
Abstract
The biological behavior and immunohistochemical features of feline renal cell carcinoma (RCC) have not been well characterized. In the present study, immunohistochemical examinations were performed in 12 feline cases of RCC. The RCC consisted of solid (n = 2), solid-tubular (n = 2), tubular (n = 3), papillary (n = 2), tubulopapillary (n = 2), and sarcomatoid (n = 1) type lesions. Of the cases with RCC, 1 developed metastatic disease and 6 cases had no evidence of recurrence at 80 to 2292 days after surgery. One papillary-type tumor had cuboidal cells with scant cytoplasm and monomorphic nuclei, and the other had pseudostratified columnar cells with abundant cytoplasm. Immunohistochemistry revealed that the tumor cells in most cases were positive for cytokeratin (CK)7, CK20, KIT, and CD10, with the exception of cases of the solid type with clear cytoplasm (solid anaplastic), papillary type with columnar cells, and sarcomatoid types. A small number of tumor cells in the solid anaplastic and in the sarcomatoid types were positive for aquaporin-1. Increased expression of N-cadherin and Twist along with nuclear accumulation of β-catenin were observed in the sarcomatoid type. These results indicated that CK, KIT, and CD10 are relatively strongly expressed in most feline RCC. The solid anaplastic RCC exhibited CD10 expression with the absence of distal tubule marker expression. Although immunohistochemistry profiles were relatively consistent with those described in human RCC, the histopathologic features were different from those seen in humans. Epithelial-mesenchymal transition (EMT) marker expression in the current cases may suggest the involvement of an EMT-like mechanism in the development of sarcomatoid RCC in cats.
Renal cell carcinoma (RCC) is the most common type of primary epithelial renal tumor affecting domestic animals, including cats. 7,34,35 On the basis of their predominant histologic features, RCCs are classified into 3 types: papillary, tubular, and solid. These types can be further classified based on their cytologic patterns into chromophobic, eosinophilic, and clear cell types. 34 Tumor cells of different subtypes are commonly observed in the same lesion, and the differences in biological behaviors of each RCC subtype have not been well defined in cats. 34 Henry et al. 22 reported that tubular and tubulopapillary carcinomas were the most common forms of feline RCC. In humans, sarcomatoid RCC is characterized by the proliferation of both epithelial and mesenchymal components, and epithelial-mesenchymal transition (EMT) is involved in its development. 8,21 Sarcomatoid RCC has also been sporadically reported in cats. 4 However, the role of EMT in sarcomatoid RCC has not been well studied. The present study aimed to investigate the biological behavior and immunohistochemical features of feline RCC. In addition, a case of sarcomatoid RCC was further evaluated using EMT markers.
Materials and Methods
Cases
Twelve cats that were histopathologically diagnosed with RCC at the Laboratory of Veterinary Pathology of the University of Tokyo between 2010 and 2016 were included in this study. Formalin-fixed tissue specimens were obtained through nephrectomy in all cases (n = 12). Survival data were available for 8 of the 12 cats. Normal renal tissues from outside of the neoplastic lesions were used as controls for the immunohistochemical examinations.
Histopathology and Immunohistochemistry
Routinely fixed (24–48 hours in neutral-buffered 10% formalin) and paraffin-embedded archival tissue blocks were sectioned into 4-μm slices. The sections were deparaffinized, rehydrated through a graded series of alcohols, and stained with hematoxylin and eosin and periodic acid–Schiff (PAS). The diagnostic criteria used during the histopathologic evaluations were based on the World Health Organization Classification (Supplemental Table S1). 34 The number of mitotic figures was evaluated per 10 high-power fields 400x, (0.55 mm in diameter) in areas that exhibited a predominant histologic pattern. The Ki-67 labeling index was determined by counting the number of Ki-67–positive tumor cells/1000 cells.
Immunohistochemistry (IHC) analysis of EMT marker expression was conducted in the case of sarcomatoid RCC, as well as in representative cases (Nos. 1, 2, 4, 5, 8, 9, and 10) for comparison. Antigen retrieval procedures were performed. Endogenous peroxidase was inactivated with 3% hydrogen peroxide in methanol at room temperature (RT) for 5 minutes. The sections were then blocked with 8% skim milk in Tris-buffered saline (TBS) at 37°C for 30 minutes. After being incubated with each primary antibody (Supplemental Table S2) at 4°C overnight, the sections were incubated with the Dako EnVision+ System horseradish peroxidase–labeled polymer anti-rabbit/mouse secondary antibody (Dako, Tokyo, Japan) at 37°C for 40 minutes. Next, the sections were washed 3 times in TBS, before being visualized using 0.05% 3,3′-diaminobenzidine and 0.03% hydrogen peroxidase in a Tris-HCl buffer. Normal kidney tissue was used as a positive control. A negative control was prepared by omitting each primary antibody. The proportion of tumor cells that were positive for each marker was classified into 4 categories as follows: negative (–), <25% (+), 25%–50% (++), and >50% (+++).
The co-localization of Twist with either E-cadherin or N-cadherin was further investigated in the sarcomatoid RCC case (No. 12) using a double immunofluorescence technique. In brief, antigen retrieval in citric acid solution (pH 6) was followed by blocking with 8% skim milk in TBS supplemented with 1% Tween 20 (TBST) at 37°C for 30 minutes. After being incubated with the first primary antibodies (E-cadherin or N-cadherin) at 4°C overnight, the sections were incubated with the second primary antibody (Twist) at 37°C for 60 minutes. Following 3 washes in TBST, the sections were incubated with Alexa 488–conjugated goat anti-rabbit IgG (1:200; Invitrogen, Eugene, OR) and Alexa 594–conjugated goat anti-mouse IgG (1:200; Invitrogen) at RT for 60 minutes. The co-expression of either E-cadherin or N-cadherin with Twist was analyzed using a laser-scanning confocal microscope (LSM700; Zeiss, Tokyo, Japan).
