
Abstract
Melanocytic neoplasms are common in dogs and frequently occur within the oral cavity or in haired skin. The behavior of melanocytic neoplasms is variable and depends on tumor location, size, and histopathologic features. This study compared cytopathology and histopathology of 32 lymph nodes from 27 dogs diagnosed with melanocytic neoplasms. Agreement between the original cytology report, cytology slide review, original histopathology report, and histopathology slide review was determined for each lymph node. A subset of lymph nodes was subjected to immunohistochemistry (Melan-A) and additional histochemical stains/techniques (Prussian blue, bleach) to assist in differentiation of melanocytes and melanophages. Agreement ranged from slight to fair for each of the variables evaluated with weighted kappa (κw) or kappa (κ) analysis (original cytology vs cytology review κw = 0.24; original cytology vs original histopathology κw = 0.007; original cytology vs histopathology review κw = 0.23; cytology review vs original histopathology κw = 0.008; cytology review vs histopathology review κw = 0.006; and original histopathology vs histopathology review κ = 0.18). The diagnoses (metastatic, equivocal, or negative for metastasis) of the original report and slide review for both cytology and histopathology were not significantly correlated with survival in this population of patients. Overall, agreement between cytology and histopathology was poor even with a single clinical or anatomic pathologist performing slide review. Consensus between routine cytology and histopathology for staging of lymph nodes in patients with melanocytic neoplasms is poor and does not correlate with survival.
Melanocytic neoplasms are common in dogs and frequently occur within the oral cavity or in haired skin. 3,31 Oral malignant melanoma is the most common tumor in the oral cavity of dogs. 3,33 The behavior of melanoma can be varied, and tumors may act differently based on their location, size, stage, and histopathologic features. 3,31 In general, melanocytic neoplasms in haired skin tend to behave in a more benign fashion, whereas those in the oral cavity more often have an aggressive metastatic course. 3 However, anatomic location alone is not sufficient to predict biologic behavior, as it has been shown that histologically well-differentiated melanomas behave in a benign fashion, even if located within the oral cavity. 8 Despite this, there are reports of patients who have died of their disease despite a histologically well-differentiated, benign-appearing melanocytic tumor. 3,32 Metastasis of melanocytic neoplasms typically occurs to draining local lymph nodes and the lungs. Surgery and radiation therapy are the most often used methods to achieve local control of melanocytic neoplasms, with chemotherapy given to control metastatic disease.
Many cytology reports are equivocal in terms of identifying metastasis of melanoma. Cytologic diagnosis of lymph node metastasis can be challenging due to the varied appearance of metastatic melanocytes and the presence of melanophages (melanin-containing macrophages), which is also the case in humans with melanocytic neoplasms. 15 Histopathology is considered the gold standard for identifying lymph node metastasis, but in many cases, it can remain difficult to differentiate between melanophages and melanocytes. 9,12 Whereas fine needle aspiration remains a mainstay diagnostic technique when evaluating for metastasis to regional lymph nodes in animals, fine needle aspiration is not commonly used to evaluate lymph node status in humans. 1,35 Studies evaluating the use of ultrasound-guided fine needle aspiration of lymph nodes in humans with melanoma have shown conflicting results, with sensitivities for detecting metastasis ranging from 34% to 100%. 1,34,35
Lymphatic pathways, particularly in the canine head, have been shown to be complex with multiple lymphocentra receiving drainage. 2,13,30 Because of this, sampling lymph nodes from a single lymphocentrum potentially overlooks metastatic disease that may be present in lymph nodes from other lymphocentra.
For lymph nodes from dogs with melanoma, the cytology report may be equivocal and recommend histopathologic evaluation of the sampled lymph node. In addition, histopathologic results of removed lymph nodes do not always correlate with cytologic findings or patient prognosis. Based on these experiences, the purpose of this study was to evaluate the correlation between cytology and histopathology for evaluation of regional lymph nodes in dogs with melanocytic neoplasms. A second purpose was to determine if cytologic or histologic diagnosis of lymph node metastasis correlated with survival.
Materials and Methods
Selection of Cases and Review of Records
Medical records from the Auburn University Veterinary Teaching Hospital were searched from 2005 to 2013 for dogs that had a primary melanocytic neoplasm with both cytologic and histopathologic evaluation of the local lymph node. The goal of surgical extirpation was to remove all lymph nodes in the lymphocentrum in their entirety. Dogs were excluded if cytology had not been performed on the lymph node prior to removal or if records of cytology and/or histopathology could not be found. For the original histopathology submission, lymph nodes were evaluated grossly and sectioned based on the individual pathologist’s discretion.
Records were reviewed and data on the following variables were collected: age, sex, breed, clinical signs, primary tumor location, lymph node palpation (enlarged or not; this was subjective based on palpation by the attending clinician), diagnostic imaging for staging, type of surgery for the primary tumor (marginal or wide), histopathology results of the primary tumor (diagnosis, margins, mitotic index), local recurrence, survival time, and cause of death.
