
Abstract
Veterinary pathologists commonly encounter lesions of blunt trauma. The development of lesions is affected by the object’s mass, velocity, size, shape, and angle of impact and by the plasticity and mobility of the impacted organ. Scrape, impact, and pattern abrasions cause localized epidermal loss and sometimes broken hairs and implanted foreign material. Contusions are best identified after reflecting the skin, and must be differentiated from coagulopathies and livor mortis. Lacerations—traumatic tissue tears—may have irregular margins, bridging by more resilient tissue, deviation of the wound tail, crushed hairs, and unilateral abrasion. Hanging or choking can cause circumferential cervical abrasions, contusions and rupture of hairs, hyoid bone fractures, and congestion of the head. Other special forms of blunt trauma include fractured nails, pressure sores, and dog bites. Ocular blunt trauma causes extraocular and intraocular hemorrhages, proptosis, or retinal detachment. The thoracic viscera are relatively protected from blunt trauma but may develop hemorrhages in intercostal muscles, rib fractures, pulmonary or cardiac contusions or lacerations with subsequent hemothorax, pneumothorax, or cardiac arrhythmia. The abdominal wall is resilient and moveable, yet the liver and spleen are susceptible to traumatic laceration or rupture. Whereas extravasation of blood can occur after death, evidence of vital injury includes leukocyte infiltration, erythrophagocytosis, hemosiderin, reparative lesions of fibroblast proliferation, myocyte regeneration in muscle, and callus formation in bone. Understanding these processes aids in the diagnosis of blunt force trauma including estimation of the age of resulting injuries.
Keywords
Pathogenesis of Blunt Force Trauma
The body surface of mammals is built to resist a wide variety of continuous and discontinuous forces, ranging from contact with surfaces while walking and resting to the sudden predicted and unpredicted impact of the body against animate and inanimate objects during voluntary movements. In most instances, the structure of the skin sustains the stress induced by such contact; however, under many circumstances, the energy of the impact can exceed the resistance and compliance of tissues, thus producing visible damage. The latter represents a wound, an entity defined as the damage to any part of the body due to application of mechanical force. 39 The definition of blunt trauma appears an easy task only when looked upon superficially. Blunt trauma is defined as the result of the impact of a body against a blunt surface, the impact of an object with a blunt surface against a body, or a combination of both. 50 Basic concepts of physics, namely, biomechanics, are crucial to understand the pathogenesis of tissue damage and to categorize the observed lesions. Differentiation between blunt and sharp force trauma may be difficult, and a gray area may exist, represented by lesions produced by objects particularly acuminated but not sharp: for these instances, terms such as penetrating blunt trauma or puncture wound have been introduced. 25,39 A clear demarcation between blunt and sharp force trauma may not exist in some circumstances, but for convention, we apply the term blunt force trauma to all lesions caused by clearly nonsharp objects.
The impact between an animal’s body surface and different types of blunt objects occurs frequently during its life and in most circumstances does not lead to tissue damage. A wound develops when the intensity of the applied force exceeds the capability of the tissue to adapt. 39 This concept, however, needs to be applied with caution, since particular types of chronic mechanical injury certainly involve a degree of adaptation of the tissues (eg, pressure sores or chronic constrictions of extremities).
The severity, extent, and appearance of blunt trauma injuries depend on (1) the amount of force delivered to the body, (2) the time over which the force is delivered, (3) the body region struck, and (4) the surface area of the body over which the force is delivered. 25 When a force is applied to an object, its acceleration in space depends on its mass according to Newton’s second law:

The energy that the object acquires and retains as long as it is moving is defined as kinetic energy. 71 This energy is the force transferred to another body when blunt trauma occurs, and it depends on the following formula:

This explains the ability of an object to induce an injury, mild or severe damage, depending on its weight and velocity: light objects that are accelerated to high velocity or heavy objects that impact slowly can deliver the same kinetic energy to the struck area, even though they produce different wound patterns (see the Contusions section).
Another crucial factor is the relative movement between the body and the impacting object. When the body is static, the severity and shape of the injury depend on the ability of the impacting object to displace the body. Similarly, when the moving body strikes a stationary object, the severity of the injury is dependent on the extent to which the object can stop the motion of the body and the degree of possible deformation (plasticity) of both. If both the body and the object are in motion, the amount of kinetic energy can be increased or diminished according to the relative directions of their movement. The more the surfaces of the body and of the object are able to deform, the milder the lesion, because a substantial amount of kinetic energy is dissipated in deforming the body and/or object without breaking their structure. 71
Thus, tissue injury is influenced by the plasticity of the tissue and the time over which the force is delivered. If the object or the body region are very plastic, the period of impact and thus the time over which the kinetic energy is released will be lengthened, causing the colliding surfaces to change in shape and therefore reducing the energy transferred and the damage provoked. In principle, the difference between a caress and a slap is the time of application of force. The rapidity of the delivered force also influences the resulting damage. A typical blunt trauma caused by a weapon is normally delivered within fractions of a second, leaving minimal opportunity for tissue adaptation, whereas a constricting force applied for a long period of time leads to tissue adaptations that may limit the resulting tissue damage.
The anatomical structure of the body region similarly affects the severity and appearance of the wounds. This is a direct consequence of the plasticity of the tissues. For example, the same force perpetrated with the same blunt weapon can lead to different traumatic lesions if delivered to the skull (where the minimally plastic bone is immediately beneath the skin) or to the shoulder region of a dog (where the bone is embedded deep below the plastic soft tissues). 25,39 In veterinary forensic pathology, the species, breed, age, and nutrition state influence the anatomic structure and thus the damage resulting from blunt trauma. Furthermore, differences in the plasticity of anatomic structures that are in the path of the waves of kinetic energy modify the morphology and severity of traumatic lesions in deeper tissues. Thus, the application of kinetic energy to the lateral abdominal wall will propagate through the tissues until it reaches those with reduced tolerance to mechanical stress such as the liver. The tolerance to stress normally relates to the organ’s structure and its mobility within the body cavity. Thus, the functional or pathologic state of an organ also influences the outcome of blunt force to the body surface, and diseased organs may incur greater (eg, degenerated organs) or lesser (eg, fibrotic organs) damage than healthy organs. Parenchymatous organs can react differently from tubular organs containing gas or fluids. In the latter, dissipation of kinetic energy displaces gas or liquid, which can cause pressure-induced injury. The area over which the kinetic energy is released also affects the degree of injury. The rule of thumb is that the smaller the area over which the energy is applied, the greater the disruption of the affected tissues. 39
Finally, the extent and severity of a traumatic lesion does not always match the clinical consequences: A moderately severe lesion in a vital organ can lead to death, while a severe lesion in a nonvital organ may be nonfatal.
Conversely, blunt trauma can lead to clinically important alterations without any macroscopic or microscopic lesions (eg, concussion; see the Cranial Cavity and Brain section).
Blunt Trauma to the Body Surface
Lesions of blunt trauma to the skin and subcutis are very common in veterinary pathology, yet the thick hair coat, thick skin, and epidermal pigmentation of many animals may minimize or obscure external injuries and make it essential for veterinary pathologists to search meticulously for evidence of superficial blunt trauma. Skinning of the entire body is necessary to detect such wounds. In special circumstances, clipping of the hair coat is also needed to reveal abrasions. The three typical lesion patterns caused by blunt force trauma to the skin and subcutis are abrasions, contusions, and lacerations, 25,39,50,52 but all 3 may occur simultaneously, such as the abraded margins of a laceration overlying a soft-tissue contusion.
Abrasions
An abrasion is defined as a skin injury in which the epidermis has been removed by friction against a rough surface or has been destroyed by compression, 25 resulting in focal loss of the epidermis, with minimal extension to the dermis. The literature varies with regard to the latter 39 : a pure abrasion (ie, a wound that does not extend beneath the epidermis) would in theory not bleed; however, as bleeding is often seen with abrasions, a working definition should consider that the most superficial dermal layers can also be involved. Complete absence of bleeding is rare because of dermal vascularization, 39 and small focal hemorrhages can be readily identified by histology.