Results
Cases
The details of the cases are summarized in Table 1. The ages of the cats ranged from 3.3 to 13.7 years (mean age: 9.9 years). There were 5 neutered males and 4 neutered and 3 intact females. Case 12 involved an American Short Hair cat, whereas the others were mixed breed. The primary tumor seemed to arise from the kidney in all cases. In case 12, sclerotic kidney and an abdominal adhesion involving the kidney, omentum, and left abdominal cavity were observed at surgery. The omental lesion was histologically confirmed as RCC. Although case 6 also formed an adhesion between the renal capsule and the liver, the hepatic sample was not available for histopathology. Case 1 had a history of nasal lymphoma. The clinical presentations varied widely. Five cases showed signs of urinary disorders such as polyuria, hematuria, and anemia. Serum biochemistry results were available in 11 cases (Table 2). Increased hematocrit and hypercalcemia were observed in 6 cases. Serum creatinine was normal but near the upper reference limit in 2 cases. Serum urea levels were elevated in 2 cases. Serum erythropoietin levels were estimated in 3 cases. Two of the 3 cases with increased serum erythropoietin level showed high hematocrit levels that were indicative of secondary polycythemia.
Case Details and Histopathologic Features of Feline Renal Cell Carcinoma.
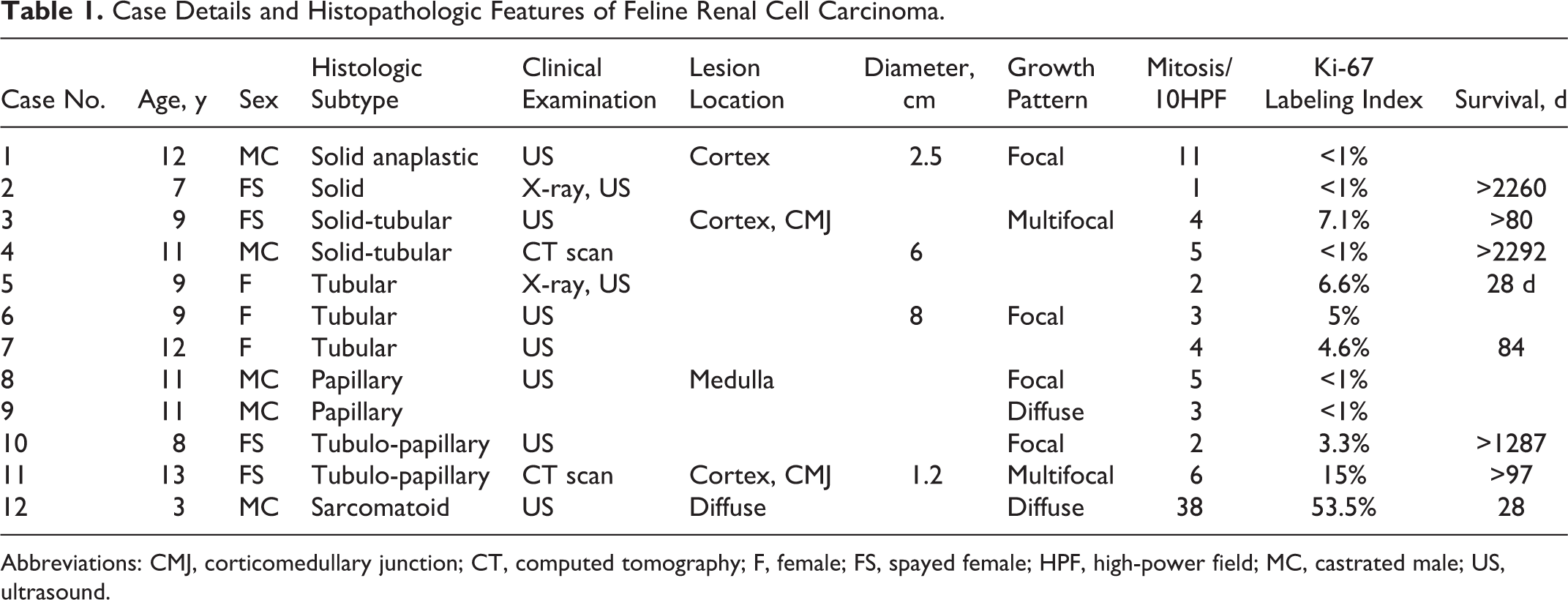
Abbreviations: CMJ, corticomedullary junction; CT, computed tomography; F, female; FS, spayed female; HPF, high-power field; MC, castrated male; US, ultrasound.
Serum Biochemistry Findings in Cats With Renal Cell Carcinoma.
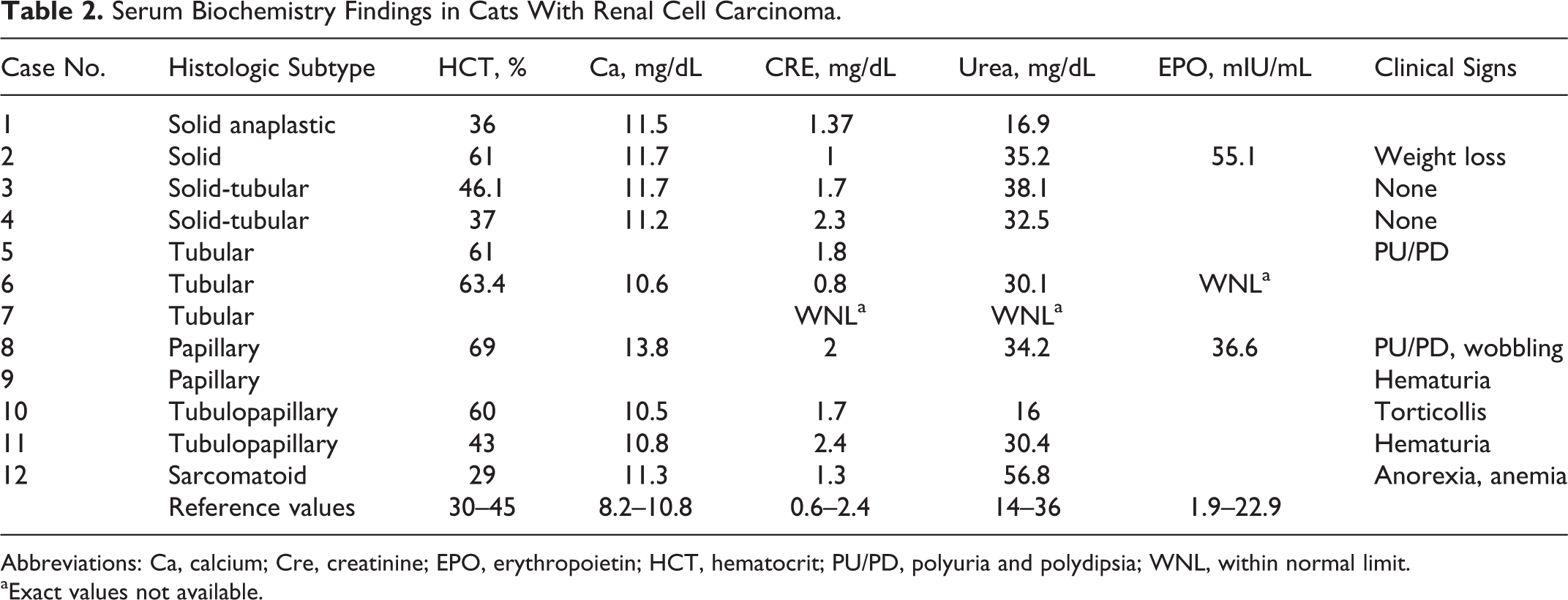
Abbreviations: Ca, calcium; Cre, creatinine; EPO, erythropoietin; HCT, hematocrit; PU/PD, polyuria and polydipsia; WNL, within normal limit.
aExact values not available.