Interpretation of Original Cytology Report Prior to Slide Review
A median of 3 smears (range = 1-10) was used to evaluate the lymph node on the original cytology report. The original written cytology reports were assessed by 3 evaluators. The description and final opinion of the original report were evaluated independently by each evaluator, and a final diagnosis of negative for metastasis, positive for metastasis, or equivocal was assessed for each patient. At the time of evaluation, evaluator 1 was a surgery resident (J.A.G.), evaluator 2 was a surgery residency trained clinician (B.M.M.), and evaluator 3 was a board-certified clinical pathologist (P.W.C.).
Slide Review
Cytology slides were reviewed by a clinical pathologist (P.W.C.). Histopathology slides were reviewed by an anatomic pathologist (J.W.K.). Cases were blinded so neither pathologist was aware of the findings of the original report.
Cytology
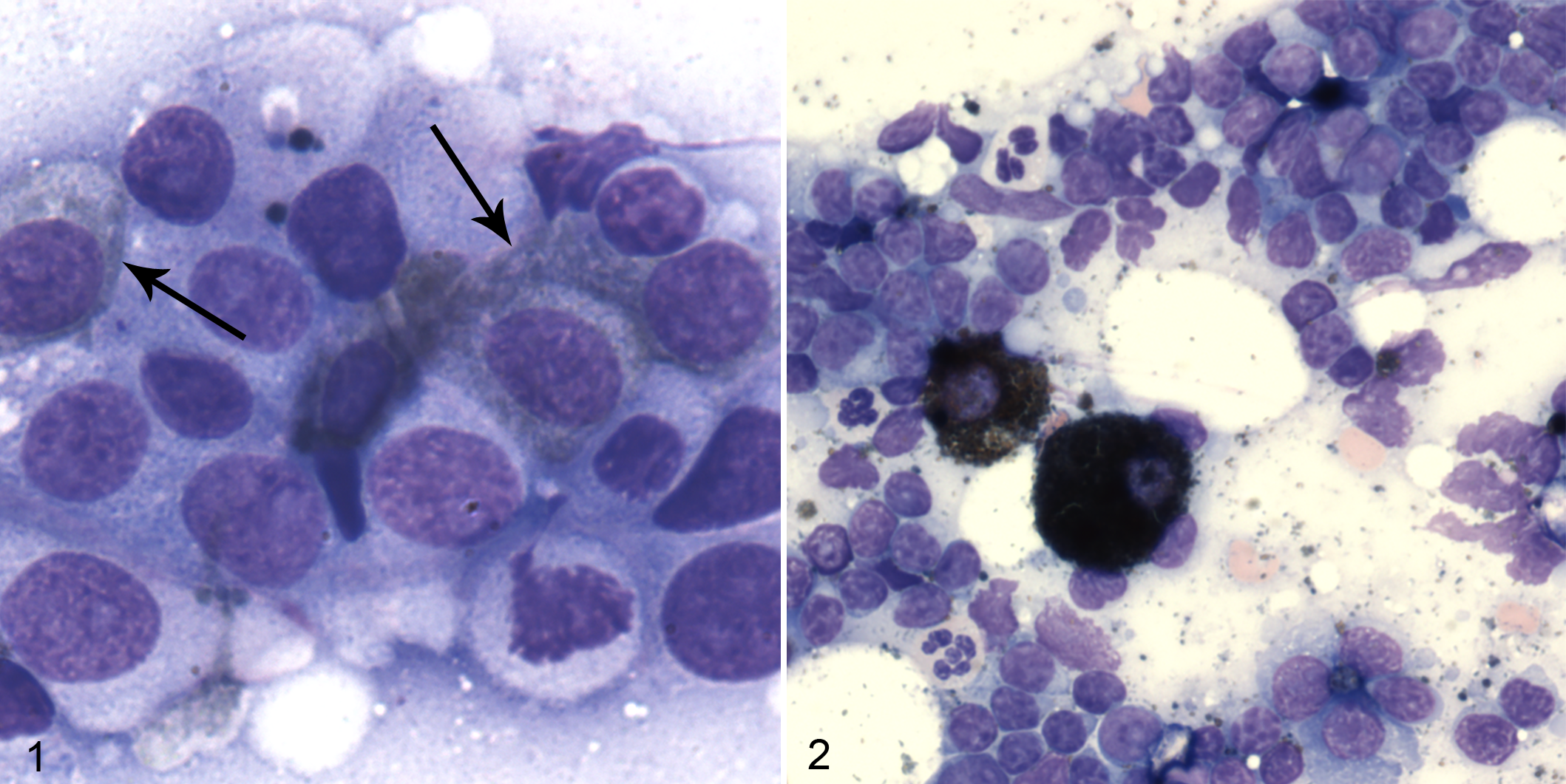
Lymph node aspirate smears were interpreted as nonmetastatic if melanin-containing cells were not identified or were rare (0-5 cells per smear), and no nonpigmented cells exhibiting cohesion, mesenchymal morphology, or features of malignancy were noted. Smears were interpreted as metastatic melanoma if increased numbers (> 5 cells per smear, but actual numbers were often much higher) of melanin-containing cells were identified, and the cells were spindle shaped, exhibited cohesiveness, and/or had distinct features of malignancy (Fig. 1). Smears were judged to be equivocal if there were increased numbers of melanin-containing cells (> 5 cells per smear) that were all individualized and round with no significant features of malignancy, including anisocytosis, anisokaryosis, variation and/or increase in nuclear-cytoplasmic ratio, multinucleation, and increased mitotic activity (Fig. 2).
