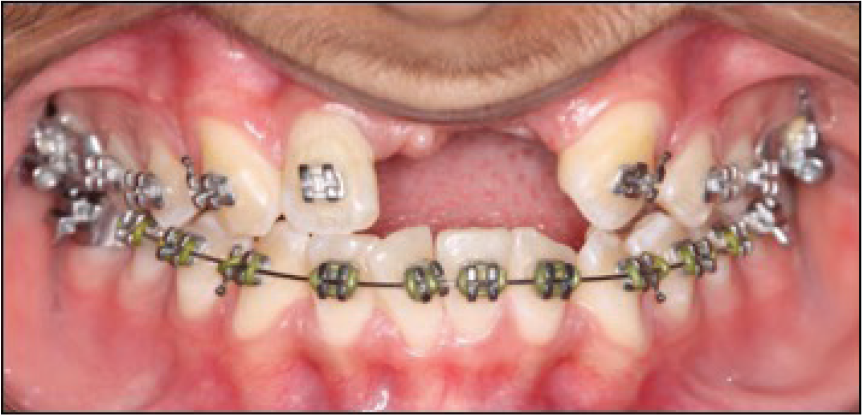
A 13-year-old male patient reported with a chief complaint of missing upper anterior teeth (Figure 1) and malaligned lower anterior teeth. Riding pontic was one of the treatment modalities for replacing anterior edentulous span, but as edentulous span was long, the stability of the pontics was questionable, and it was decided with the patient to place a miniscrew supported pontic attachment for replacing the anterior teeth till cessation of growth.
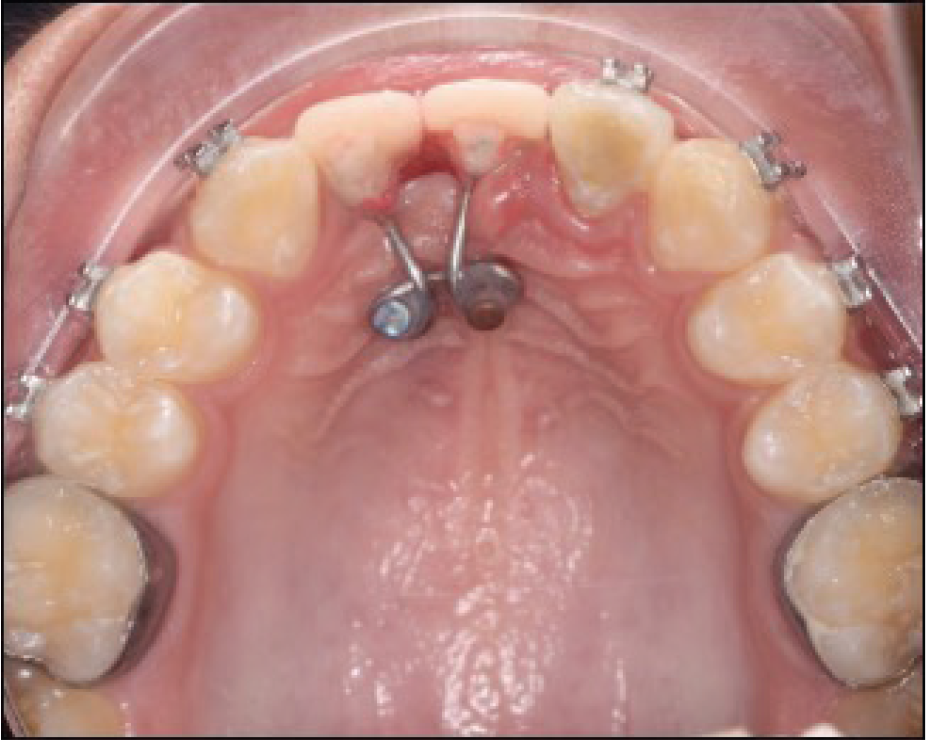
Shade matching, mesiodistal width, and height determination of the pontic were done followed by bending a 0.036-inch wire framework that consists of two loops to hold the miniscrews and extensions for supporting the pontics, which were attached with self-cure acrylic resin (Figure 2). The assembly was placed intraorally and stabilized with two miniscrews (1.8 × 8 mm, 1.8 × 10 mm, FavAnchor SAS, India) placed using a palatal driver (L’il One Driver; FavAnchor SAS, India) as follows:
Patient with anterior edentuluous span
Occlusal view
Radiograph depicting angulation and size of miniscrews
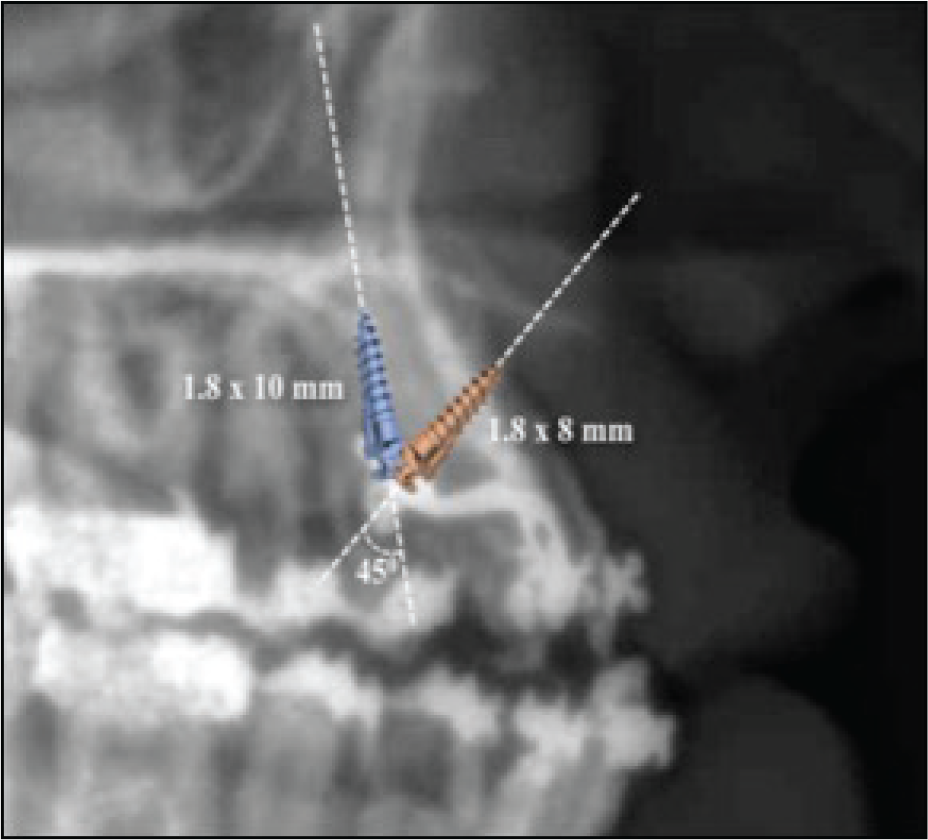
Miniscrew 1: A 1.8 × 8 mm miniscrew was placed across the alveolar ridge for a bicortical engagement for increased stability (Figure 3).
Miniscrew 2: A 1.8 × 10 mm miniscrew was placed at an angle of 45 degrees to the first miniscrew, restricting the effect of rotational forces and increasing the mechanical retention (Figure 3).
Advantages
The advantages are as follows:
Increased stability owing to the rigid wire framework as a large edentulous span was to be replaced.
The pontic can be modified in width or height, as and when required by grinding or adding composite resin.
Claims to maintain alveolar bone density, vertical development, and morphology of the alveolar process.
The direction of miniscrew placement can be planned according to the available bone and adjacent anatomic structures.
Improved patient compliance and hygiene maintenance.
Tooth movement of adjacent teeth is not affected, as pontic is devoid of their support.
