
Abstract
Owl monkeys are nocturnal primates in the genus Aotus that range across a wide variety of arboreal habitats from Central to South America. Owl monkeys are an important animal model for malaria research. Despite decades of use as a laboratory animal model, disease of the hepatobiliary system is rarely described in this species. The exception is cholelithiasis, which has been reported in the species as an incidental finding with minimal serum chemistry derangements or histologic evidence of disease. However, a retrospective analysis of clinical histories and necropsy reports from owl monkeys housed at the Keeling Center as part of the Owl Monkey Breeding and Research Resource identified 7 cases of obstructive hepatopathy associated with chronic cholecystitis (3/7) and cholelithiasis (4/7). Secondary sclerosing cholangitis was identified in 3/7 monkeys. Elevated gamma-glutamyl transferase was associated with obstructive disease and was increased in 6/6 animals with available bloodwork. Gross lesions included gallbladder distension (5/7), cystic dilation of the common bile duct (1/7), and gallbladder atrophy (1/7). Histologic lesions included moderate to severe submucosal and periductular fibrosis, bile duct hyperplasia, biliary mucosal hyperplasia, and luminal narrowing. A single case had squamous metaplasia of the gallbladder, intrahepatic duct, and common bile duct epithelium. This report defines the clinical syndrome associated with obstructive biliary disease, including ultrasound and serum chemistry derangements, and describes the associated gross and microscopic lesions.
Owl monkeys (Aotus spp.) are small nocturnal arboreal nonhuman primates whose native habitat spans countries of Central and South America. 26 Several species of owl monkey, including Aotus nancymai, Aotus azarae infulatus, Aotus griseimembra, and Aotus vociferans, are kept as research populations for use in biomedical research. Owl monkeys are susceptible to human and nonhuman primate strains of malaria and have been primarily used for malaria research including maintenance of malarial strains, host-vector investigations, and evaluating candidate vaccines and potential therapeutics.16,17,19,20 Additional research uses include ophthalmological and reproductive investigations.12,15
In health, the biliary tree functions to move the bile from the hepatocytes via the canalicular network to the common bile duct into the duodenum. Cholestasis can originate from altered function of the hepatocytes (hepatocellular cholestasis) or from obstruction of the gallbladder or biliary tree (obstructive cholestasis). 10 The biliary tree comprises the intrahepatic bile ducts, extrahepatic left and right bile ducts that join to form the common bile duct, the gallbladder, and the cystic duct that enters at the ampulla into the duodenum.9,10,42 Obstructive cholestasis can result from chronic inflammation, intraductal choleliths, pancreatic disease, neoplasia, or iatrogenic damage to the bile duct.10,34
Little is known about the gallbladder and common bile duct spontaneous pathology that occurs in Aotus spp except cholesterol cholelithiasis.3,6,43 Previous reports have suggested cholelithiasis is an incidental finding at necropsy because the liver and gallbladder did not have histologic evidence of disease associated with obstruction.6,14 Other research populations of neotropical nonhuman primate species have also been diagnosed with spontaneous cholelithiasis including squirrel monkeys (Saimiri spp.), common marmosets (Callithrix jacchus), and other members of the Callithrichidae family (marmosets and tamarins).11,24,38 In addition, choleliths can be induced through dietary changes in Aotus spp., Saimiri spp., and Cebus spp., and these species have potential to serve as models for human disease.3,5,27,29,30,32,41
The goal of this study was to define the clinical syndrome associated with obstructive biliary disease, including ultrasound and serum chemistry derangements, and to describe the gross and microscopic findings associated with obstruction.
Materials and Methods
Animal Welfare
The University of Texas MD Anderson Michale E. Keeling Center for Comparative Medicine and Research houses 4 species of owl monkeys: A. nancymai, A. vociferans, A. azarae, and A. griseimembra. All procedures involving animals were conducted in compliance with all applicable regulations with oversight by the MD Anderson Cancer Center Institutional Animal Care and Use Committee. Animal care and husbandry conformed to practices established by AAALAC, The Guide for the Care and Use of Laboratory Animals, and the United States Department of Agriculture Animal Welfare Act and Animal Welfare Regulations. 28
All animals were housed in compatible social groups unless health status necessitated temporary individual housing for supportive care. Animal housing rooms were maintained at 75–80°F with a relative humidity between 50% and 70% and at least 10 complete air changes per hour. A 12:12-hour light-dark cycle was maintained in animal rooms. Animals were housed either in 48″ deep × 60.5″ high × 36″ wide Britz cages or 28″ deep × 31.5″ high × 32.75″ wide stainless steel cages with synthetic polymer thermoneutral nest boxes and a variety of physical enrichment including ladders, barrels, and manipulanda. Animals were fed Teklad 7195, Hi-Fiber Primate diet supplemented with daily produce items (eg, oranges, sweet potato, peanuts, and meal worms). Animals had ad libitum access to reverse osmosis treated drinking water via a lixit system.