Based on the angle of impact with the skin, abrasions can be classified as scrape (or brush), impact (or crush), and/or pattern abrasions when the morphology of the wound indicates the object that caused the lesion. 25,39
Scrape Abrasions
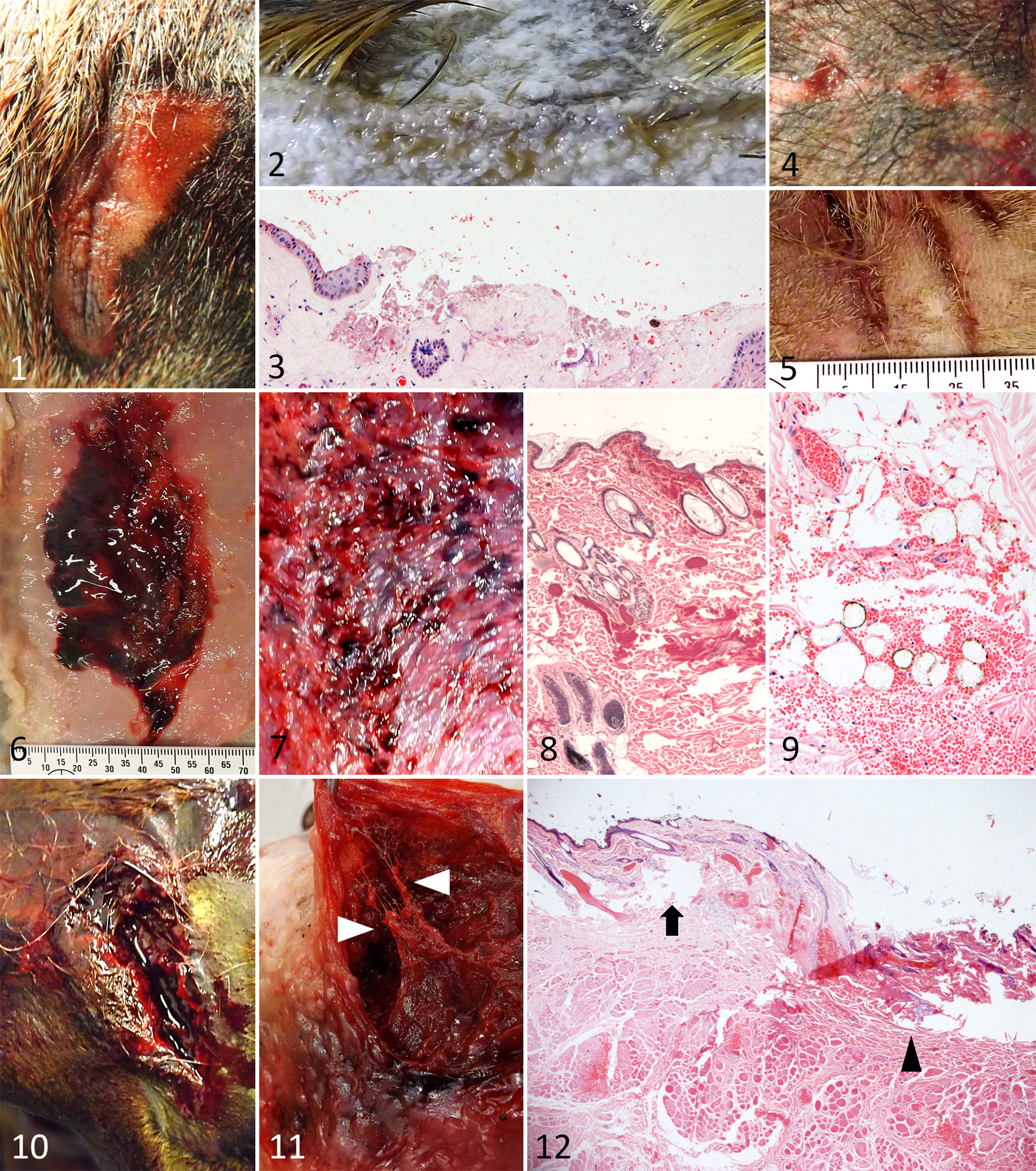
In scrape abrasions, the object hits the body surface tangentially. Therefore, the area of epidermal detachment is larger than the surface area of the object, which explains why scrape abrasions rarely indicate the shape of the offending object. 25 Grossly, scrape abrasions appear as variably sized areas of exposed superficial dermis (Figures 1 and 2); in haired animals, this is generally associated with the presence of broken hair shafts. The gross examination itself provides some information on the direction of the impact; in humans, the area of deeper abrasion and more extensive hemorrhage is likely the area of impact, while the “tail” of the lesion is usually more superficial and exhibits less bruising. 39 While in our experience, such an interpretative approach is valuable, other authors questioned its reliability 25 : it has been shown in humans that when the angle of the impact is particularly narrow (acute), the epidermis can be “rolled” or elevated at one margin, which provides evidence of the direction from which the impact hit, and it has been suggested that an epidermal tag represents the terminal area of impact, thereby allowing for the determination of its direction. 39 Such knowledge is only partially helpful in veterinary forensic pathology, as the hair of most domestic animals will act as a cushion and may alter the pattern, as expected in humans. Artifactual changes (eg, due to handling of the carcass) can alter the shape of the lesion and hamper its interpretation.
Blunt trauma to the skin and subcutis.
Scrape abrasions are probably the most common abrasions in animals. In our experience, they are particularly frequent in larger animals, probably because of the substantial resistance of their body mass to the tangential blow. Scrape abrasions are found almost invariably in animals that have been hit by a motor vehicle, 52 and upon detailed examination, inorganic material (eg, tire rubber, asphalt, soil) can often be retrieved, providing useful information on the scenario. 52
Histologically, scrape abrasions are characterized by focal epidermal detachment, often with disruption and hemorrhages in the dermis (Figure 3). Small focal hemorrhages, as are frequently seen also in deeper areas of the dermis, are likely the consequence of local contusion.
Impact Abrasions
This uncommon type of abrasion occurs when the surface of an object hits the skin perpendicularly. In humans, this leaves an imprint on the skin. In animals, a visible imprint is likely only in sparsely haired areas and very close to an underlying bone. Impact abrasions are also observed occasionally on the supraorbital ridges of horses that fall to the ground during the agonal phase. In our experience, pure impact abrasions are extremely rare in animals. Instead, most impact abrasions are associated with contusions and/or lacerations and thereby represent mixed blunt trauma. However, multiple impact abrasions inflicted upon a cat by a clothes dryer have been described resulting from repetitive impacts of the smooth metal surface of the dryer. 50
Pattern Abrasions
Pattern abrasions reflect the shape of the object that caused the lesion (Figures 4 and 5). These may be considered together or separate from the above patterns. While pattern abrasions are of great importance in humans involved in motor vehicle accidents and in many other scenarios, they are infrequent in animals and seen only in shorthaired animals or in sparsely haired regions. In humans, fingernail abrasions are of major relevance in the context of crime scenes. 39 In domestic animals, nail abrasions are probably the most common genuine pattern abrasions. Their shape is strictly dependent on the nail shape of different species; roughly circular marks are produced by primates (Figure 4), whereas canids induce narrow elongated marks (Figure 5). Our case material suggests that the nails of cats and large felids as well as birds of prey are more likely to produce abrasions with lacerations, penetrating puncture wounds, or pure lacerations. We have also identified abrasions induced by human fingernails in animals with short hair that have been strangled. In cases of sexual abuse (or other types), the inner pinna, vulva, and inguinal skin may be abraded by human fingernails (often with typical crescent shaped abrasions). In primates, socially patterned fight schemes result in fingernail abrasions mainly on the neck, face, arms, and forearms. 10
Contusions
Contusions (bruises) are found at the site of an impact that did not lead to disruption of the continuity of the overlying (epidermis) tissue. They are characterized by the presence of extravasated blood (hemorrhage) beneath the intact epidermis. In humans, bruises are focal areas of discoloration identified externally, and their color changes with the age of the lesion. 25,39 In domestic animals (with some exceptions such as birds or pigs), bruises are seldom evident upon external examination because they are obscured by hair and pigmentation of the skin. Therefore, bruises are best identified after complete skinning of the animal and careful examination of the subcutis for hemorrhages. In humans, some bruises may become evident on the skin only in the postmortem period, after the blood has had sufficient time to emerge. 25 This is believed to result from extension of free blood from its origin in deeper tissues upward to the epidermis, along with hemolysis and release of hemoglobin that stains the tissues more intensely. 25 In our experience, this phenomenon is not applicable to domestic animals. Instead, complete skinning as soon as possible after death is needed to optimally visualize bruises. Grossly, bruises represent focal accumulations of blood that are evident from the subcutaneous surface of the skin (Figure 6). Multiple small pinpoint (1 to 3 mm) hemorrhages (petechiae) may result from trauma where friction causes mechanical stretching and rupture of capillaries (Figure 7). Histologically, a bruise presents as an accumulation of extravasated erythrocytes within the different subepidermal soft-tissue layers. Such hemorrhages can occur at all levels of the dermis (Figure 8) and subcutis (Figure 9). In our experience, however, bruises are far more common in the subcutis than the dermis and may extend into the superficial muscle layer. 39 In small bruises, extravasated erythrocytes tend to infiltrate tissues with a looser texture (eg, adipose tissue). A hematoma can develop within more severe bruises. 52 Depending on the amount of pooled blood and the time after injury, blood may migrate along fascial planes to appear as a bruise distant from the traumatized area, and the direction of gravitational flow depends on the animal’s position before or after death. 25 As well as postmortem changes that can mimic areas of contusion (see the section Distinction Between Antemortem and Postmortem Blunt Trauma), other intravital conditions such as septicemia, anticoagulant toxicity, and coagulation disorders can lead to subcutaneous or dermal hemorrhages. Thus, histologic or cytologic examination of the bone marrow is recommended in a forensic postmortem examination. Hemorrhages resulting from coagulopathies differ from traumatic contusions with respect to their distribution and absence of associated damage: traumatic lesions are generally localized and may have underlying fractures or other injuries, whereas the distribution of hemorrhages secondary to other diseases may be disseminated or inconsistent with a trauma. The size of a bruise is generally dependent on the severity of the blunt trauma. However, the extent of bruising is also dependent on the underlying vascular network, the volume of the subcutaneous tissue, the fragility of the blood vessels, and an individual’s hemostatic parameters. Therefore, care should be taken in inferring the severity of blunt trauma from the extent of a bruise, particularly if the coagulation status of the animal is unknown. Furthermore, the size of a bruise is also influenced by the anatomic area subjected to the mechanical force. As a general rule, bruises are most prominent in areas of the body with a small amount of subcutaneous tissue and where muscle is directly overlying bone (such as the head) because this tissue is easily compressed even when only minimal force is applied. In contrast, the abdominal wall and the thighs are less prone to bruising when the same level of force is applied. The vascularity of the wounded tissue also determines the number of ruptured vessels and consequently the amount of extravasated blood. Finally, the laxity of the tissue adjacent to the lacerated blood vessels and the depth at which the bleeding originates can affect the propagation of the bruise. 25,39 Slow-moving heavy objects usually cause deep muscular hemorrhage, whereas high-speed, lightweight objects are more likely to cause a rapidly developing superficial bruise, even though both deliver the same kinetic energy. 65
Pattern Contusions
Similar to abrasions, contusions can also have a shape that indicates the striking object.