Histopathology
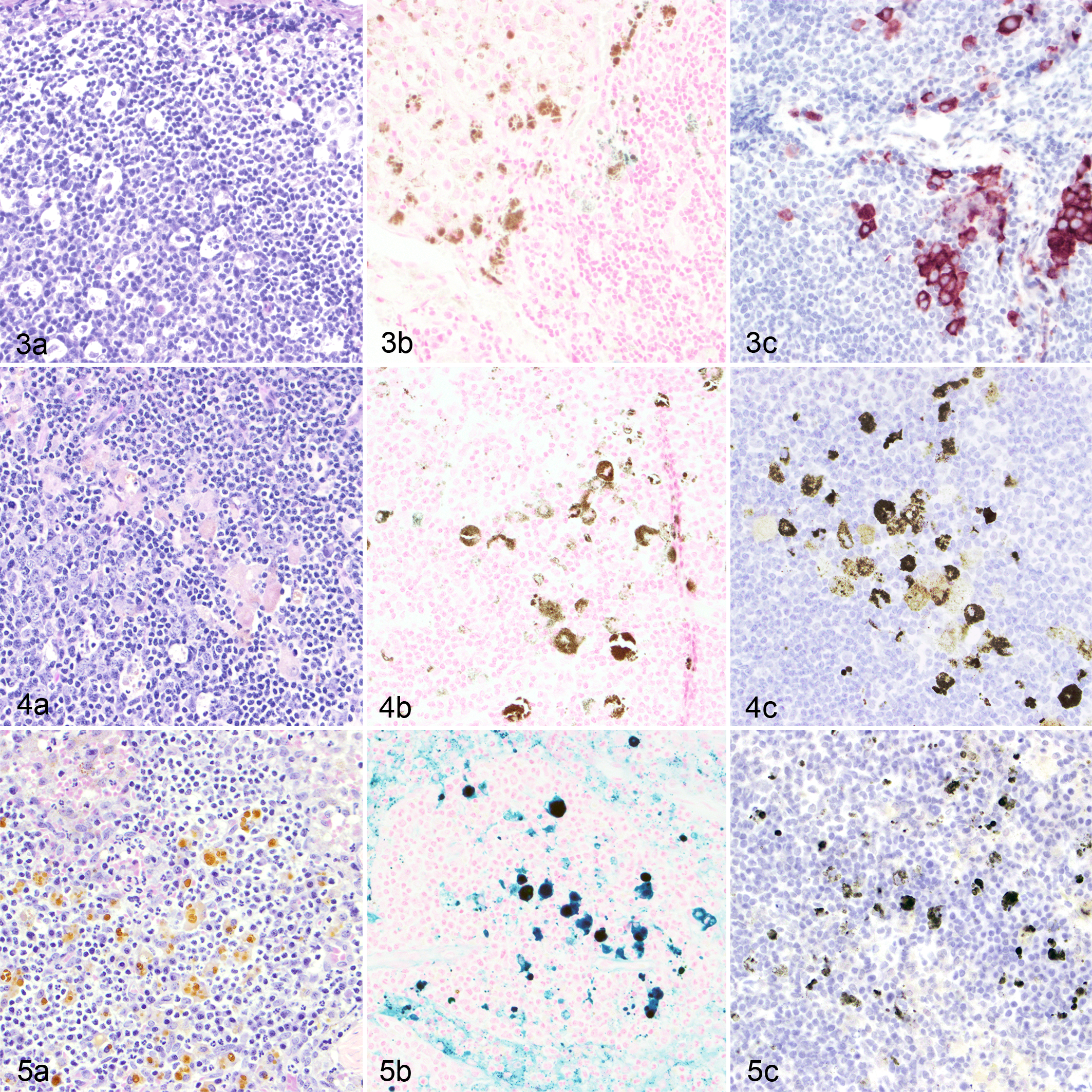
Lymph nodes were evaluated for the presence of (1) cells with morphology consistent with malignant melanocytes and (2) cells of indeterminate origin that contained pigment consistent with melanin (cytoplasmic dark brown to black granular pigment). Nodes were considered to have macrometastasis if neoplastic cells were present in large enough groups to efface or distort the architecture of the node. Sections stained with hematoxylin and eosin were examined first. If aggregates of pigment-containing cells were present, a Prussian blue stained section and a bleached section were examined. If there were pigment-containing cells that did not contain hemosiderin, immunohistochemistry for Melan-A (and in some cases for S100) using a red chromogen (NovaRED) was performed in an effort to further identify these cells (Fig. 3-5). Nodes were considered to have micrometastasis if the sinuses or perisinusoidal parenchyma contained low numbers (5-15) of individualized or clustered cells that had (1) morphology consistent with melanocytes, (2) negative staining for iron, and (3) immunopositivity for Melan-A.