Case Selection
Medical and necropsy records from a 17-year period (2008–2025) at the Keeling Center were queried for clinical histories (including serum chemistry derangements, clinical signs, and ultrasonographic reports) and necropsy reports that cited significant gallbladder and common bile duct pathology. All animals were experimentally naïve and were maintained as part of the Owl Monkey Breeding and Research Resource. Animals included in this study either died spontaneously or were euthanized by intravenous sodium pentobarbital overdose while anesthetized in accordance with the American Veterinary Medical Association Guidelines for Euthanasia. 23
Four cases received abdominal ultrasonographic exams performed by a board-certified laboratory animal veterinarian specialized in nonhuman primate medicine using an Esaote MyLab Class C ultrasound unit (Esaote North America Inc., Fishers, Indiana) with an LA523 probe. 40
Necropsy and Histology
At necropsy, a standard tissue list was collected representing all major organ systems according to institutional standard operating policy in 10% neutral-buffered formalin and were routinely processed, embedded, and stained with hematoxylin and eosin. Necropsy and histologic evaluation were performed by board-certified veterinary anatomic pathologists. Selected samples were evaluated with Masson’s trichrome to evaluate fibrosis and periodic acid-Schiff to evaluate mucin. Selected slides were digitally scanned with an Aperio CS2 Slide Scanner (Leica).
Serum Chemistry and Complete Blood Count
For selected animals, up to 1.5 ml of blood was collected via venipuncture and placed in K2EDTA tubes (BD vacutainer Ref. No. 367841) and/or red top tubes (BD vacutainer Ref. No. 366688) for processing. Complete blood counts were performed using whole blood collected in K2EDTA tubes and measured on the Siemens Advia 120 Hematology Analyzer. Serum chemistries were evaluated from whole blood collected in red top tubes. Serum was separated by centrifugation at 1300 × g for 10 minutes, and chemistry parameters were measured on the Beckman Coulter AU680 Chemistry Analyzer. Values for serology and hematology were compared with in-house reference intervals for Aotus species.
Results
Clinical Presentation and Serum Chemistry
A total of 305 records were available for review, and biliary tree disease was diagnosed in 7 animals (2.295%) with a median age of 17 years. The species involved included 4 A. nancymai (1 male, 3 females), 2 A. azarae (1 male, 1 female), and 1 female A. griseimembra (Table 1).
Signalment, diagnosis, and disease features of Seven owl monkeys with biliary disease.
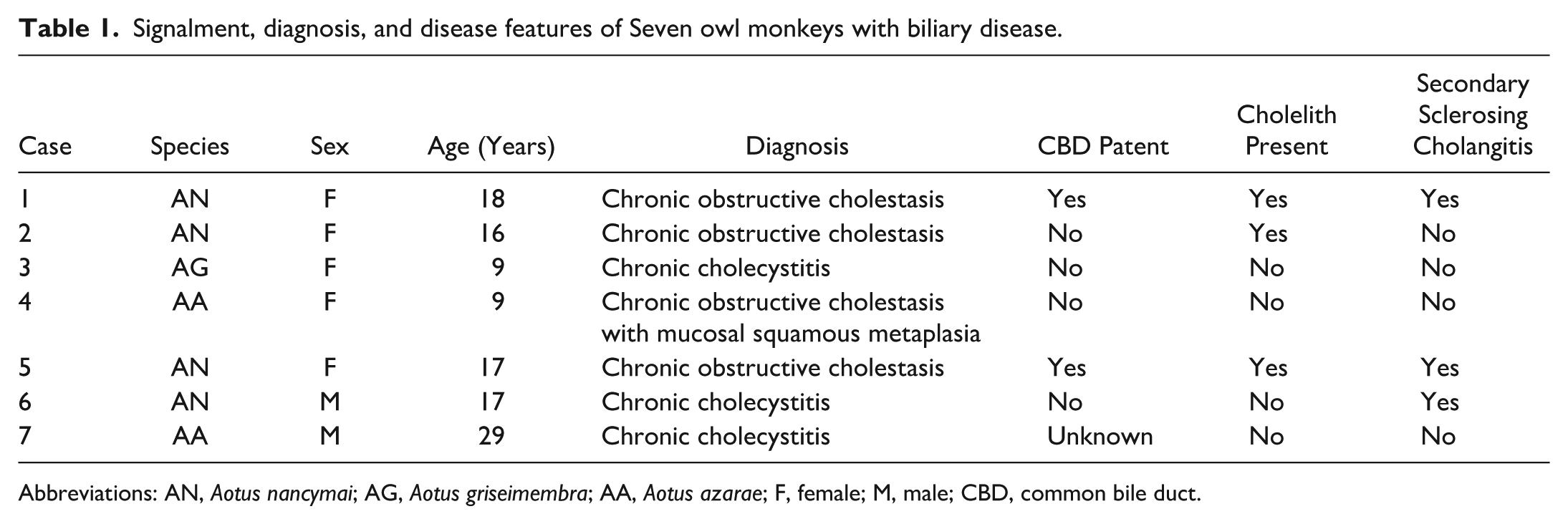
Abbreviations: AN, Aotus nancymai; AG, Aotus griseimembra; AA, Aotus azarae; F, female; M, male; CBD, common bile duct.