Histopathology
Twelve feline RCC cases were histopathologically classified into solid (n = 2), solid-tubular (n = 2), tubular (n = 3), papillary (n = 2), tubulopapillary (n = 2), and sarcomatoid (n = 1) types. Unilateral renal tumors were found in all cases. Metastatic lesions were detected only in the sarcomatoid case (metastases in the omentum; case 12). Regional lymph nodes were not taken at surgery in any of the cases.
In RCC of solid type with clear cytoplasm (solid anaplastic type; case 1), the tumor cells exhibited a balloon-cell-like appearance. These cells had a high N/C ratio, had frequent vesicular nuclei containing clumped chromatin (Fig. 1a), and often contained irregular cytoplasmic vacuoles with abundant PAS- and Alcian blue–positive material (Fig. 1b). In this case, cholesterol crystals were frequently deposited in the tumor nest. The other case with solid type (case 2) was characterized by sheets of polygonal or round tumor cells with a reticular PAS-positive basement membrane (Fig. 2). The tumor cells had eosinophilic granular cytoplasm with infrequent small cytoplasmic vacuoles and round to ovoid nuclei, which displayed moderate nuclear atypia.
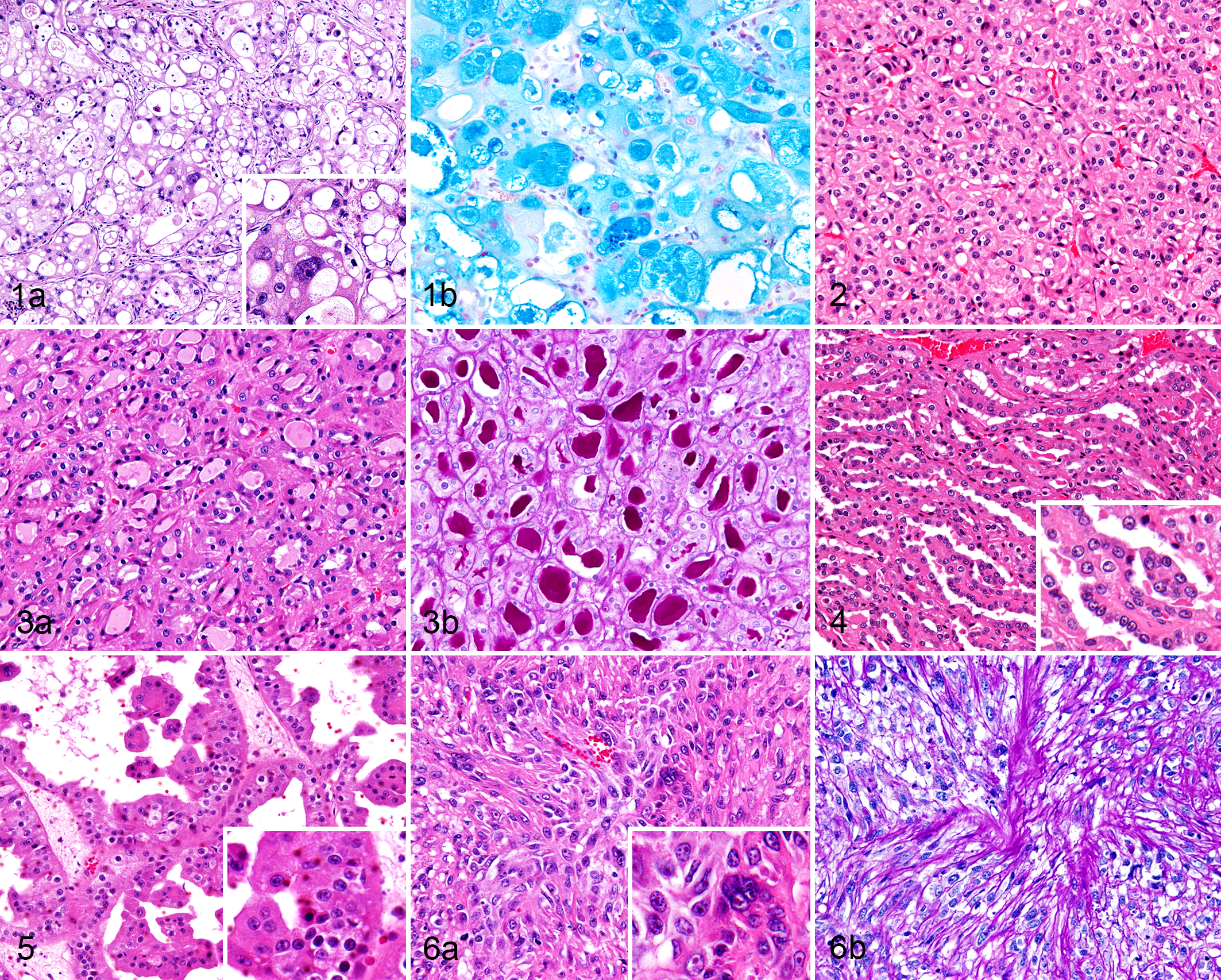
The tubular type (cases 5–7) consisted of tubular structures composed of cuboidal tumor cells separated by basement membrane. The tumor cells had eosinophilic cytoplasm, round to ovoid monomorphic nuclei, and centrally located nucleoli (Fig. 3a). The tubular structures were often filled with PAS-positive eosinophilic material (Fig. 3b).
The papillary type (cases 8 and 9) contained a papillary PAS-positive fibrovascular stroma lined by neoplastic epithelial cells. The papillary lesions had 2 distinct subtypes. Case 8 exhibited papillae covered by a single layer of cuboidal cells and scant cytoplasm, monomorphic nuclei, and small nucleoli (Fig. 4). In contrast, case 9 displayed columnar tumor cells with abundant cytoplasm, prominent nuclear crowding, and pseudostratification (Fig. 5).