Statistical Analysis
Agreement between reviewer interpretation of the original cytology report was measured using Fleiss kappa. Weighted kappa was used to compare cytology to histopathology for each of the following scenarios: original cytology report interpretation (always by evaluator 3) to cytology slide review results, original cytology report interpretation to original histopathology report, original cytology report interpretation to histopathology slide review results, cytology slide review results to original histopathology report, and cytology slide review results to histopathology slide review results. An imputed relative distance of 1 was assigned to the difference between equivocal and negative or metastatic results (thus, equivocal/negative or equivocal/metastatic disagreement was not graded as harshly as a negative/metastatic disagreement). Kappa analysis was used to compare the original histopathology report to the histopathology slide review results. Interpretation of the kappa statistics was performed based on previously reported strengths of agreement. 16 Kaplan–Meier survival analysis with log-rank test was performed to evaluate results of the original cytology report, cytology slide review, original histopathology report, and histopathology slide review for significance to survival. When dogs with multiple lymph nodes removed were evaluated, only their most aggressive factors were analyzed (eg, if 1 lymph node was enlarged and the other was of normal size, the enlarged lymph node was used for analysis). Fisher exact test was performed to compare the type of surgery (wide vs marginal) and margins (clean or dirty) to local recurrence.
Results
Thirty-two lymph nodes previously collected from 27 dogs were evaluated retrospectively. Four dogs had lymph nodes removed bilaterally for the same primary tumor (all oral in location), and 1 dog had 2 lymphadenectomies for 2 different primary melanocytic neoplasms (both cutaneous in different areas). Mean (SD) age at time of presentation was 10.3 (2.7) years. There were 14 female spayed, 3 male intact, and 10 male castrated dogs. Dogs represented numerous breeds, with 8 mixed breed, 3 each of Labrador Retriever and Golden Retriever, 2 Miniature Schnauzers, and 1 each of Beagle, Cocker Spaniel, Gordon Setter, Havanese, Kerry Blue Terrier, Lhasa Apso, Norfolk Terrier, Rottweiler, Scottish Terrier, Siberian Husky, and Yorkshire Terrier.
Seven dogs had a single cutaneous tumor, 1 dog had 2 cutaneous tumors in different locations, and 19 dogs had oral tumors. Of the cutaneous tumors, 3 were digital, 2 were associated with the metacarpal/tarsal pad, 2 were on haired skin not associated with a digit, 1 was associated with a digital pad, and 1 was ungual in location. For oral tumors, 3 were lingual, 7 were maxillary (4 left caudal maxilla, 3 right caudal maxilla), 5 were mandibular (1 left rostral, 1 left middle, 2 right rostral, and 1 bilateral rostral), and 4 were associated with the lip. Twenty-three patients were diagnosed with a malignant melanoma on histopathology and 4 were diagnosed with melanoma (2 cutaneous, 2 oral), with no information given as to malignant or benign appearance.
Lymph Node Palpation
Information on lymph node palpation was available for 29 lymph nodes, and results of lymph node palpation (normal size or enlarged) were compared to the results of cytology and histopathology slide review (Table 1). Compared to histopathologic evaluation, lymph node palpation had a sensitivity of 67%, specificity of 50%, positive predictive value of 27%, and negative predictive value of 85%.
Relationship Between Palpation of Lymph Nodes (Normal or Enlarged) and Review of Cytology and Histopathology Slides for 29 Lymph Nodes From 27 Dogs With Melanocytic Neoplasms.
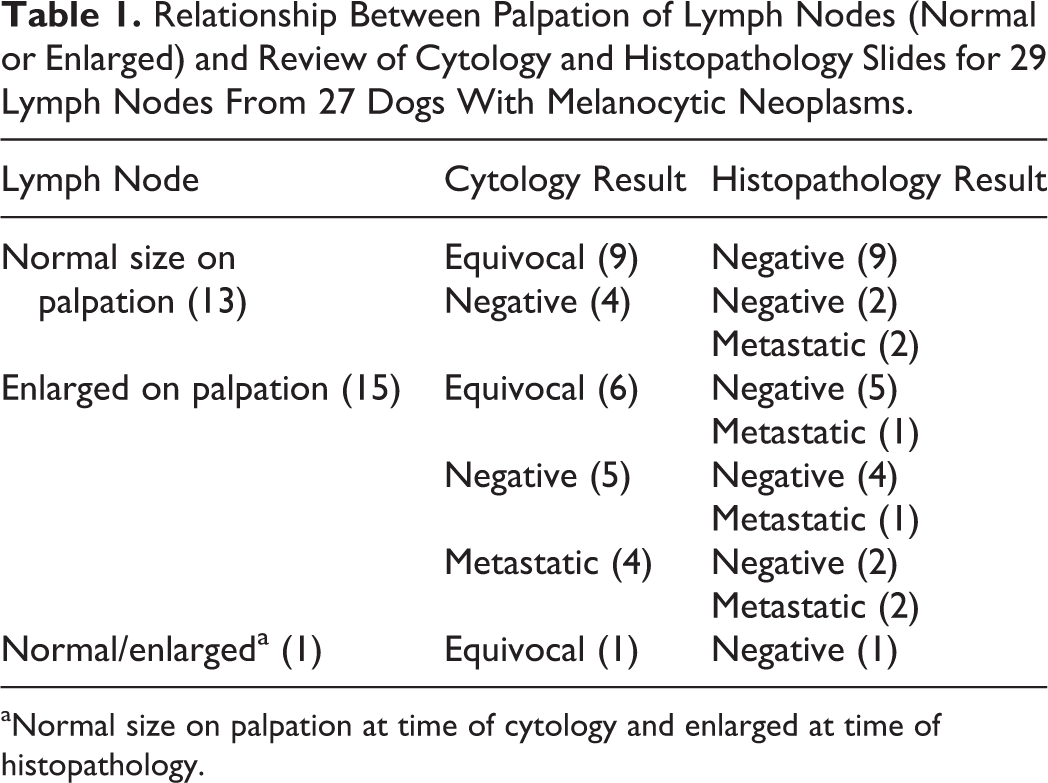
aNormal size on palpation at time of cytology and enlarged at time of histopathology.