The most consistent clinical sign was gradual weight loss, which occurred in 4/7 animals. One animal (case 4) was found dead and had no supporting clinical information. Five cases had a single time point of serum chemistry results available for review (Table 2). One case (case 7) had serial serum chemistry results available for review (Table 3). Elevated gamma-glutamyl transferase (GGT, 6/6) and hyperbilirubinemia (3/6) were the most common chemistry changes associated with gallbladder and common bile duct disease, although 4/6 animals also had increased cholesterol and/or triglycerides (Table 2). Abdominal ultrasounds on 4 cases (cases 2, 5, 6, and 7) revealed hepatomegaly and distended gallbladders with hyperechoic to mixed echogenic material in the lumen (Supplemental Figures S1a–d).
Serum chemistry derangements associated with obstructive hepatopathy.
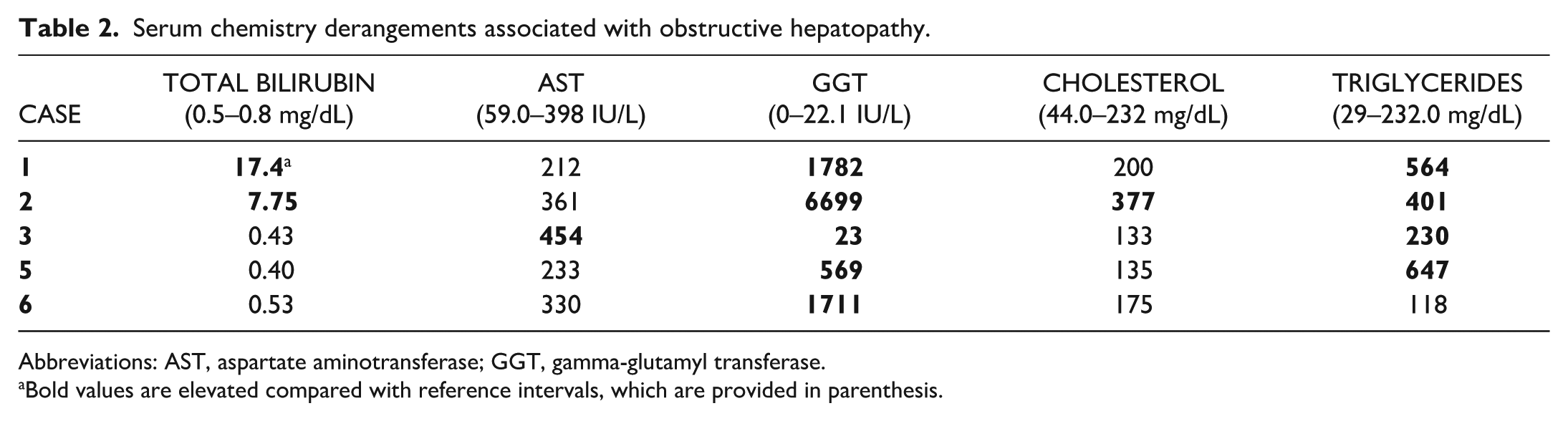
Abbreviations: AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase.
Bold values are elevated compared with reference intervals, which are provided in parenthesis.
Serial serum chemistry results from case 7, 29-year-old A. azarae with intermittent cholestasis.