A “tram line” bruising pattern is often seen when the victim has been struck by a rectangular or cylindrical object, and it appears as 2 parallel lines of bruising with an undamaged area in the center. 39 This phenomenon is due to maximal stretching of the tissue at the border of the area compressed by the impacting object. Representative examples of pattern contusions in animals are provided in several publications. 4,32,56 However, as mentioned for pattern abrasions, pigmentation, hair, and other features of animal skin often obscure pattern contusions in animals.
Lacerations
A laceration is a tear in the tissue that results from the application of a crushing or stretching force to the skin. A blunt object or surface generally induces a laceration where the skin and underlying connective tissue are stretched over a superficial prominent bone, providing a firm base that acts as an anvil for the skin. 39 In areas with no underlying bone, a similar lesion can occur when a sharper object crushes the skin. Thus, the site of a laceration can suggest the shape of the impacting object: a laceration in a body region where a bony prominence underlies the skin can be the result of a blow by a decidedly blunt object (eg, a pipe or a walking stick), while in a region with large amounts of muscle or adipose tissue, it can be induced only by a sharper object (eg, teeth or a blunt axe).
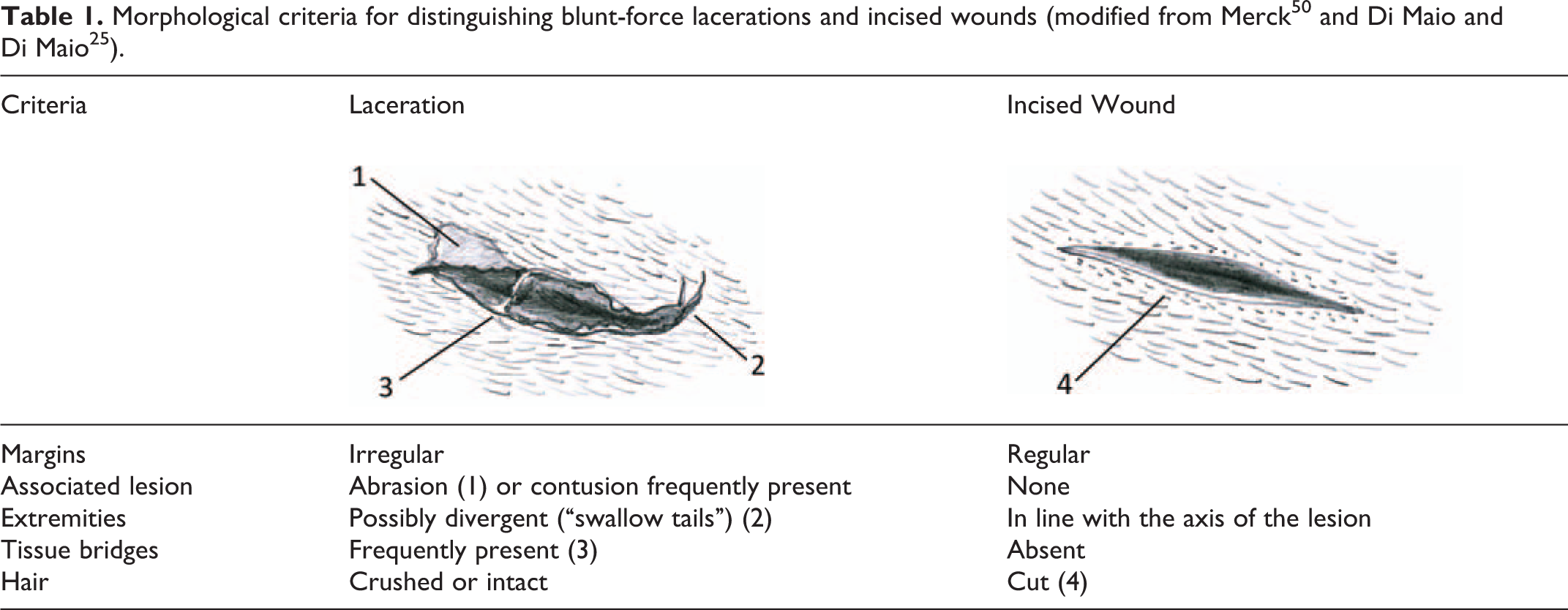
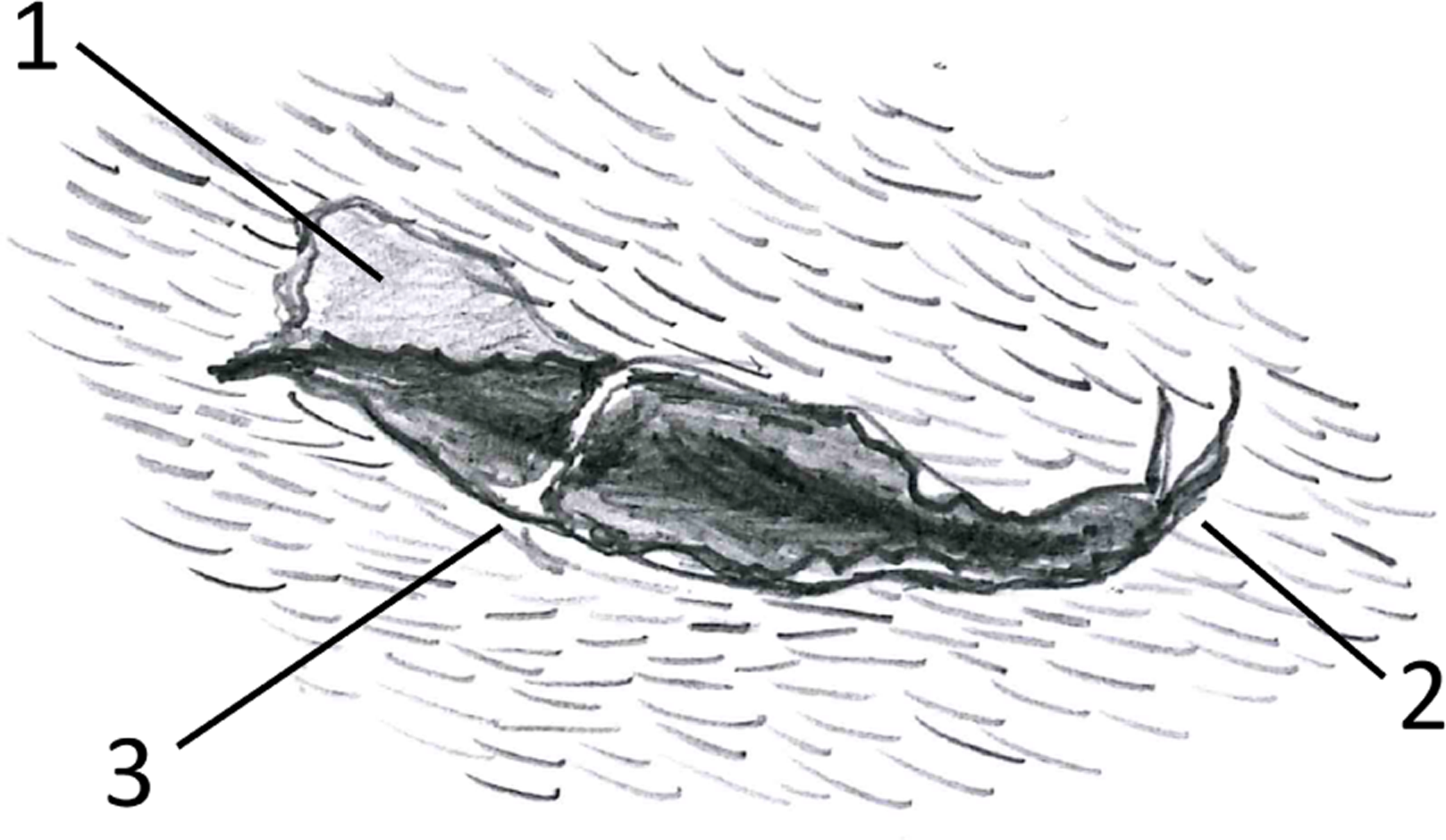
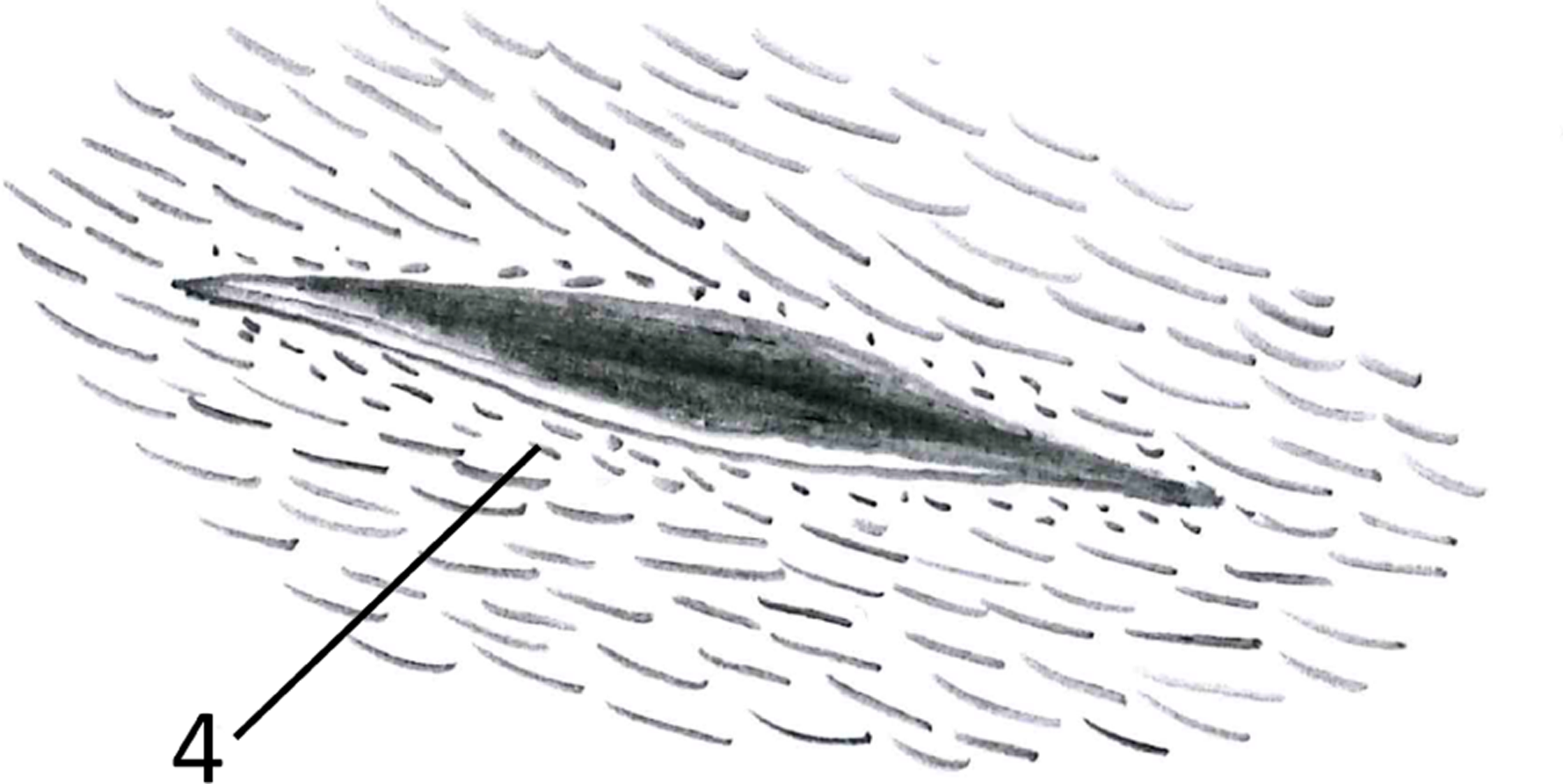
Grossly, lacerations are characterized by variably shaped tissue tears of variable depth with irregular margins (Figure 10). When more resilient tissue components, such as vessels and nerves, remain intact, they are often found crossing the tear; such “tissue bridging” is a definitive indicator of a laceration (Figure 11). 