Thoracic Radiographs
Thoracic radiographs were available from 26 of the 27 dogs. In 2 dogs (8%), thoracic radiographs were strongly suspicious for metastatic disease. In 1 of these dogs, the lymph node was negative on the original cytology report, cytology slide review, original histopathology report, and histopathology slide review. For the other dog, the original cytology report was equivocal, cytology slide review indicated metastasis, the original histopathology report indicated metastasis, and the histopathology slide review did not identify metastasis.
Local Treatment of the Primary Tumor
Of the 27 dogs, 22 (81%) dogs had surgery alone for their primary mass, 4 (15%) had surgery and radiation therapy, and 1 (4%) had radiation therapy as the primary treatment. A wide excision was performed for 15 tumors and a marginal excision was performed for 13 tumors. Local recurrence of the primary tumor occurred in 9 of 13 dogs with marginal excision (69% of all marginal excisions) and 5 of 14 (36%) cases with wide excision and information on local recurrence. Of the 5 cases that underwent wide excision and had recurrence, 3 (60%) had clean margins on histopathology. Local recurrence of the primary tumor occurred in 7 of 10 (70%) tumors with dirty margins on histopathology and in 4 of 14 tumors (29%) with clean margins on histopathology. In all 4 cases that did not have margins reported, the tumor recurred and all of these patients had previously undergone a marginal excision of their primary tumor. Achieving clean margins was not significant for local recurrence (P = .066), nor was marginal versus wide surgical excision (P = .082).
Interpretation of Original Cytology Report Prior to Slide Review
Based on their review of the cytology report, all 3 evaluators agreed with each other on the diagnosis for 19 of the 32 lymph nodes (59%). Nine of these 19 lymph nodes were interpreted as equivocal, 2 as metastatic, and 8 as negative for metastasis. All disagreements were between a negative and equivocal result. Agreement between reviewers was moderate on Fleiss kappa statistical analysis (κ = 0.51). Perfect agreement was reached for all cases designated as metastatic (κ = 1), with moderate agreement for a negative interpretation (κ = 0.45) and an equivocal interpretation (κ = 0.46).
Interpretation of Cytology After Slide Review
After slide review, evaluator 3 agreed with the original interpretation of the report for 16 of 32 (50%) lymph nodes. Ten cases that evaluator 3 originally considered negative (based only on review of the original cytology report) were changed to equivocal after slide review. Of the 6 cases originally considered equivocal by evaluator 3, 4 were changed to negative and 2 were changed to metastatic. All cases that were initially considered metastatic remained metastatic after review. There was fair agreement between evaluator 3’s interpretation of the original cytology report and the subsequent slide review by evaluator 3 on weighted kappa analysis (κ = 0.24).
Histopathology Slide Review
On the original histopathology report, 20 cases (63%) were considered metastatic and 12 (38%) negative for metastasis. For 15 cases (47%), the lymph node diagnosis was changed based on slide review. Fourteen of these were considered metastatic based on the original report but were diagnosed as negative for metastasis after slide review based on systematic application of iron stain and bleach followed by Melan-A, along with the aforementioned criteria for diagnosis of metastasis. One case that was originally interpreted as negative was changed to metastatic. There was fair agreement (κ = 0.18) between the original histopathology report and the histopathology slide review results.
Comparison of Cytology and Histopathology
Weighted kappa analysis for comparison of the original and slide review cytology reports to the original and slide review histopathology results showed fair to slight agreement among all categories evaluated (Table 2).