The sarcomatoid type (case 12) was characterized by polygonal to spindle-shaped pleomorphic cells with eosinophilic granular spindle-shaped cytoplasm, ovoid to irregularly shaped nuclei, scattered chromatin, and distinct nucleoli (Fig. 6a) often along with abundant PAS-positive extracellular matrix (Fig. 6b). The nuclei of the sarcomatoid type displayed marked nuclear atypia with a high N/C ratio. Metastatic lesions were evident only in the sarcomatoid case at the time of presentation.
The neoplasms in cases 3 and 4, and those encountered in case 10 and 11, were composed of both solid-tubular and tubulopapillary variants.
Of the 12 feline RCC examined in this study, a moderate and high number of mitotic figures were observed in the solid anaplastic type (case 1) and sarcomatoid type (case 12), respectively. A significantly high Ki-67 labeling index (53.5%) was also observed in case 12. In the renal tissue adjacent to the tumor, there were degenerated tubular cells with marked lymphocyte infiltration. Tubular atrophy and congested blood vessels were also noted. A varying degree of sclerotic change was observed in the renal glomeruli. Foci of hemorrhage and necrosis were more commonly found in cases 4, 9, 10, and 12. In case 12, the tumor cells infiltrated the surrounding fibrous capsule and invaded the vessels.
IHC
The IHC results are summarized in Table 3. In the normal renal tissues, the proximal tubules expressed aquaporin-1 (AQP-1; Fig. 7a) and CD10 (Fig. 7b). AQP-1 expression was observed at the apical and lateral cell membranes, while CD10 expression was restricted to the apical cell membrane (the brush border). The distal tubules, collecting ducts, and renal pelvic epithelium expressed KIT (Fig. 7c), cytokeratin (CK) AE1/3, and CK20 (Fig. 7d). CK7 was expressed in the collecting duct and renal pelvic epithelium. Vimentin was expressed in the distal tubules and collecting ducts. CK AE1/3 and vimentin had cytoplasmic expression while KIT and CK 20 showed membranous expression at apical/lateral margins of the epithelial cells.
Immunohistochemical Features of Feline Renal Cell Carcinoma.
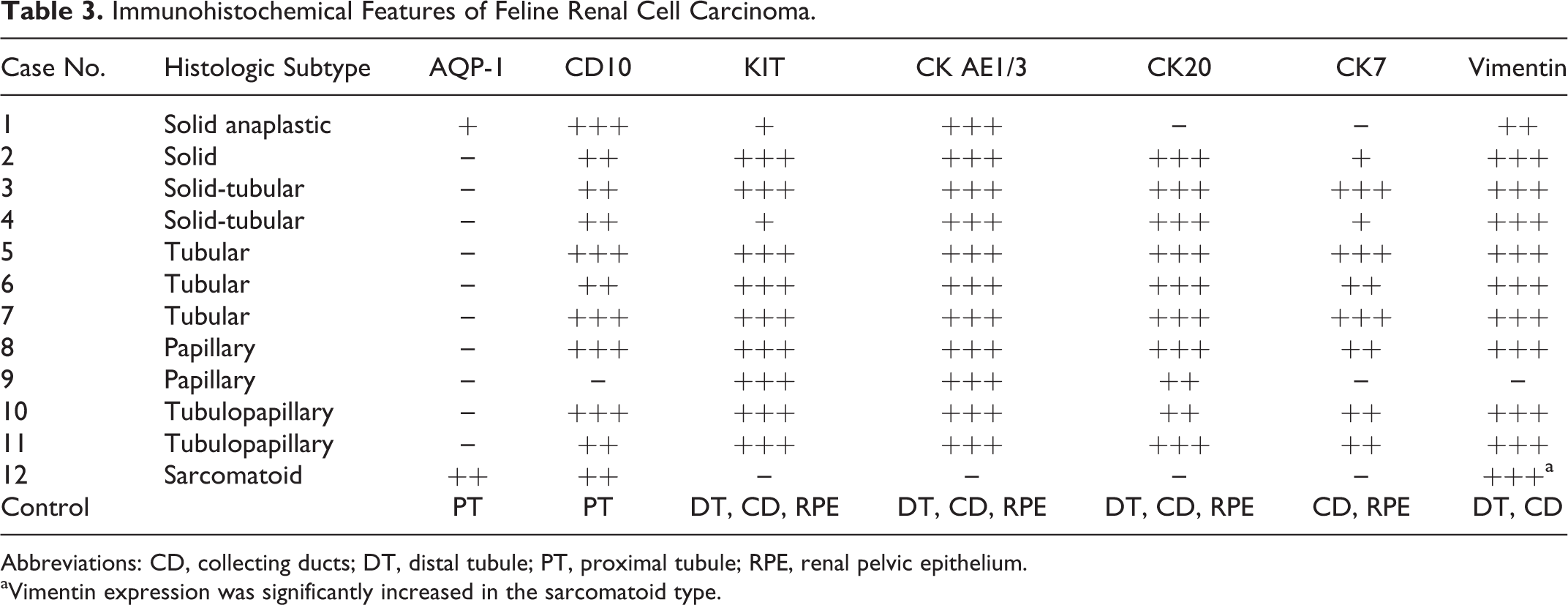
Abbreviations: CD, collecting ducts; DT, distal tubule; PT, proximal tubule; RPE, renal pelvic epithelium.
aVimentin expression was significantly increased in the sarcomatoid type.