25 The endpoint of a laceration often exhibits a further tear that diverges from the main axis of the laceration. Such “swallow tails” develop when a tear follows definite anatomical lines of cleavage. 25 A laceration is invariably associated with hemorrhage. As for a bruise, its extent depends on several factors, such as the anatomy of the region, the depth of the wound, and the coagulation state. A crushing force usually induces a laceration with ragged margins and abrasions of the adjacent skin where the striking object has rubbed against the skin. Careful examination of the margins may provide further information: the wound often exhibits an abraded margin at one side; as this is the point where the object first made contact, it indicates the direction from which the blow was applied. 25 A perpendicular blow results in a laceration with symmetrical edges, whereas asymmetrical edges are the result of a tangential blow. 39 When a very strong force is applied, one of the margins can be torn off; for such lesions, the term avulsion has been suggested. 25 Lacerations need to be distinguished from incised wounds caused by sharp force trauma. As the latter are discussed separately in the same issue of the journal, 22 we restrict their discussion at this stage to a list of the morphological criteria that allow distinction between the 2 types of lesion (Table 1). Microscopic analysis of the hair at the margin of the lesion can provide further information, as crushed hairs are found in a laceration, whereas an incised wound contains cut hair shafts. 68 Histologically, lacerations are characterized by locally extensive tissue distortion and disruption with associated hemorrhages (Figure 12). In many cases, the damaged tissue appears hypereosinophilic and crushed. Material from the object or surface that induced the laceration can often be detected at the surface of the wound or embedded within it; this can provide information for the identification of the causative object.