Weighted Kappa Statistic for Comparison of Original and Slide Review Cytology Reports to the Original and Slide Review Histopathology Results.a
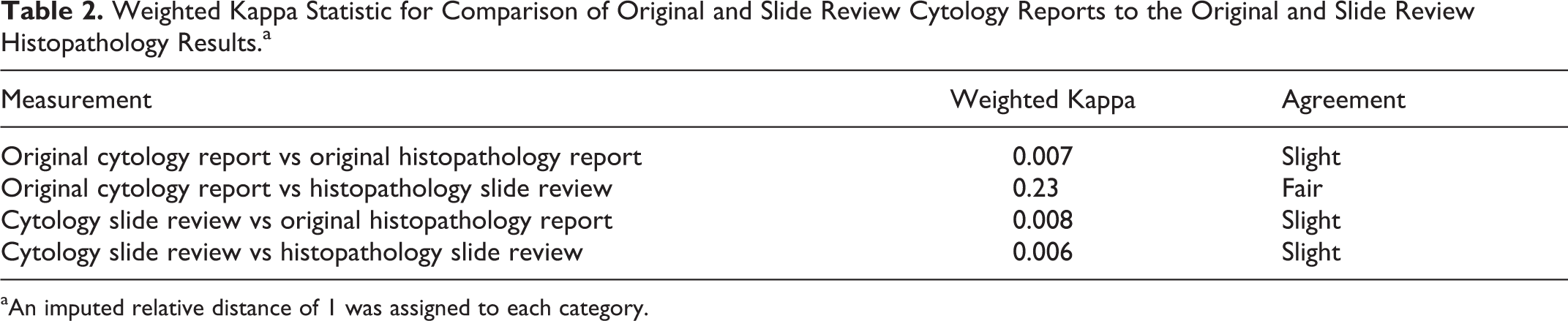
aAn imputed relative distance of 1 was assigned to each category.
Survival
At the end of the study, 22 dogs were confirmed to be dead, 4 confirmed alive, and 1 lost to follow-up. The overall median survival time (MST) was 539 days. The cause of death was related to progression of disease in 13 of 27 patients (59%), was unrelated to the tumor in 2 cases (9%), and was unknown in 7 cases (32%). Both patients with radiographic evidence of suspected lung metastasis died—1 died of their disease at 41 days and the other of unknown causes at 81 days following presentation. Neither the original cytology report, cytology review, original histopathology report, nor histopathology review were significantly correlated with survival in this population of dogs (Table 3).
Kaplan–Meier Survival Analysis for Comparison of Results From Each Report Category.

Abbreviation: MST, median survival time in days; NA, not applicable.
Discussion
The objective of this study was to evaluate the correlation between routine cytology and histopathology for assessment of regional lymph node metastasis of melanocytic neoplasms. Agreement was fair to slight among all categories tested, indicating that correlation between cytology and histopathology is low, even after slide review by a single clinical or anatomic pathologist. There was a change in the final diagnosis for 46.9% of cases after histopathology slide review, indicating that interobserver variability is high. Reclassification was performed based on uniform criteria for diagnosis of metastasis by a single pathologist. Macrometastasis was defined as neoplastic cells present in large enough groups to efface or distort the architecture of the node. Micrometastasis was defined as low numbers of individualized/clustered cells with melanocyte morphology, and when present, additional sections were subjected to iron stain, Melan-A immunohistochemistry, and bleaching for further examination. If pigment-containing cells did not contain hemosiderin and had immunopositivity for Melan-A, micrometastasis was diagnosed. Immunohistochemistry may not have been routinely performed prior to slide review, and cells interpreted as metastatic melanocytes on the original histopathology report may have been hemosiderin- or melanin-laden macrophages, resulting in a change in diagnosis when immunohistochemistry was used.
Neither the original cytology or histopathology report nor the cytology or histopathology slide review results were significantly correlated with survival time. Although not statistically significant, it is interesting to note that patients diagnosed with lymph node metastasis survived longer (MST = 669 days) than patients without metastasis (MST = 422 days) based on results of the original histopathology report. After histopathology slide review, patients with negative lymph nodes survived longer (MST = 539 days) than those with lymph node metastasis (MST = 344 days), although this difference was not statistically significant. Dogs that had an original histopathologic diagnosis of lymph node metastasis may have been treated more aggressively with additional modalities than dogs with negative lymph nodes, which may explain these findings.
One patient in this study with lung metastasis from an oral melanoma had a negative mandibular lymph node on original cytology, slide review cytology, original histopathology, and slide review histopathology. Metastasis is generally thought to occur to the local draining lymph node prior to advancing further to the lungs, but it is possible that this patient’s tumor drained to a different lymphocentrum than was sampled. Lymph pathways in the head are complex, with ipsilateral and contralateral flow to various node basins. 2,13,30 The 2 dogs in this population with suspected lung metastasis had survival times of 41 and 81 days, respectively. Although there were too few cases for statistical analysis, this is shorter than the overall MST of 539 days for the entire population of dogs.
It is possible that lymph node status is not as important to disease progression in dogs as may be thought. In human medicine, lymph node status is an important prognostic indicator in melanocytic neoplasms. 19 In the current study, it is more likely either that metastatic disease was present in an area of the lymph node that was not evaluated or that metastasis occurred through a lymphatic pathway that led to a different lymphocentrum than was sampled. A major difference in the evaluation of lymph node metastasis in human and veterinary medicine is that a significantly higher number of sections are evaluated histopathologically in human melanoma patients as compared to veterinary patients. 21,28 This is largely related to cost constraints in veterinary medicine, which also influence the use of immunohistochemical markers. It is possible that metastatic disease was missed based on how the lymph nodes in this study were sectioned. This was a retrospective study, and sectioning methods were not controlled.