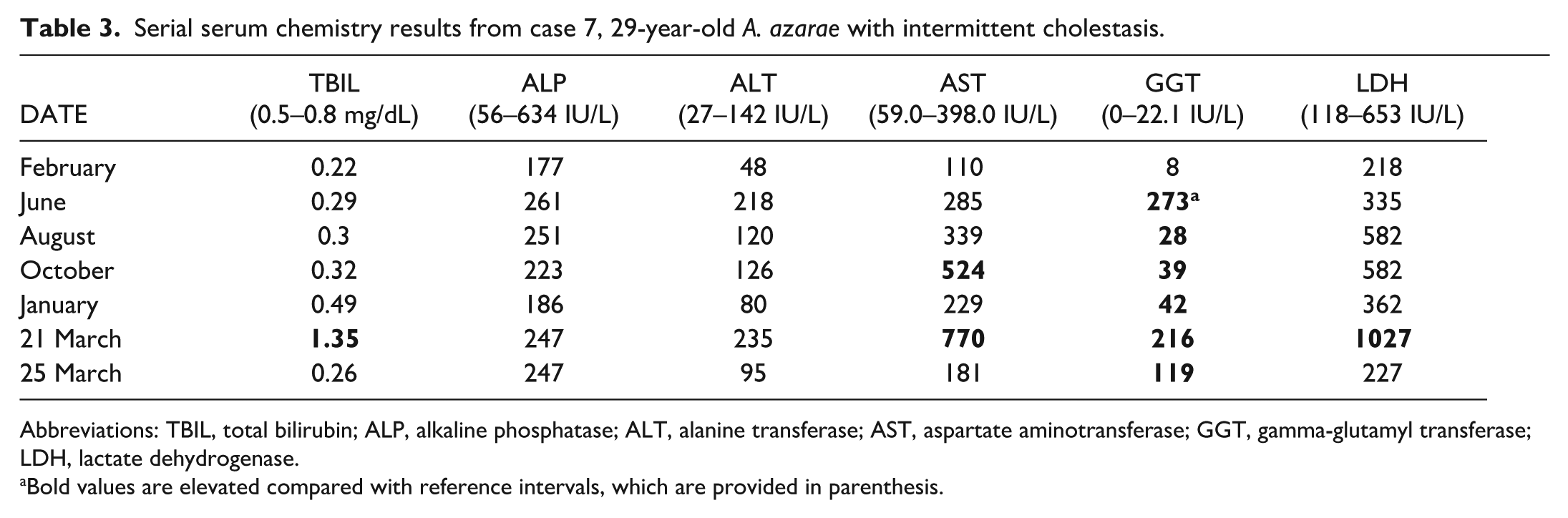
Abbreviations: TBIL, total bilirubin; ALP, alkaline phosphatase; ALT, alanine transferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; LDH, lactate dehydrogenase.
Bold values are elevated compared with reference intervals, which are provided in parenthesis.
Gross and Histologic Lesions
Case 1
On gross examination, the liver of case 1 (18-year-old, female A. nancymai) was diffusely enlarged (4.23% body weight; Supplemental Table S1), orange-tinged, and firm. The common bile duct was tortuous with multifocal cystic diverticuli (Fig. 1a). The gallbladder was distended by 12 ml of yellow-tinged fluid with black to dark green granular material, but bile could be expressed into the duodenum. Upon opening the common bile duct, the lumen contained dark green to black sludge, and the wall was thickened up to 1.5 mm.

Gross and microscopic lesions of obstructive hepatopathy, owl monkey.
Histologically, multiple transverse sections of the gallbladder, common bile duct, and intrapancreatic duct had mucosal hyperplasia with severe submucosal fibrosis that narrowed the lumen (Fig. 1b). The lamina propria and submucosa of the gallbladder were infiltrated by multifocal nodular aggregates of lymphocytes. Brown amorphous material, interpreted as cholesterol, was multifocally closely associated with the mucosa. The hepatic parenchyma had varying amounts of hepatocellular loss with periportal bridging fibrosis and bile duct hyperplasia, and small and medium-sized bile ducts were surrounded by concentric layers of fibrosis with mixed inflammatory cell populations (secondary sclerosing cholangitis). The pancreas at the level of the ampulla had chronic active pancreatitis characterized by neutrophilic and lymphoplasmacytic inflammation, acinar atrophy, and interstitial fibrosis. Multifocally, the arterioles and small muscular arteries of the gallbladder, common bile duct, pancreas, and duodenum had concentric thickening of the media with eosinophilic hyaline material, and the lumen was narrowed, consistent with arteriolosclerosis and arteriosclerosis from systemic hypertension. Similar vascular lesions were also noted in the vessels of the heart and kidneys.
Case 2
Case 2 was a 16-year-old female A. nancymai. The mucous membranes, sclera, and nonhaired skin were icteric, which corresponded with severe hyperbilirubinemia (Table 2). The gallbladder was distended up to 2.2 cm on ultrasound. At necropsy, the liver was diffusely firm with an enhanced reticular pattern, and the capsular surface had an irregular cobblestoned appearance with depressed gray foci, which was especially severe in the caudate lobe. Gross examination confirmed gallbladder distension with dark green to black gritty contents, and bile could not be expressed through the common bile duct.