Pattern Lacerations
As with abrasions and bruises, pattern lacerations are those in which the shape of the lesions suggests the causative object. Although it is known that the shape of a laceration does often not exactly match the shape of the impact surface of the striking object, 25 there are examples of lesions in humans for which a correct match of the weapon used can be found. 39 In veterinary medicine, examples of pattern lacerations are rare. A series of pattern lacerations have been described in marine mammals with lethal propeller strikes; in this case, linear wounds, sometimes associated with fractures of underlying bones, were observed. 14 In animals, bite wounds and gunshot wounds are probably the most common pattern lacerations; the former will be discussed separately in the present review, while the latter is discussed more extensively in a separate article in this issue. 11
Blunt Trauma to the Nails and Footpads
In our experience, fractures of the nails and abrasions/erosions of the footpads are frequent injuries of the extremities in carnivores. Nail fractures are commonly found in dogs and cats that are hit by motor vehicles, 52 but we also observed excessive wear or fracture of nails in animals that died under other circumstances. These included cases of hanging when a vertical surface was close enough for contact in association with hyperactivity during the agonal phase and in cases in which animals were trapped alive inside a closed container such as a suitcase. Fragments of material present from the contact surface might be present on or near the injured nail and may represent important evidence for the investigation. 52
Blunt Trauma to the Musculoskeletal System
Skeletal Muscles
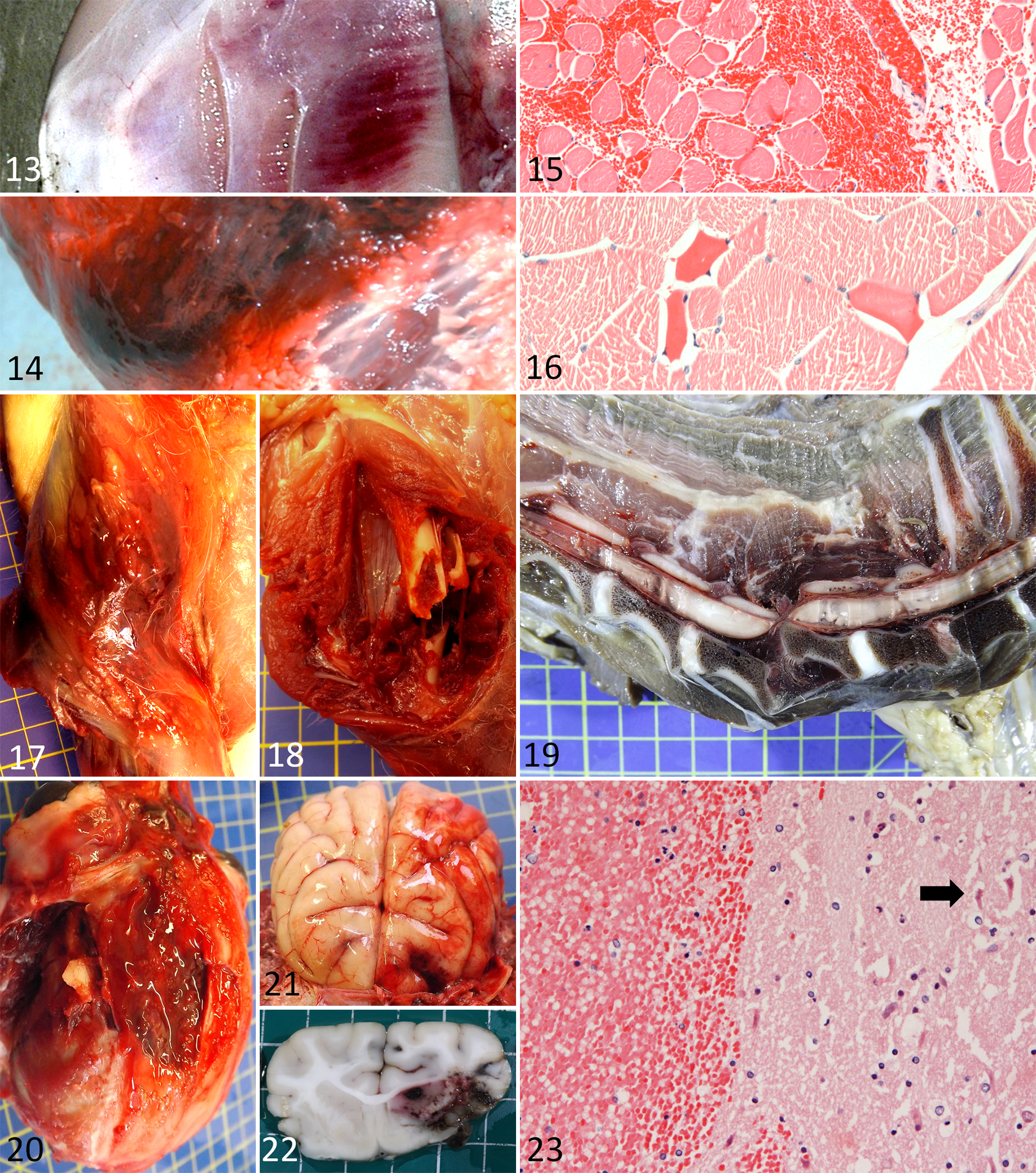
According to our experience, muscle trauma is the second most common traumatic lesion in forensic veterinary cases, after subcutaneous contusions. While muscle contusions are most common, muscle lacerations are also seen as a consequence of penetrating blunt trauma. Muscles are immediately beneath the skin over almost the entire body. Considering the resistance that the heavily haired skin of domestic animals offers to blunt trauma, careful examination of the underlying muscles can often clarify whether a severe blunt trauma was applied. Grossly, muscle trauma can range from small focal bruises that often infiltrate between muscle fibers (Figure 13) to large bruises with hematoma formation (Figure 14). The gross appearance is generally determined by the same parameters as skin bruises; however, in the muscle, bone in the vicinity will often increase the severity of tissue damage and hemorrhage. The histologic picture shows large numbers of extravasated erythrocytes that dissect the myofibers (Figure 15). In our experience, when the trauma is associated with vigorous compression and stretching of muscle fascicles (eg, muscle lacerations with bone dislocation due to a car accident), segments of hypereosinophilic myofibers with loss of striations are occasionally found close to the site of the impact (Figure 16). Similar changes have been previously documented in the muscles of pigs subjected to blunt trauma. 4 With time, the lesions change according to the evolution of a hemorrhagic process, with initial nonseptic rhabdomyolysis, followed by leukocyte influx, myotube formation, and repair. Connective tissue scarring will develop in sites of muscle laceration. 42
Blunt trauma to the musculoskeletal system.
Bones of the Limbs
Bone is a relatively elastic tissue that tolerates strong mechanical stress, but severe blunt trauma can lead to fracture. With the latter, the bone usually breaks at a leverage point (point of maximum tension). 18 The classification of bone fractures is found in veterinary textbooks. In human forensic pathology, specific fracture patterns are described in association with particular types of blunt trauma, 25 but specific fracture patterns have not been described in animals. 52 Bone fractures are classified as physiologic when affecting a healthy bone or pathologic when affecting a structurally altered, weaker bone. The possibility of pathologic fracture should be taken into account in forensic cases where multiple fractures are detected. 52 Fractures can also be classed as “direct” or “indirect,” depending on whether the causative force is applied directly to the site of the fracture or distant from it. With direct fractures, the kinetic energy can either produce a crush at the site of the impact or can lead to bending of the tissue and, potentially, cracks at the opposite side. 25 In this particular situation, radiographs can be of use for the identification of the site of impact, based on the presence of small bone fragments disseminated within the adjacent tissues. 71 Indirect fractures result from the application of several types of force to the bone: traction, twisting, rotation, compression, or a mixture of the aforementioned. In humans, the morphological features of the fracture can suggest the type of force applied. 25 As the bone structure of most domestic animals is similar to that of humans, 58 this system may suggest an interpretation in forensic veterinary medicine. Most limb fractures are not associated with external gross lesions unless there is an open compound fracture. Upon dissection of the tissues, however, hemorrhages and possibly lacerations within soft tissues and muscles become evident (Figure 17). The margins of recent fractures are sharp (Figure 18), while callus formation is associated with subsequent healing (see rib fractures in the section on the thoracic cavity).
Histologically, bone fragments are found in association with hemorrhages in the early phase; followed by the formation of a hematoma, fibrous tissue, woven bone, and/or cartilage in later phases (calluses); and finally lamellar bone is formed with healing and callus formation. 42 Similarly to that described in humans, 12 we have occasionally found histological evidence of bone marrow emboli as a consequence of multiple severe fractures. Blunt trauma applied to the bones of the limbs can also cause luxations or subluxations. Depending on the site, they can lead to intra-articular hemorrhages, ligament rupture, tendon laceration, and further associated soft-tissue damage.
Vertebral Column
The vertebral column is relatively protected from blunt trauma as several muscle groups attach to the vertebrae. Nonetheless, particularly severe trauma can lead to fractures or luxations. Care should be taken to identify or exclude preexisting pathological conditions that may predispose the vertebral column to fractures. In this context, species- and breed-related conditions (eg, disk herniations) are of relevance. Therefore, longitudinal sagittal or parasagittal sectioning of the vertebral column is essential to examine the spinal cord and vertebrae. Blunt force of a severity that can fracture or luxate the vertebral column generally damages the spinal cord irreversibly (Figure 19). Grossly and histologically, hemorrhages in the spinal cord and/or the surrounding soft tissues (mainly muscles) can be seen in the region of the fracture or luxation.