The diagnosis of melanocytic metastatic disease in lymph nodes is difficult due to the presence of melanophages, which can complicate cytologic and histopathologic evaluation of the lymph node. Melanophages are macrophages that have taken up melanin granules released into the dermis via a process called pigmentary incontinence. These melanophages then carry the melanin granules to the draining lymph node for removal. This process can occur in normal dogs but is marked in dogs with inflammation. 14 Animals with melanocytic neoplasms are also subject to pigmentary incontinence from the tumor and inflammation associated with the tumor. 18 It can be difficult to distinguish melanophages from tumor cells on cytology and histopathology, and special stains may be required to assist in differentiation on histopathology. This only adds to the difficulty in accurately diagnosing lymph node metastasis in animals with melanocytic neoplasms.
The use of special stains and immunohistochemistry may assist in the diagnosis of melanocytic neoplasms and/or metastasis of these neoplasms. Use of cytology and immunocytochemistry for diagnosis of canine amelanotic melanomas was found to have 66.7% accuracy with cytology and 100% accuracy with immunocytochemistry, compared to histopathology and immunohistochemistry in 1 study that evaluated Melan-A, vimentin, and cytokeratin for both the primary tumor and lymph nodes. 22 The number of lymph nodes evaluated in that study was small (n = 6) and 3 tumors thought to be amelanotic melanoma on cytology were reclassified as sarcoma (n = 2) and carcinoma (n = 1) with use of immunocytochemistry. Use of immunocytochemistry may assist in the cytologic diagnosis of metastasis of melanocytic neoplasms when poorly differentiated neoplastic cells are present, although immunocytochemistry can be difficult to perform. 22
Immunohistochemistry may be used to assist in the diagnosis of metastasis of melanocytic neoplasms, with these tumors generally showing immunoreactivity for 1 or more of S100, Melan-A, PNL2, and tyrosinase as well as immunoreactivity for vimentin antigen and a lack of immunoreactivity for cytokeratins. 10,22 –24 There have been no published studies demonstrating a lack of reactivity for melanin-associated antigens in melanophages in dogs and cats. One study in human medicine found that S100 reliably stained melanocytes and HAM-56 reliably stained melanophages in formalin-fixed paraffin-embedded tissues, but this has not been evaluated in companion animals. 9 Another group evaluated the ability of numerous immunohistochemical markers to differentiate melanocytes and melanophages in pigs, which are a model for human melanoma. 11 This group found that use of Melan-A, PNL2, and ionized calcium binding adaptor molecule 1 (Iba1) was useful to distinguish melanocytes from melanophages, with Melan-A and PNL2 identifying melanocytes, and Iba1 identifying melanophages in pigs. Regardless of which immunohistochemical marker is used, the presence of large amounts of pigment in a cell can make interpretation difficult by obscuring areas in which there is bound chromogen, although bleaching can improve visibility.
Melanocytic neoplasia is not the only canine cancer with poor correlation between cytology and histopathology. One study evaluated the use of cytology compared to histopathology as a gold standard for neoplastic and nonneoplastic lesions and found that cytology correlated with histopathology in only 33% to 66% of cases, depending on location, with false-negative results being more likely than false-positive results. 6 Complete agreement between cytology and histopathology was present in 32%, with partial agreement in another 32% when only neoplastic lesions were evaluated. 6 This study had a low number of lymph nodes evaluated, but only 5 of 10 (50%) had agreement between cytology and histopathology. 6 In addition to the difficulty correlating cytology and histopathology, interobserver variation among pathologists interpreting the same histopathology samples has been shown to occur in a variety of tumors. 20,25,26 The ultimate interpretation changed partially (change in grade, tumor subtype, or margin evaluation) in 20% to 29% of cases or completely (change in cell of origin or degree of malignancy) in 10% to 19% of cases with the use of second opinion histopathology for dog and cat neoplasms. 25,26 In 17% to 37% of these cases, the patient’s treatment and/or prognosis was affected. 25,26 In cases of canine cutaneous mast cell tumors, 1 study had 10 pathologists evaluate the same 60 tumors and found significant variation in tumor grading, although at least 5 pathologists agreed on a grade for all 60 tumors. 20 Given the difficulty in diagnosing metastasis of melanocytic neoplasms in general, it is likely that interpathologist variation also plays a significant role in variability of interpretation. Within the current study, interpretation of the clinical pathology report led to a difference of opinion on the final diagnosis in 37.1% of cases, and agreement was moderate with kappa analysis. Two of the evaluators in this study were not pathologists; however, this is likely more clinically relevant because in many cases, a nonpathologist interprets the report to determine if lymph node extirpation is warranted. Based on the results of this study, different treatment recommendations might have been made in almost one-third of cases due to a difference in interpretation.