Histologically, the gallbladder had moderate submucosal fibrosis, and the mucosal folds were flattened (Fig. 1c). The hepatic parenchyma had extensive areas of hepatocellular loss with bridging periportal to centrilobular fibrosis embedded with numerous small bile duct profiles. Remaining hepatocytes had mild-to-moderate cytoplasmic vacuolation consistent with lipidosis. Parenchymal changes indicated end-stage hepatopathy. Small to medium-sized bile ducts were surrounded by fibrosis. The changes were most severe in the caudate lobe in which approximately 95% of the hepatic parenchyma was lost and replaced by dense bands of mature fibrous connective tissue embedded with innumerable small bile duct profiles (Fig. 1d). The small muscular arteries and arterioles of the common bile duct, intrapancreatic duct, and duodenum at the ampulla had moderate to severe concentric medial thickening and hyalinization with rare subintimal eosinophilic deposits, which were associated with inflammation and vascular occlusion. Lesions of mild arteriolopathy and arteriolosclerosis were also noted in the heart and kidneys. Chronic hypertension may have contributed to obstructive hepatopathy by creating transient ischemic events that healed by fibrosis or by increasing portal pressure.
Case 3
Case 3 was a 9-year-old female A. griseimembra with a clinical history of congestive heart failure that had been medically managed for approximately 1 month before clinical endpoints were reached, which included failure to respond to medical management and worsening clinical signs. Gross lesions associated with heart failure were confirmed at necropsy, including tri-cavitary transudate effusions, a globoid heart with multifocal areas of myocardial fibrosis, and brown-tinged lungs from chronic pulmonary hemorrhage. Heart failure was confirmed histologically based on extensive interstitial fibrosis with cardiomyocyte degeneration and multifocal to coalescing areas of pulmonary hemorrhage with heart failure cells (hemosiderin-laden alveolar macrophages). The gallbladder was shrunken, tan, and firm, and bile could not be expressed into the duodenum (Fig. 1e). The liver was diffusely orange and firm with an enhanced reticular pattern, and the capsular surface had an irregularly pitted appearance.
Histologically, the hepatic parenchyma had multifocal areas of acute centrilobular congestion with scattered foci of extramedullary hematopoiesis. The gallbladder mucosa was hyperplastic with multifocal dilated glands containing mucin. The lamina propria was multifocally infiltrated by a small number of neutrophils, and the mucosa was herniated into the submucosa (Fig. 1f). The lamina propria and submucosa were markedly thickened by a mixture of amorphous, lightly eosinophilic material and mature fibrous connective tissue. The final diagnosis was chronic cholecystitis with mucinous hyperplasia.
Case 4
Case 4 was a 9-year-old female A. azarae that was found deceased with no premonitory signs. The presumptive cause of death was gastric bloat, which was supported by a severely gas-distended stomach at gross examination. Significant lesions were noted in the gallbladder, which was markedly shrunken and firm, and only 0.5 cm in diameter at its widest aspect. The gallbladder lumen was empty, and the common bile duct was thickened and tortuous.
On histologic exam, the mucosa of the gallbladder was replaced by metaplastic squamous epithelium and hyperplastic glandular epithelium (Fig. 2a). Multifocally, the submucosal vessels had mural necrosis with acute thrombosis and hemorrhage of the overlying mucosa (Fig. 2a, b). The hepatic parenchyma was disorganized with multifocal regenerative nodules separated by bands of mature fibrous connective tissue with small bile ducts embedded (Fig. 2c). Scattered medium to large intrahepatic bile ducts had squamous metaplasia of the epithelium (Fig. 2c). The submucosa was markedly expanded by mature fibrous connective tissue and had multifocal areas of hyperplastic glandular epithelium (Fig. 2d) surrounded by intense inflammation composed of lymphocytes and plasma cells (Fig. 2d, inset). The mucinous material of the hyperplastic epithelium was positive by periodic acid-Schiff reaction (Fig. 2e).

Squamous metaplasia of the gallbladder and intrahepatic ductular epithelium associated with chronic obstruction. 9-year-old, female Aotus azarae. Case 4.