Blunt Trauma Affecting the Head, Thorax, Abdomen, and Pelvis
Cranial Cavity and Brain
The neuropathology of trauma is dealt with separately in this issue 30 and is covered only minimally here. The brain is a vital, highly specialized, and extremely delicate organ intimately surrounded by 3 layers of variably vascularized meninges and encased in protective bone (calvarium). The dura mater, the most external meningeal layer that also serves as periosteum for the calvarium, is separated from the neuroparenchyma by a continuous film of cerebrospinal fluid that also protects the brain. It is this fluid layer in which the brain is suspended and the rigid calvarium contributes significantly to the high susceptibility of the brain to blunt trauma. When a moving head comes to a sudden stop due to contact with a surface (negative acceleration or deceleration), the side of the brain contralateral to the impact will develop more severe hemorrhages due to shearing and tension applied to the meningeal vessels and negative pressure that leads to vascular rupture and bleeding (contrecoup). 60 On the other hand, when a blow hits the skull, most of the kinetic energy of the impacting object is dissipated into tissue deformation at the site of direct contact. The consequent recoil of the skull will damage the brain directly; therefore, the only or the most severe hemorrhage is detected at the impact point (coup lesion), which may also have contusion of soft tissues and possibly fracture of the skull (Fig. 20).
Hemorrhages are the most characteristic gross lesions resulting from blunt trauma to the brain (Fig. 21), but contusion and laceration can also be seen. The term contusion is used for hemorrhages with preserved leptomeningeal integrity, while cortical lesions with discontinuity of the leptomeninges are considered lacerations. 59 After fixation and serial sectioning of the brain, areas of contrecoup contusion can frequently also be detected (Fig. 22). Histological examination of early lesions shows intact erythrocytes around vessels, filling and distending the Virchow-Robin and subarachnoid spaces. More severe lesions are represented by multiple small hemorrhages that tend to coalesce and create multiple erythrocyte “lakes” centered on engorged vessels in the cortex and underlying superficial white matter. With time, a series of pathological changes will be seen. Following extravasation of erythrocytes and mechanical damage of neurons, lysis of erythrocytes and neuronal cell death are evident (Fig. 23). Concurrently, an inflammatory response will be initiated, represented by the recruitment of leukocytes and activated astrocytes and microglia. 16,24 With time, lesions contain hemosiderin-laden macrophages, lymphocytes, gitter cells, and progressively expanding areas of parenchymal rarefaction. 60 In some cases of blunt brain trauma, especially those developing as a consequence of kinetic energies inducing strong acceleration and applied from an angle, marked hemorrhage occurs in deep and axial locations, as mechanical stretching will rupture large vessels around the main impact area.
Blunt trauma to the skull can result in functional damage to the brain without detectable gross or microscopic changes (concussion). In humans, this is often seen after mild trauma or rotational acceleration that preferentially causes axonal stretching and functional impairment without appreciable morphological alterations. 60 Therefore, the absence of lesions does not entirely rule out a trauma to the brain.
A direct association has been shown between the size of the surface of impact and the area over which the fracture develops 71 ; conversely, small, fragmented, and often depressed fractures occur when strong force is concentrated on a small area. 50 We frequently observed large depressed fractures of the calvarium when the impact surface was wide. However, in our experience, fracture lines can also extend along natural suture lines, rendering the fractured fragment larger and more complex than the actual area of impact.
Eyes
Eyes can be the direct target of blunt force trauma, resulting in hemorrhages such as within the sclera, orbit, anterior chamber (hyphema), or filling the entire globe. In addition, orbital hemorrhage resulting from severe cranial injuries often leads to protrusion of the eye bulb (traumatic proptosis) and multifocal ecchymoses due to percolation of blood from the primary site of the bruise. In some cases, ocular injuries are the only reported external gross evidence of a trauma to the head. 50 Histological evaluation of traumatized eyes is recommended for confirmation of grossly identified lesions and to detect additional changes such as retinal detachment.
Thoracic Cavity
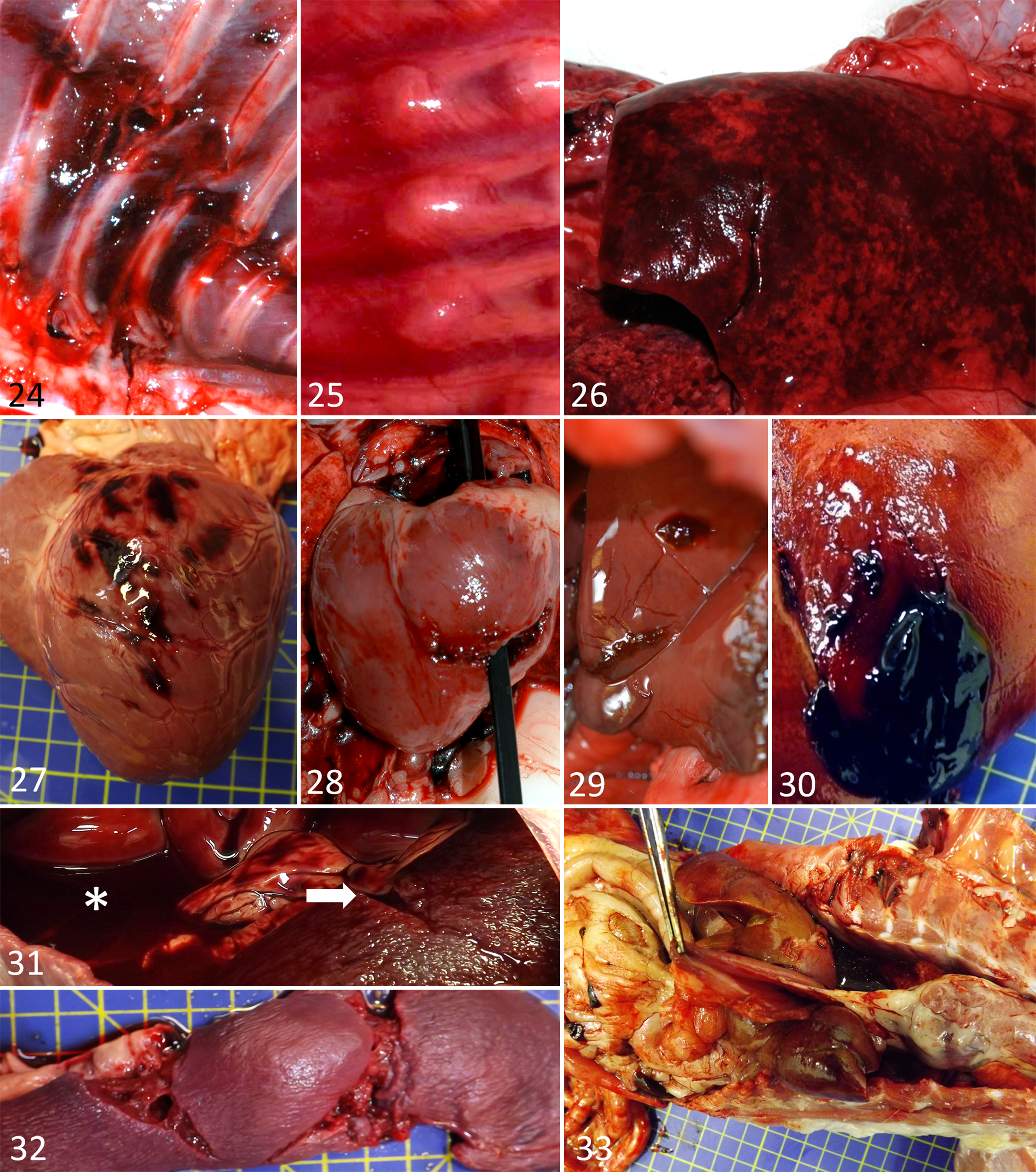
In animals, the chest wall makes the vital thoracic organs less susceptible to blunt trauma than those of the abdomen. However, acuminated blunt objects can perforate the intercostal muscles and cause severe deep damage and pneumothorax or hemothorax, comparable with sharp force injuries. If the thoracic cavity sustains the impact without structural damage, the kinetic energy is transmitted to the internal organs, leading to internal trauma even without obvious external lesions 50 ; nonetheless, focal hemorrhages are often found within the stretched intercostal muscles upon careful examination. 52 Rib fractures are a common feature of nonaccidental injuries. 23,54 They indicate dissipation of the energy applied to the bone. Differences exist in the anatomy of the rib cage of domestic animals, with some being more plastic (eg, rabbits) than others. Age also influences the elasticity of the ribs; those of young animals are more elastic and difficult to break, whereas they are more brittle in older animals. 52 Features discussed for the long bones of the limbs are also relevant for the ribs. Some authors are of the opinion that rib fracture patterns (eg, bilateral fractures) are indicative of certain types of nonaccidental injury, 50 although this is debated by others. 52 Rib fractures often affect 2 or 3 adjacent ribs (serial fractures) 50 that exhibit sharp margins when recent (Fig. 24) and callus formation when old (Fig. 25). With comminuted rib fractures, bone fragments often cause lacerations of internal organs such as the heart and lungs. 52
Blunt trauma to the thorax.