A previous study of 100 dogs with oral malignant melanoma found that 70% of cases with lymphadenomegaly had metastatic disease and 40% of cases without lymphadenomegaly had metastatic disease. 36 Based on these findings, it was recommended that cytology of the draining local lymph node should be performed regardless of lymph node size. In the current study, there was a low sensitivity, specificity, positive predictive value, and negative predictive value for lymph node palpation compared to histopathology. In the population of dogs reported here, the lymph node was not measured but was determined to be enlarged based on subjective palpation by the attending clinician. Although subjective, lymph node measurements indicating enlargement have not been reported, and given the varied size of the patients in this study, a single cutoff value would likely be of no benefit. In addition, these methods are in keeping with previous reports on lymph node evaluation for melanocytic neoplasia. 4,36
Lymph nodes can be enlarged for reasons unrelated to tumor metastasis, and these conditions have been previously reviewed. 7 Hyperplastic lymph nodes often show expansion of the lymphocyte population, formation of secondary lymphoid follicles, and increased numbers of plasma cells in medullary cords. These nodes are believed to be responding to antigenic stimulation and have also been termed reactive lymph nodes. Sinus histiocytosis can also be seen in lymph nodes draining an inflamed or hemorrhagic area. In these cases, lymph node sinuses are filled with edema, foamy and/or erythrophagocytic macrophages, inflammatory cells, hemorrhage, and debris. Either condition alone can lead to enlarged lymph nodes on palpation, but lymphoid hyperplasia and sinus histiocytosis are not mutually exclusive and can occur concomitantly. Because most melanocytic neoplasms are in the oral cavity, the draining lymph nodes may be reacting to inflammation caused by tumor necrosis, ulceration, and/or hemorrhage, thus explaining the reason that lymph node palpation is not a sensitive or specific indicator of metastatic disease in these cases. A previous study of oral malignant melanomas in dogs found a similar low sensitivity and specificity for lymph node palpation comparable to our results. 4 Based on these findings, the authors recommended routine lymph node extirpation for histopathologic evaluation in dogs with oral malignant melanoma. 4 The authors also recommended bilateral lymphadenectomy due to a reported risk of contralateral lymph node metastasis in humans. 4
Contralateral lymph node metastasis has also been shown in dogs with tumors of the head. 29 In the current study, 4 patients with oral tumors had bilateral lymphadenectomy of the mandibular lymph nodes and histopathology was negative for metastasis in all lymph nodes (on the original report and subsequent slide review). It has been shown that the locally palpable node is not always the draining node basin. 5,37 In human medicine, sentinel lymph node biopsy is also frequently used to guide lymphadenectomy. 17,19,27 With sentinel lymph node biopsy, the first lymph node receiving drainage from the tumor is identified with the use of lymphoscintigraphy and dye techniques. 19 This lymph node is evaluated for metastasis, and if found, the remainder of the lymph nodes in the region are removed. 17,27 If no metastasis is found, no further lymph node dissection is performed. 17,27 In humans, tumor management based on sentinel lymph node biopsy prolongs disease-free survival and melanoma-specific survival for patients with nodal metastasis from intermediate-thickness melanomas. 19 Rarely, human patients with negative sentinel lymph nodes on histopathology develop regional and distant metastasis, and “stealth” melanoma cells are the suspected culprits of this phenomenon. 15 These are melanoma cells that are difficult to detect since they are single and do not cluster but are still capable of metastasis. 15 This phenomenon may also occur in veterinary patients, where detection of micrometastasis can be difficult. Studies evaluating sentinel lymph node biopsy-based management in dogs with melanocytic neoplasms are needed to determine what role sentinel lymph node evaluation plays in improving the accuracy of lymph node evaluation in these patients.
The major limitations of the current study relate to its retrospective nature. There was significant variation in treatment of these patients, and lymph node sectioning was not standardized. In addition, there may have been a bias for surgical extirpation of lymph nodes that were thought to be more likely to contain metastatic disease. However, 15 cases that were originally considered negative on cytologic analysis by evaluator 3 had surgical extirpation of their lymph nodes, and the reasoning for the recommendation for surgical removal was unclear in these cases. These findings show that there is no gold standard for diagnosis of lymph node metastasis, as there was a change in diagnosis in 46.9% of dogs in this population upon second opinion histopathology review. This study documents inconsistencies in diagnosing lymph node metastasis for canine melanocytic neoplasia.
This study highlights that interpretation of cytology and histopathology of lymph nodes in dogs with melanocytic neoplasms is highly variable. Results do not always correlate with survival. Improved techniques are necessary to better estimate the true presence of lymph node metastasis, such as immunocytochemistry or immunohistochemistry. More defined criteria are necessary to assist in the diagnosis of lymph node metastasis in order to decrease interobserver variation. Routine sampling of mandibular lymph nodes may not provide a true picture of lymph node metastasis for oral melanocytic neoplasms, as lymphatic drainage within the canine head is complex with multiple lymphocentra receiving lymphatic drainage. 2,13,30 It has been previously shown that the mandibular lymph node can have no evidence of metastasis, even when other head lymphocentra have metastatic disease. 13 Sentinel lymph node evaluation may be a more accurate predictor of metastatic status by showing the direct drainage pathway within a particular patient to allow targeting of a specific lymph node. Further research should be done to investigate ways to improve diagnosis of metastasis to lymph nodes for canine melanocytic neoplasms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.