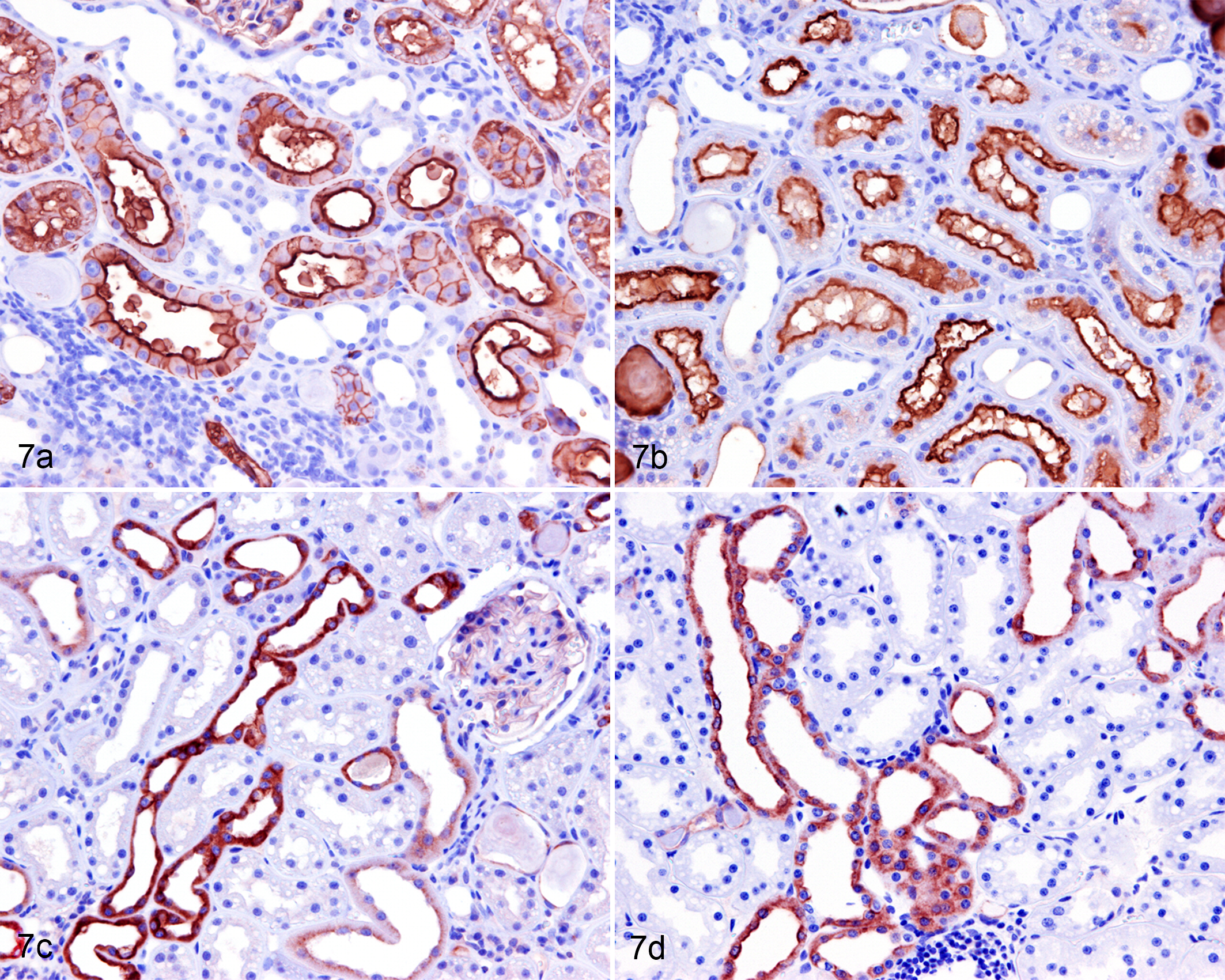
Normal tissue, kidney, cat, case 11. Immunohistochemistry for aquaporin-1 (a), CD10 (b), KIT (c), and cytokeratin (CK) 20 (d). (a) Aquaporin-1 is expressed at the apical and lateral margins, while (b) CD10 is predominantly expressed at the apical cell margins (brush border) of the epithelial cells in the proximal tubules. (c) KIT and (d) CK20 are expressed at the apical/lateral margins of the epithelial cells in the distal tubules and collecting ducts.
The RCC of sarcomatoid type (case 12) had focal cytoplasmic expression of AQP-1. The solid anaplastic RCC (case 1) also had occasional cytoplasmic expression of AQP-1 (Fig. 8). CD10 was positive in all cases except for case 9. CD10 predominantly showed membranous expression. Interestingly, the solid anaplastic type (case 1) showed membranous CD10 expression (Fig. 9), while the other solid type (case 2) had a “dotlike” cytoplasmic expression pattern with intense CD10 reactivity in the tubular components (Fig. 10). All cases had cytoplasmic expression of KIT (Fig. 11) and CK AE1/3 (Fig. 12), except for the sarcomatoid type. KIT was diffusely positive in the neoplastic cells with variable staining intensity while it was focally positive in only one solid type (case 1) and one solid-tubular type (case 4). Similarly, CK20 was positive in the tumor cells of all types (Fig. 13), except for the solid anaplastic and the sarcomatoid types. Most cases had focal to diffuse cytoplasmic CK7 expression (Fig. 14) while the solid anaplastic (case 1), pseudostratified papillary (case 9), and sarcomatoid types lacked CK7 expression. Filamentous cytoplasmic expression of vimentin was observed except for one papillary type (case 9). Interestingly, the staining intensity was different between the sarcomatoid type (case 12) and the remaining types. The sarcomatoid type exhibited strong cytoplasmic expression of vimentin while the remaining types exhibited faint filamentous cytoplasmic expression.