Case 5
Abdominal ultrasound of case 5, a 17-year-old female A. nancymai, revealed an enlarged liver and distended gallbladder compared with an unaffected control (Supplemental Figures S1a, b). Based on the clinical suspicion of neoplasia causing complete cholestasis, the animal was humanely euthanized and submitted for necropsy. On gross examination, the liver was 37.7 g (4.9% body weight; Supplemental Table S1) with multifocal areas of capsular fibrosis especially along the margins (Fig. 3a). The gallbladder was enlarged and contained dark green to black gritty material. The common bile duct was patent but mildly distended. Within the lumen of the gallbladder and common bile duct, multifocal, 200–400 μm diameter brown concretions interpreted as cholesterol material was closely associated with the mucosa (Fig. 3b–c).

Gross and histologic lesions associated with chronic cholelithiasis. 17-year-old, female A. nancymai. Case 5.
Histologically, the common bile duct mucosa was multifocally attenuated to hyperplastic with papillary projections and foci of dysplasia characterized by loss of nuclear polarity, increased nuclear to cytoplasmic ratio, and loss of the apical brush border (Fig. 3d). The submucosa had mild-to-moderate bands of mature fibrous connective tissue with multifocal aggregates of lymphocytes forming follicles (Fig. 3b). The arterioles and small muscular arteries of the common bile duct had medial hypertrophy and hyalinization with reactive endothelium consistent with hypertension. Similar vascular lesions were noted in the heart and kidneys. The hepatic parenchyma had multifocal areas of hepatocellular loss with compensatory hypertrophy and karyomegaly. Bridging fibrosis spanned portal areas with bile duct hyperplasia.
Case 6
Case 6 was a 17-year-old male A. nancymai with a clinical history of progressive weight loss and alopecia. Abdominal ultrasound revealed an enlarged gallbladder with a mass-like hyperechoic area in the lumen (Supplemental Figure S1c). At necropsy, the gallbladder contents were yellow tinged with plaques of tan friable material, and the mucosa was irregularly roughened and reddened. Bile could not be expressed through the common bile duct, suggesting an obstruction. The hepatic parenchyma had bridging periportal fibrosis with bile duct hyperplasia and a mild infiltrate of lymphocytes, plasma cells, and eosinophils.
Histologic examination of the common bile duct revealed chronic inflammation characterized by submucosal lymphoplasmacytic infiltrates, mural fibrosis, mucosal hyperplasia, and subglandular hyperplasia. Cholelith material was not identified on gross examination or in the histologic sections examined. The primary diagnosis was chronic cholecystitis with luminal stricture of the common bile duct due to lymphoplasmacytic and eosinophilic inflammation and fibrosis. Intrahepatic bile ducts had similar lesions of periductular fibrosis and inflammation resembling secondary sclerosing cholangitis. Mild cardiomyopathy and chronic nephropathy were comorbidities.
Case 7
Case 7 was a 29-year-old male A. azarae with a 1-year history of medical management for waxing and waning changes to GGT and aspartate aminotransferase (AST) (Table 3) and hyperechoic biliary material on ultrasound that suggested an ongoing and intermittent obstructive lesion in the biliary tree (Supplemental Figure S1d). The animal was scheduled for humane euthanasia when ultrasound and clinical pathology changes indicated complete obstruction. The liver was small (3.13% body weight; Supplemental Table S1) and firm. The most significant gross lesion was a small gallbladder with an edematous wall (Fig. 4a). The lumen contained minimal gritty green to black contents and less than 1 ml of yellow-tinged fluid. The common bile duct wall was diffusely thickened up to 2 mm (Fig. 4a). Patency of the common bile duct could not be assessed due to the minimal contents in the gallbladder.

Gross and microscopic lesions from a 29-year-old, male A. azarae with weight loss and waxing/waning clinical signs of obstruction and chronic cholecystitis. Case 7.
Histologically, the gallbladder mucosa was eroded to ulcerated (Fig. 4b) and replaced by an intense infiltrate composed primarily of plasma cells with fewer lymphocytes, macrophages, and eosinophils (Fig. 4c, d). The submucosa had foci of lymphoid hyperplasia and was thickened by bands of mature fibrous connective tissue and mural edema (Fig. 4c). The hepatic parenchyma had mild, multifocal, periportal bridging fibrosis with minimal lymphocytic infiltrate and bile duct hyperplasia. Multifocally, hepatocytes had cytoplasmic lipid vacuolation.
Discussion
The most common diagnosis in this study was obstructive cholestasis secondary to cholelithiasis (4/7). Three cases (3/7) had histologic features resembling secondary sclerosing cholangitis. Obstructive cholestasis and secondary cholangitis have not been previously reported in Aotus spp. even though cholelithiasis has been described.