Lungs
Being closely apposed to the rib cage, the lungs can be damaged as a direct consequence of blunt trauma to the thoracic wall. This manifests as bruising of the parenchyma with formation of superficial rib imprints or focal parenchymal hemorrhages due to rupture of larger vessels. 52 Because of their spongy structure, lungs are highly elastic tissues; however, the delicate capillary network of the alveolar walls, together with the tissue distention caused by inspiration, make them prone to rupture. Grossly significant lung damage may occur in association with severe trauma such as motor vehicle accidents 72 and can be associated with extensive bruising and bulla formation with potential subsequent pleural rupture. 52 When blunt trauma causes rib fractures, bone fragments can lacerate the lungs (Fig. 26), leading to leakage of air and pneumothorax, even when the integrity of skin and subcutis is preserved.
Heart and Pericardium
The heart is reasonably protected by both the ribcage and the lungs; however, in severe trauma, it can suffer concussions, contusions, or lacerations, in particular via dissipation of an applied force to the sternum.
Cardiac concussion (commotio cordis) can lead to sudden death from cardiac arrest in the absence of visible cardiovascular trauma. 40 In a canine model of cardiac concussion, despite the absence of either gross or histopathological changes, severe disturbance of cardiac functionality occurred following impact against the sternum. 35 At a higher degree of severity, cardiac contusions are grossly evident as focal or multifocal areas of myocardial hemorrhage (Fig. 27). These must be differentiated from infarcts in which the hemorrhage is usually less marked. 57 Areas of contusion can progress to necrosis and repair, creating areas of weakness that can develop into abnormal structures such as aneurysms and may be prone to rupture. 70
Heart lacerations are described in human forensic pathlogy. 8 In our experience, those are rare consequence of blunt trauma in animals and are seen only with very severe forces (such as falls from a considerable height). They can involve both atria and ventricles (Fig. 28). For the myocardium to be prone to laceration, sufficient tension of the heart wall has to be built up. Accordingly, the trauma has to occur during the systole to affect the atria and in diastole to affect the ventricles. 57 Cardiac lacerations that do not result in death of the animal can heal with fibrous scars; these can potentially lead to dysrhythmias as can also occur subsequent to contusions.
Laceration of the pericardium is rare but can be induced by bone fragments from rib fractures due to penetrating blunt trauma. 51 Like heart lacerations, pericardial lacerations can cause hemopericardium. This needs to be differentiated from the serosanguineous pericardial fluid that is often present in frozen-thawed carcasses as a postmortem change. 49,52
Large Vessels of the Thorax
Damage to the large arteries and veins is a rare consequence of blunt trauma, 71 whereas it is commonly seen with chest injuries due to sharp or penetrating force trauma. This is likely due to the high elasticity of the large blood vessels and their fluid content, which serve as a shock cushion. However, in some circumstances, the hydrostatic pressure may be high enough to rupture a more fragile area of a vessel. For example, a severe blow to the sternum can result in rupture of the base of the aorta as a result of motor vehicle accidents in humans. 70 In general, however, a preexisting condition affecting the vessel wall needs to be excluded when a large vessel is found ruptured at postmortem examination. Exceptionally, we observed the rupture of the thoracic vena cava in a cat after a fall from a great height.
Abdominal Cavity
Differing from the thoracic wall, the abdominal wall is composed of resistant but very elastic and movable muscle layers that almost completely surround the cavity and its voluminous organs. Moreover, while the thorax is protected by ribs, the blades of the scapula, and the extensive musculature of the proximal forelimb, the abdominal cavity is longer, more exposed, and easily accessible when a blow is intended toward the body. Bruises may not be seen after blunt trauma to the abdominal wall, as the kinetic energy from impacting objects is dissipated into tissue deformation and then transferred to internal organs. The organ damage occurring after blunt trauma to the abdominal wall correlates with organ volume, texture, and motility. 25 The kinetic energy transferred from blunt trauma through the deformable abdominal wall will be dissipated in large compact organs with restricted mobility, resulting in contusion and lacerations.
Liver
In both humans and animals, the liver is the abdominal organ that is most commonly and most severely affected by blunt trauma. 25 It is the combination of structural features, such as the large organ volume, the friable texture, the lack of elastic tissue, and the intense vascularity that renders the liver particularly susceptible to the effects of blunt forces. Lacerations of the liver often lead to life-threatening abdominal hemorrhage; therefore, it is important to measure the amount of free and clotted blood during the postmortem examination. The degree of tissue deformation reaches critical levels when the liver arrives at the costal arch and/or the vertebral column and the acceleration is suddenly reduced. 25 Depending on the extent of the trauma, radiating lines of parenchymal laceration are observed (Fig. 29) at both the ipsilateral and contralateral sides of the impact (coup and contrecoup lesion), either beneath an intact capsule (subcapsular laceration) or in association with adherent blood clots when the capsule is breached (transcapsular laceration; Fig. 30). Alternatively, subcapsular bleeding and hematoma formation can subsequently lead to capsule rupture and fatal bleeding into the abdominal cavity. Histologically, there are large areas of hepatocyte dissociation and disintegration due to extravasated blood expanding and effacing sinusoids. In the absence of coagulation disorders and with mild parenchymal damage, tissue repair can result in the formation of retracting scars.
Spleen
The spleen is smaller and more mobile, located under the left rib arch of the epigastric region, which ensures that it is better protected from blunt trauma. This accounts for the relatively lower incidence of splenic lacerations, which, when they do occur, almost invariably result in severe and potentially fatal bleeding (Fig. 31) owing the high level of vascularity. When the spleen is physiologically or pathologically enlarged, its susceptibility to severe blunt trauma is markedly increased. As in the liver, depending on the applied force, traumatic deformation of the spleen could result in subcapsular tears only or, in the extreme, complete organ laceration (Fig. 32). Bleeding beneath the intact capsule can induce hematoma formation; this can regress and be organized into fibrous scars or can increase in size, predisposing the spleen to ruptures and bleeding, even a long time after the original blunt trauma. 25
Other Organs
The muscular wall and the high flexibility and mobility of the gastrointestinal tract are extremely efficient in reducing the traumatic effect of blunt impacts to the abdominal wall. Contusions and laceration, especially of the stomach, can still occur and are generally associated with a blow inflicted on areas of the abdominal wall directly opposed to hollow organs distended by either solid or gaseous content. Because of the extreme mobility of the intestinal loops, vessel tears and associated mesenteric hemorrhages can be observed. 52 When the abdomen is forcefully compressed by heavy objects that produce high intra-abdominal pressure, as occurs when an animal is run over by a car tire, laceration of the diaphragm and/or the pelvic region can result in herniation of abdominal organs (Fig. 33). The urinary bladder is another hollow organ susceptible to damage. When empty, the bladder is almost completely protected by the pelvis. However, when distended by urine, a severe blow to the caudoventral abdomen can compress the organ against the lumbo-sacral spine and induce a sudden increase in pressure and laceration, resulting in leakage of urine into the abdomen (uroperitoneum). 52 Because of their minimal mobility and the protection warranted by the lumbar spine, kidneys are seldom affected by blunt trauma. We observed subcapsular contusion and laceration of the kidneys only in rare cases of extremely severe abdominal injury.