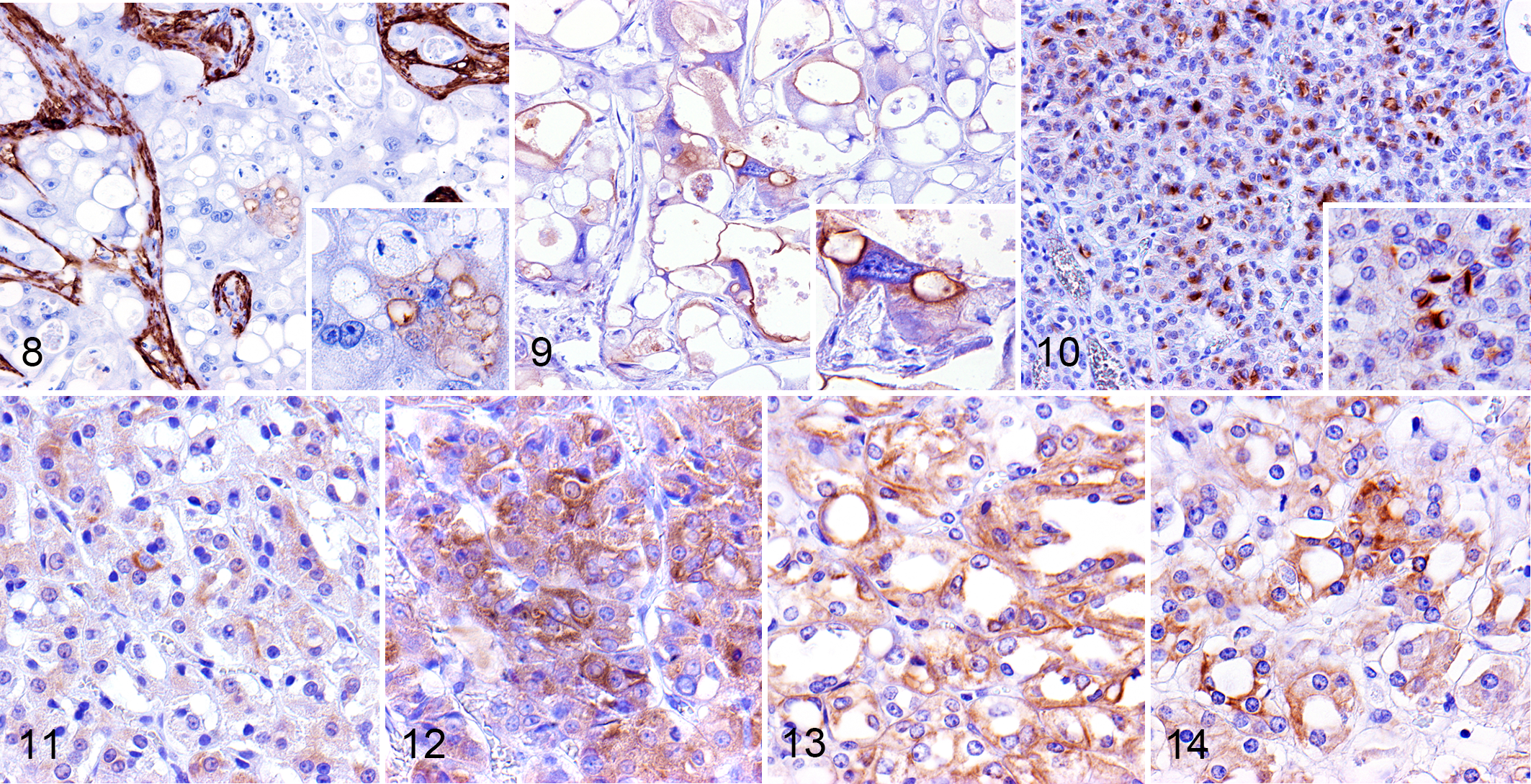
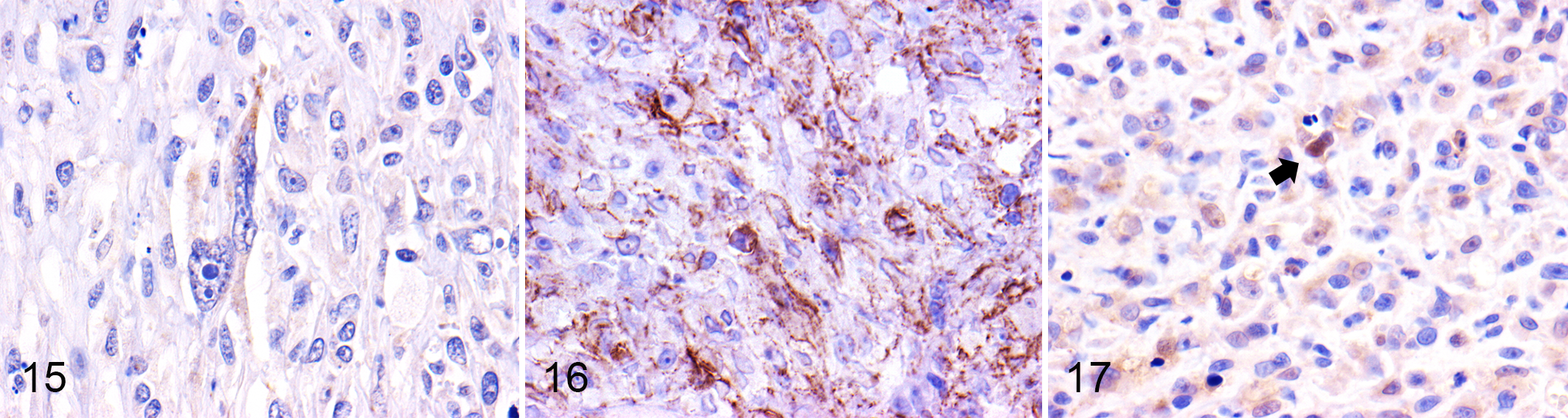
The expression of EMT-related markers was also evaluated (Table 4). Twist was positive in the RCC of sarcomatoid type (Fig. 15) and solid anaplastic type. α-Smooth muscle actin (SMA) was expressed only in the sarcomatoid type. E-cadherin expression was significantly reduced in the sarcomatoid type. Focal cytoplasmic expression of N-cadherin was observed in the=sarcomatoid, solid, and solid-tubular types (Fig. 16). Intranuclear expression of β-catenin was seen in the sarcomatoid type (Fig. 17), while cytoplasmic expression was seen in the other types. Desmin expression was absent in all cases.
Immunohistochemistry for EMT-Related Markers in Feline Renal Cell Carcinoma.
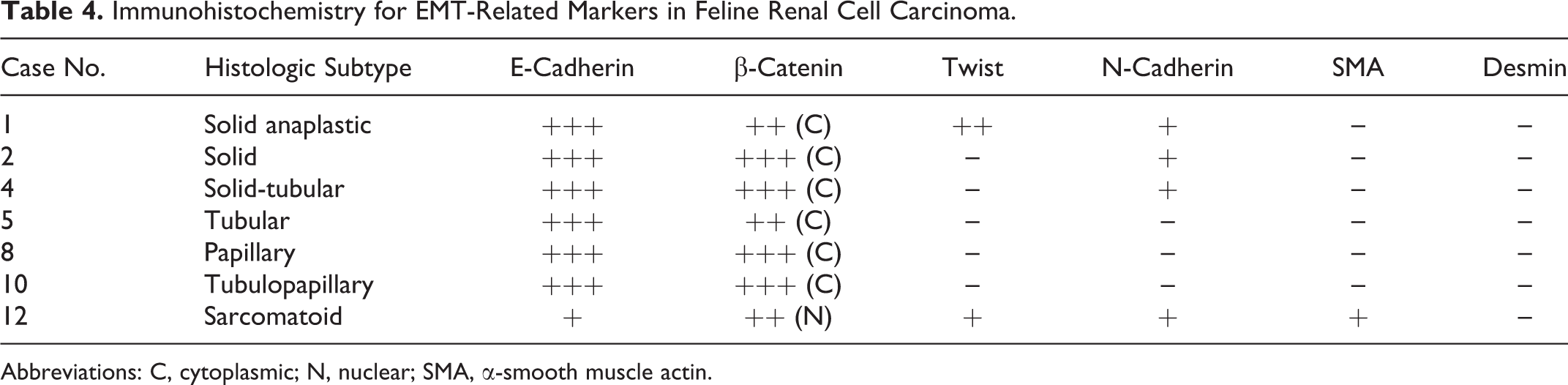
Abbreviations: C, cytoplasmic; N, nuclear; SMA, α-smooth muscle actin.