Cholelithiasis has been observed in owl monkeys and many other nonhuman primate species.3,6,14,21,24,31,35,37,40 The initial reports of cholelithiasis in owl monkeys found no correlation between the presence of choleliths and GGT or AST. 6 GGT is produced by the microvilli of hepatocytes, bile duct epithelium, and renal tubular epithelium but is considered a sensitive enzyme marker for cholestasis, posthepatic obstruction, or obstructive hepatopathy. 7 In the study by Baer et al, 6 only 1 animal of 7 had elevations in GGT to suggest biliary disease. Takeshita et al 40 identified gallstones in 6 of 68 animals evaluated by ultrasound; however, elevated GGT and total bilirubin was only identified in one animal. In this study, GGT was increased in all cases with available bloodwork. Hyperbilirubinemia is also a specific marker for intrahepatic and extrahepatic biliary tree obstruction but was less reliably increased in our study. Icterus was only noted in one animal and was found during sedated exam; cage-side assessment of icterus is difficult in owl monkeys due to their nocturnal nature, thick haircoat, and pigmented skin.
Regarding histopathology, the previous report of cholelithiasis documented no lesions in the gallbladder mucosa, which led Baer et al 6 to conclude that cholelithiasis was an incidental finding. In the cases presented herein, mild-to-moderate gross and histopathologic lesions were noted in the hepatic parenchyma in cases 3, 5, 6, and 7. End-stage hepatopathy from chronic extrahepatic obstruction was identified in cases 1, 2, and 4, and the hepatic parenchyma in these animals exhibited histologic features of chronic extrahepatic cholestasis, including lipid-type hepatocellular vacuolar degeneration and periportal to centrilobular bridging fibrosis with bile duct hyperplasia. Hepatocytes had frequent karyomegaly and polyploidy indicating a regenerative response. Interestingly, even in the case with a total bilirubin of 17.4 g/dL, bile plugs were not observed in the canaliculi or portal bile duct profiles. The gross changes seen in these owl monkeys were similar to those reported in a case report of spontaneous cholelithiasis in a squirrel monkey (Saimiri sciureus), including an irregular capsular surface of the liver and cystic dilation of the common bile duct that contained black hard stones. 24
The gallbladder and common bile duct of 6 of 7 cases in this study had lesions of chronic inflammation including mucosal hyperplasia; submucosal fibrosis; and infiltrates of lymphocytes, plasma cells, and eosinophils in the mucosa and submucosa. Cholelith material was noted in the lumen of the gallbladder and common bile duct in 4 cases at gross exam but was only confirmed histologically in 2 cases. Solid choleliths were rarely seen; instead, the more common presentation was sludgy, friable, bile-stained material. The original report of cholesterol choleliths reported both solid choleliths and more amorphous material.3,6 The friable nature of the material may explain the prolonged clinical course. This material may have created a partial obstruction and slowed the flow of bile leading to intermittent cholestasis and inflammation and fibrosis of the common bile duct mucosa. This hypothesis is supported by the case with serial bloodwork available (case 7), which demonstrated waxing and waning changes in both GGT and AST over a 1-year course of disease progression.
In 3 cases (cases 1, 2, and 4), the submucosal and adventitial vessels of the common bile duct had medial hypertrophy and hyalinization, which is associated with systemic hypertension.8,39 Systemic hypertension is a well-documented comorbidity of zoo and research Aotus and other neotropical species and can result in medial hyalinization of small muscular arteries and arterioles.8,13,39 The submucosal vessels of the common bile duct, intrapancreatic duct, and ampulla had evidence of medial necrosis and intraluminal thrombosis, which may have resulted in focal mucosal necrosis and fibrosis contributing to luminal narrowing and cholestasis. The common bile duct has a poor collateral blood supply and is vulnerable to ischemic events.33,36 We hypothesize that systemic hypertension and resulting arteriolosclerosis of the vasculature of the common bile duct led to transient ischemic events and necrosis of the ductular mucosa of the common bile duct and pancreatic duct. These foci of necrosis were replaced by fibrosis and created a stricture of the duct that decreased the flow of bile and made these locations more vulnerable to intermittent obstruction by sludgy material.