Different angulations of miniscrews warrant different rotational axes, thus giving a significant boost in terms of stability as it will help to resist the perioral muscular forces as well as masticatory forces better.
Problems with Conventional Pontic
The problems with conventional pontic are as follows:
Labiopalatal rotational control of the riding pontic is difficult with initial aligning wires; however, it is more stable with the rectangular wires used later during the course of the treatment. 12
Bond failure of the pontic may occur during the treatment. 13
Enamel reduction of healthy teeth is required for almost all fixed options.
Ideal gingival contours, alveolar bone height, or aesthetics are not certain.
The common limitation to all of the above is the fact that none of the fixed or removable methods administered prevent alveolar bone resorption over time in the location of the missing teeth. In fact, the lack of alveolar loading promotes alveolar bone loss. 14
Conclusion
It has always been a clinical enigma to replace anterior teeth in growing individuals. With the help of miniscrews, the crestal and buccolingual alveolar bone volume is preserved until the completion of facial growth and the patient need not remove the retainer or pontic. Every other treatment option can possibly lead to disuse atrophy of alveolar bone, which often calls for bone grafting in the future. Anterior teeth angulation and the angulation of the placement of miniscrews in the available bone usually do not coincide, and thus, this approach using a wire framework mimics the use of angulated abutments as used in oral implantology to compensate for ideal prosthetic placements.
The possibility of an interim restoration with a miniscrew and an acrylic teeth assembly (Figure 4) is an appealing and viable alternative for a patient who is yet to finish growth. The replacement of missing anterior teeth during treatment is favorable in improving various functional factors and elevating self-confidence and motivation level of the patient.
Frontal view

Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.