A double immunofluorescence examination revealed cytoplasmic expression of E-cadherin and N-cadherin co-localizing with Twist in the RCC of sarcomatoid type (case 12; Fig. 18).
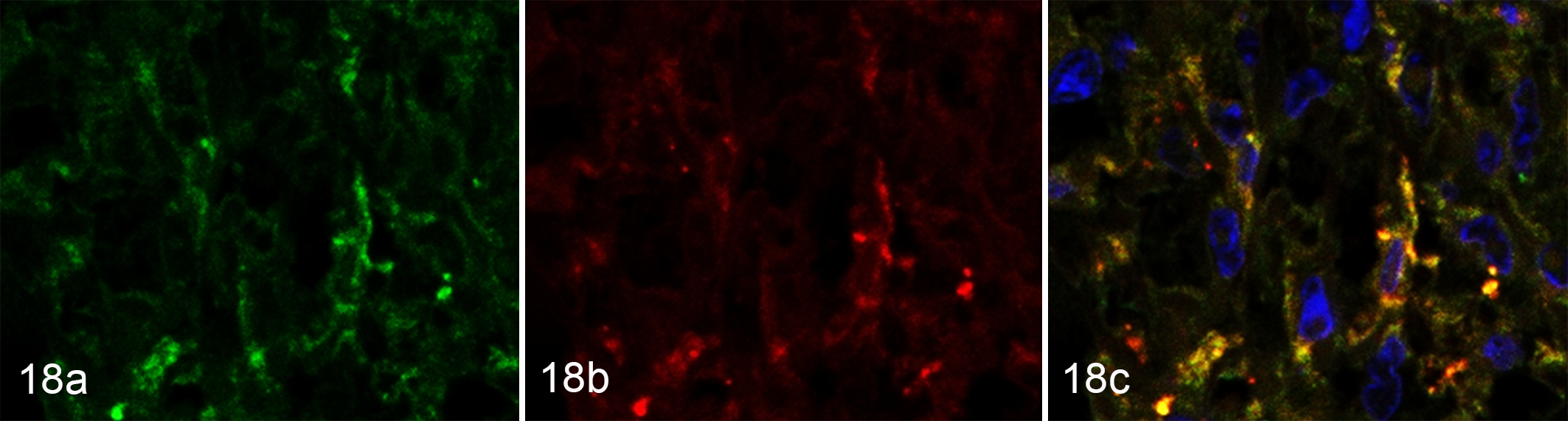
Sarcomatoid renal cell carcinoma, kidney, cat, case 12. (a) Granular cytoplasmic expression of Twist (green) is detected in the tumor cells. (b) Cytoplasmic granular N-cadherin expression (red) is demonstrated in a similar manner. (c) The merged signals (yellow) indicate the colocalization of N-cadherin and Twist. Immunofluorescence.
Survival
Survival data were available in 8 of the 12 cases (Table 1). The animal with sarcomatoid type (case 12) suffered peritonitis, developed a metastatic lesion in the omentum, and died at 4 postoperative weeks. The cat in case 5 died of non–cancer-associated renal failure at 4 postoperative weeks. Autopsies were not conducted in either of the deceased cats. At the time of publication, the survival durations of the cats in cases 2, 3, 4, 7, 10, and 11 were 2260, 80, 2292, 84, 1287, and 97 days, respectively (Table 1). No tumor recurrence has been reported in those cases.
Discussion
All RCC examined in this study occurred unilaterally in the kidney. RCC was observed predominantly in middle-aged or older cats with no sex predisposition. One outlier in the age distribution was the sarcomatoid case, which presented at a younger age. This may indicate a distinct underlying pathogenesis in sarcomatoid RCC. Hypercalcemia is the most common type of paraneoplastic syndrome in human RCC, 37 and there is a case report of RCC with hypercalcemia in a dog. 33 In the present study, hypercalcemia with normal creatinine levels in 6 cases may suggest either hypercalcemia associated with hemoconcentration or paraneoplastic syndrome in feline RCC. Increased hematocrit with high erythropoietin level in 2 cats may suggest inappropriate secondary polycythemia, as previously described in a case report. 29 In a recent publication, a metastatic rate of 11% was reported in canine RCC, and that study also demonstrated the association of the Ki-67 labeling index and clear cell morphology with a significantly reduced median survival time. 13 In the present feline study, of the 12 cases, only the sarcomatoid type produced a metastatic lesion, and this tumor had a markedly high mitotic count and Ki-67 labeling index. The sarcomatoid type had a shorter survival time compared with the other cases. Taken together, these finding suggest aggressive behavior of sarcomatoid RCC in cats, although only 1 case was available in this series. The solid anaplastic type also had increased mitotic activity, but survival data were not available for this case.
The differential diagnosis of feline sarcomatoid RCC includes leiomyosarcoma. 15 In the present case, leiomyosarcoma was considered less likely due to the presence of focal α-SMA expression and the lack of immunoreactivity to desmin.
Tubular tumors with eosinophilic cytoplasm were the most commonly observed type of RCC in this study. As described in a previous study, 22 tubular RCC might be the most common form of RCC in cats. PAS-positive material (Tamm-Horsfall protein casts) in the tubular components may suggest an origin for those tumor cells in the distal tubule or collecting duct. However, proximal and distal tubule markers were uniformly expressed in all types of RCC regardless of Tamm-Horsfall protein cast formation.
The distributions of CK7, CD10, KIT, AQP-1, and vimentin in the normal renal tissue were comparable with those seen in previous human and feline studies with minor variations. 2,6,9,14,28,36,38,42,47 CK20, a marker of urothelial neoplasia, is normally expressed on the surface of the urothelium and is absent in RCC in humans. 5,20,30,49 In contrast, CK20 was expressed in the distal tubules and collecting ducts of cats in the current study.