The gallbladder and common bile duct of case 4 was initially diagnosed as neoplasia at the time of necropsy because the gallbladder was replaced by firm tan tissue suggestive of a carcinoma. However, histologic examination revealed a spectrum of hyperplastic and metaplastic lesions associated with chronic obstruction.1,18 The gallbladder epithelium and areas of the intrahepatic and common bile ducts were replaced by squamous epithelium. Metaplastic changes can be a sequela of chronic cholecystitis and may be seen in conjunction with hyperplasia of the glandular epithelium, which was also noted in the case.1,18 Pyloric and intestinal metaplasia are the most common metaplastic lesions diagnosed in the human medical literature and can be associated with chronic obstruction from neoplasms or cholelithiasis. 18 Squamous metaplasia is a more unusual form of metaplasia. 1 In a retrospective morphologic study of the extrahepatic bile ducts in forty-two human patients, squamous metaplasia was only diagnosed in a single individual with an inflammatory stricture of the common bile duct. 18 Squamous metaplasia of the gallbladder epithelium may represent a preneoplastic lesion of carcinoma in situ or squamous cell carcinoma. 1
Secondary changes in the intrahepatic bile ducts were common including periductular fibrosis with a lymphoplasmacytic and eosinophilic inflammatory cell infiltrate and bile duct hyperplasia, which suggests that cholelithiasis resulted in secondary sclerosing cholangitis. Sclerosing cholangitis can be either primary or secondary. Physicians may use magnetic resonance imaging with and without biopsy to confirm the diagnosis.2,25,34 The histologic features of primary and secondary sclerosing cholangitis are similar; in postmortem samples, the diagnosis of secondary sclerosing cholangitis requires concurrent lesions such as pancreatitis, hilar lymphadenopathy, cholelithiasis, ampullary carcinoma, or cholangiocarcinoma.2,25,34 Sclerosing cholangitis is characterized by cholestasis, periductular fibrosis, and nonspecific inflammation, and most cases in the medical literature are associated with markedly elevated GGT and alkaline phosphatase. 34 This type of lesion has been documented in baboons (Papio spp) but is not typically diagnosed in other veterinary species. 4 The diagnosis is almost exclusively made postmortem, and the case details must be correlated retrospectively with any clinicopathologic information such as liver enzymes. In the present series, each case of secondary sclerosing cholangitis was accompanied by a recognized predisposing condition: chronic pancreatitis (case 1), obstructive hepatopathy with cholelith material (case 5), or chronic cholecystitis (case 6). All of these lesions are associated with the development of secondary sclerosing cholangitis in the human medical literature. 34 This lesion has not been reported in spontaneous or experimental cases of cholelithiasis in squirrel monkeys (Saimiri spp.) or owl monkeys (Aotus spp.).
Risk factors for developing choleliths in humans include increased age, high cholesterol diet, and hypothyroidism. 22 The pathogenesis or risk factors for cholelithiasis in owl monkeys have not been confirmed, but a recent paper evaluating the ultrasonagraphic findings in a colony of A. azarae infulatus found no familial relation between animals with choleliths. 40 The A. nancymai cases (1, 2, 5, and 6) have common ancestors on the maternal and paternal side, but the associations are distant and are within expected parameters for a closed breeding group. As in humans, the affected animals in this case series were older (median age affected 17-year-old; range 9–29 years). 44 During the 17-year period for which records were reviewed, owl monkeys were fed a commercial primate diet with high fiber (14.9%) and low fat (5%) supplemented with peanuts, fruits, and vegetables. In an experimental setting, supplementing the diet with 1.5% cholesterol induced cholesterol choleliths within 5 weeks in owl monkeys, which correlated with hypercholesterolemia in males. 30 Based on the diet composition, it is unlikely that diet played a significant role in cholelith development.
Conclusions
This report highlights the clinical signs and spectrum of lesions associated with obstructive cholestasis. The underlying pathogenesis of cholelith formation is not well established and is likely multifactorial. Further studies investigating the genetics or effects of diet could clarify this question and provide practical information to improve animal welfare in zoological and laboratory populations.
Supplemental Material
sj-pdf-1-vet-10.1177_03009858261451486 – Supplemental material for Clinical, gross, and microscopic findings in 7 owl monkeys (Aotus spp) with chronic biliary tree disease
Supplemental material, sj-pdf-1-vet-10.1177_03009858261451486 for Clinical, gross, and microscopic findings in 7 owl monkeys (Aotus spp) with chronic biliary tree disease by Martha E. Hensel, Leqin Yan, Natalie W. Fowlkes, Carolyn L. Hodo and Sarah M. Kezar in Veterinary Pathology
Footnotes
Acknowledgements
The authors gratefully acknowledge Dr Dipen Maru, MD for consulting on several cases. We would also like to thank Dr Gwen Levine, DVM for consulting on the ultrasonography figure. We would also like to thank the animal care staff for their dedicated efforts to support the Owl Monkey Breeding Resource, and the histotechnology staff for providing excellent case materials.
Supplemental material for this article is available online.
Author Contributions
MEH designed the study, analyzed and interpreted the data, and wrote the manuscript. SK analyzed data and wrote the manuscript. CLH, LY, and NWF interpreted the data. All authors reviewed the manuscript and gave final approval.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.