While clear cell RCC has occasionally been described in rodents and is rare in cattle and dogs, it is the most common type of RCC in humans. 34 Since clear cell RCC is thought to be of proximal tubular origin, it is often positive for proximal tubule markers and negative for distal tubule markers. 41 Although immunohistochemical profiles of the solid anaplastic type (case 1) resembled those of clear cell RCC in humans, the current feline case showed significantly higher atypia. In humans, clear cell RCC usually contains glycogen and lipid. 18 In case 1, the cytoplasm of the tumor cells contained mucin and/or glycogen. Unfortunately, frozen tissue samples were not available for lipid staining. Mucin-producing clear cell RCC is a rare type of tumor and has been reported in humans. 46 The development of clear cell RCC is often associated with von Hippel–Lindau gene (VHL) mutations in humans. 32 The VHL gene is primarily responsible for controlling the cell’s response to oxygen availability. 17,19,24 VHL mutations in feline renal cell tumors have not been previously reported, and sequencing of the gene was not performed in the current study.
Two subtypes of papillary RCC are described in humans. 11 Type 1 tumors exhibit papillary structures covered by a single layer of small, cuboidal cells with small monomorphic nuclei and scant cytoplasm. Type 2 tumors are characterized by a branching fibrous stroma lined by a pseudostratified layer of tumor cells with large pleomorphic nuclei, prominent nucleoli, and abundant eosinophilic cytoplasm. 11 Type 2 papillary RCC is a more aggressive subtype and carries an unfavorable prognosis. 12 In the present study, both types of papillary RCC were identified in cats. However, it was not possible to conclude that type 2 morphology predicts a poor prognosis in cats because no survival data were available for the present feline cases. Because of the consistent expression of proximal tubular markers, human papillary RCC is considered of proximal tubular origin. 45 Human cases of type 2 papillary RCC display a different staining pattern from that of type 1. 45 The expression of CD10 together with KIT and CK20 might indicate that papillary RCC is able to differentiate toward both proximal and distal tubule phenotypes. The lack of CK7 expression in the tumor cells of the type 2 papillary RCC was consistent with the findings of human studies. 31
AQP-1 acts as a water channel and is widely expressed in the membranes of fluid-transporting epithelia, including the proximal tubules of the kidney. In humans, papillary and clear cell RCC that exhibit increased AQP-1 expression have a better prognosis. 23,43 On the other hand, the overexpression of AQP-1 is associated with angiogenesis, tumor spread, and a poor prognosis in sarcomatoid RCC. 48 In the current feline study, the strong interstitial and rare cytoplasmic AQP-1 expression in the solid anaplastic type can be explained by the well-vascularized nature of such lesions, which decreases as the tumor stage progresses. 1,10,39,40
CD10, a marker of the proximal tubule, is sporadically expressed in canine RCC, while KIT, a marker of the distal tubules, is expressed in most cases of canine RCC. 7,16 In contrast, human RCC frequently exhibits CD10 expression but lacks KIT expression. 7 In the present study, CD10 and KIT were shown to be specific to the normal proximal and distal tubules, respectively. However, most cases were positive for both CD10 and KIT. In a previous case study, feline RCC exhibited inconsistent CD10 expression, 3 while in the current study, feline RCC demonstrated reasonably consistent CD10 expression. The intensity of CD10 immunoreactivity was similar to that described by Ramos-Vara et al. 38 Solid type, in particular, showed dotlike inconsistent CD10 expression in the solid components with more intense CD10 expression in the tubular components. This may indicate an increased CD10 expression according to tubular differentiation. Espinosa de los Monteros et al. 14 reported that 50% of feline RCC expressed CK20. However, in the present study, CK20 expression was detected in most cases, except in the solid anaplastic and sarcomatoid types. These findings indicate that feline RCC might display aberrant proximal and distal tubule marker expression, regardless of the origin of the tumor.
EMT has been demonstrated to be an essential process for tumor metastasis, and the development of sarcomatoid RCC represents an example of EMT in humans. 8,21,44 In the present study, the co-localization of E-cadherin and N-cadherin with Twist was detected in the tumor cells of the sarcomatoid type. Decreased E-cadherin expression, increased N-cadherin and Twist expression, and the nuclear accumulation of β-catenin are highly indicative of the involvement of an EMT pathway, as described in human sarcomatoid RCC. 26,27,50,51 EMT is a process that allows epithelial cells to acquire mesenchymal phenotypes via the down-regulated expression of cell adhesion molecules, such as E-cadherin and β-catenin. 26,27 Interestingly, N-cadherin or Twist expression was not specific to the sarcomatoid type but was also present in the solid or solid-tubular types. Twist expression in the solid anaplastic type may be associated with poor prognosis, as described in human clear cell RCC. 25
In conclusion, the present study revealed distinct immunohistochemical features of feline RCC that differ from those of canine or human RCC. Most feline RCC express CK AE1/3, CK7, CK20, CD10, KIT, and vimentin, regardless of their histological subtypes. The tumor cells of the type 2 papillary RCC were negative for CK7, which was consistent with the findings obtained in human cases. These findings warrant further investigation to clarify whether the biological behavior of feline papillary RCC is comparable with that of human RCC. Lastly, EMT might be involved in the development of sarcomatoid RCC in cats. Additional samples and cytogenetic investigations are needed to understand the nature of sarcomatoid RCC in cats.
Supplemental Material
Supplemental Material, DS1_VET_10.1177_0300985818776055 - Histopathologic and Immunohistochemistry Findings in Feline Renal Cell Carcinoma
Supplemental Material, DS1_VET_10.1177_0300985818776055 for Histopathologic and Immunohistochemistry Findings in Feline Renal Cell Carcinoma by Isao Matsumoto, James K. Chambers, Kazumi Nibe, Ryohei Kinoshita, Ryohei Nishimura, Hiroyuki Nakayama, and Kazuyuki Uchida in Veterinary Pathology
Supplemental Material
Supplemental Material, DS2_VET_10.1177_0300985818776055 - Histopathologic and Immunohistochemistry Findings in Feline Renal Cell Carcinoma
Supplemental Material, DS2_VET_10.1177_0300985818776055 for Histopathologic and Immunohistochemistry Findings in Feline Renal Cell Carcinoma by Isao Matsumoto, James K. Chambers, Kazumi Nibe, Ryohei Kinoshita, Ryohei Nishimura, Hiroyuki Nakayama, and Kazuyuki Uchida in Veterinary Pathology
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.