Pelvic Cavity
Because of the strong bone and muscle belt, the pelvic cavity and its organs are relatively protected from blunt trauma, and only an extreme force can disrupt the pelvic ring. 25 The pelvis is crushed more often in dogs hit by motor vehicles than with nonaccidental injury. 41
Special Forms of Blunt Trauma
Compression: Constriction and Pressure Sores
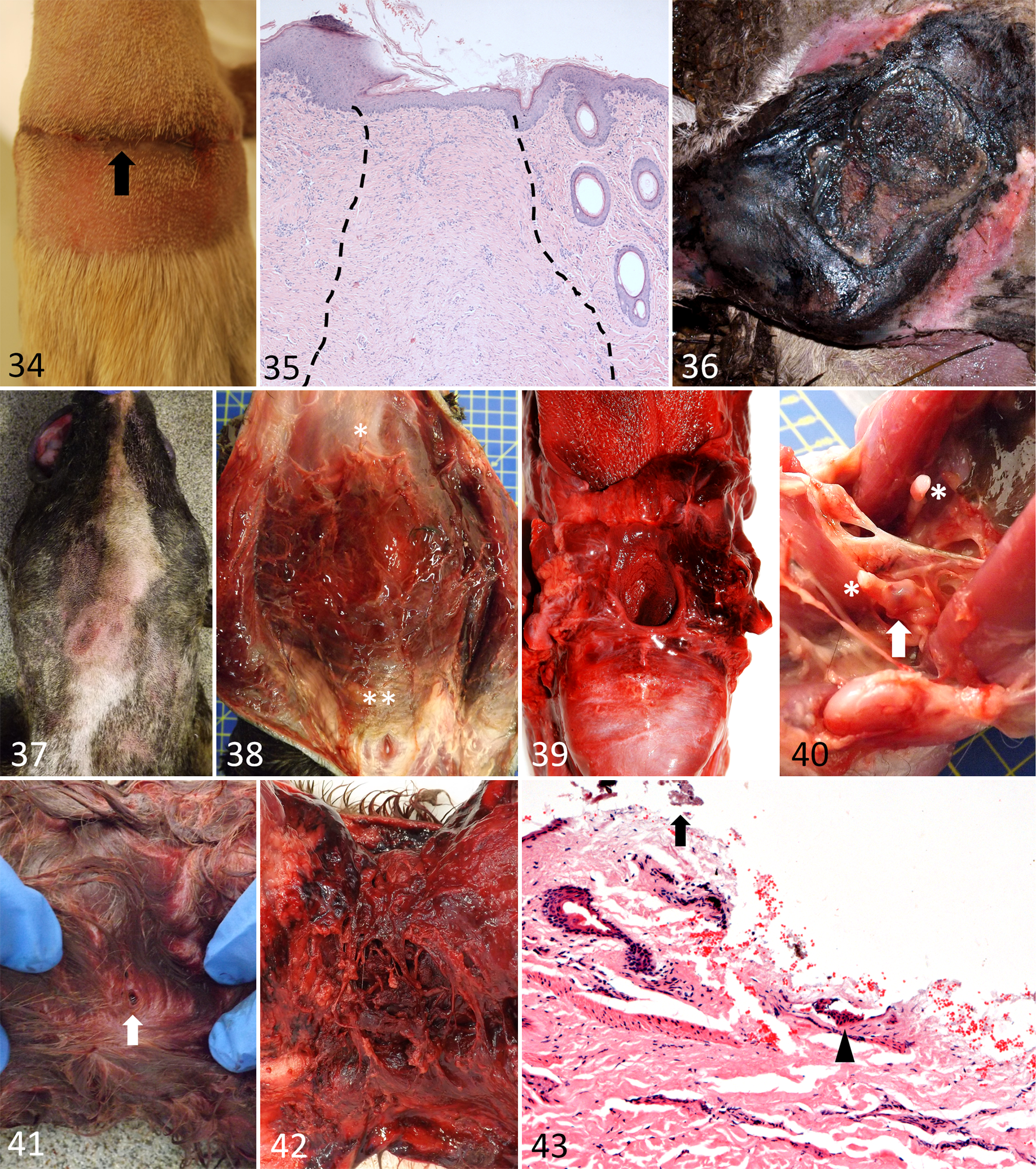
Focal application of a moderately strong force for a prolonged time rarely leads to tearing of or damage to the tissue but instead induces a tissue reaction. Constriction of a body area by string, metal wire, cable tie, or rubber band results in a grossly visible marked circular depression (Fig. 34) due to compression atrophy of the underlying tissue, followed by a chronic epidermal and dermal reaction that is apparent upon histological examination (Fig. 35). Even after long time periods, occasional iron-laden cells can be identified using the Perl’s Prussian blue stain, confirming that hemorrhage had initially been present. We have observed adaptive changes in the underlying bones, such as resorption and new bone formation. If stronger pressure is applied to a large area of the body, time- and force-dependent changes such as focal fibrosis or necrosis can occur as a result of impaired circulation (Fig. 36). As an example, in cases of starvation, when the animal can no longer stand, recumbency can prompt the formation of pressure sores or extensive areas of necrosis mainly over bone prominences.
Special types of blunt trauma.
Compression: Choking and Hanging
Under some conditions, strong pressure applied to large areas for a longer time period than in classical nonaccidental blunt trauma can provoke direct mechanical damage of vessels. Alternatively, progressively increasing venous pressure, as occurs when normal blood flow is impaired, can lead to rupture of vessels and subsequent hemorrhages. An example of the first scenario in veterinary medicine would be manual strangulation of an animal, where the pressure of human fingers elicits a direct traumatic effect on vessels. The second scenario includes both hanging and ligature strangulation. Hanged animals exhibit a combination of morphological features at the location of the ligature that are not always present together, including rupture of hairs (ranging from a circumferential line of hair fragmentation to a partial line of complete epilation), areas of skin abrasion, occasional tenuous superficial bruises apparent upon external examination (Fig. 37), and multifocal to coalescing petechial hemorrhages in the loose subcutaneous tissue (not always corresponding to the external abrasions). In strangulation cases, such pinpoint hemorrhages (Fig. 7) are seen along the margins of the area where the force was applied. With ligature strangulation, the pressure on the neck is intermittent, 25,71 and the progressively increasing venous pressure distally to the ligature point (head) is responsible for the severe edema, congestion, and extravasation of red blood in the soft tissues of the head (Fig. 38) and of the neck (ie, in the region of the larynx; Fig. 39). Histologically, these lesions are characterized by extravasation of erythrocytes deep within the subcutis, with diapedesis of intact erythrocytes into areas with less densely packed mature collagen and around markedly engorged and distended veins. Occasionally, the hyoid bones are fractured. 52 It is therefore important to carefully check the integrity of the hyoid bones for fracture or dislocation in cases of suspected strangulation or hanging; however, the absence of such changes does not exclude strangulation. In animals suffering from chronic abuse and previous attempts at strangulation, we have occasionally observed callus formation of the hyoid bones (Fig. 40).
Dog Bites
In veterinary forensic investigations, lesions caused by bites are frequently seen, either due to natural predation or interanimal aggression. In contrast to the dentition of some of the most common predators, dogs’ teeth have more rounded apices that, combined with a powerful jaw closure, often produce a type of tissue damage compatible with blunt trauma. Moreover, the extensive social interaction among canids and in particular the synanthropic behavior of dogs and humans within confined areas, renders dogs particularly susceptible to behavioral aberration and abuse by humans. This makes animal-to-animal and animal-to-human dog attacks a frequent reason for forensic examinations. 21 In our experience, lesions of dog bites often appear on external examination as small, barely detectable, individual or more often paired, circular impressions or puncture wounds of the superficial skin, with or without grossly visible bruises (Fig. 41). When detected, small superficial lacerations or abrasions of the skin need to be documented by clipping the hair coat and measuring the distance between paired lesions, which can be compared with the dentition of a putative animal perpetrator. Conversely, a dental cast obtained from the examined individual provides a valuable and permanent record of the expected morphological features of bite marks induced by the superior and inferior dental arcades. Moreover, when the identification of an individual biting dog is required (eg, in illegal dog fighting and hunting), DNA swabs of saliva from the margins of bite marks can be used for comparison with samples from suspected dogs. Characteristically, substantial lacerations of the underlying structures are apparent only after complete skinning of the wounded body region (Fig. 42). In our experience, there are body regions that represent common targets for dog bites. When the attacking dog is substantially larger than its victim, the chest and neck are the preferred biting regions. Under these circumstances, death is likely to occur due to a combination of hypovolemic shock (due to exsanguination), neurogenic shock (due to transection of major nerves in the neck), and pneumothorax. In dog fights, or when intraspecies fights for social precedence take place between individuals of comparable strength and size, bites are frequently located on the head, neck, and proximal and distal legs, with multiple lacerations and contusions, occasionally leading to death due to the transection of vital large arteries and veins. Histologically, such lesions are essentially lacerations, often presenting as wedge-shaped discontinuities of the skin with hypereosinophilic collagen bundles and necrotic epithelial cells of both the epidermis and dermal adnexa (Fig. 43). Such a morphological pattern represents the mixed compression/laceration effect of dog bites. Along the irregular margins of the wound, free erythrocytes, foreign material including bacteria (originating from the oral cavity of the perpetrator), and a few fragmented hair shafts are a frequent finding.
Distinction Between Antemortem and Postmortem Blunt Trauma
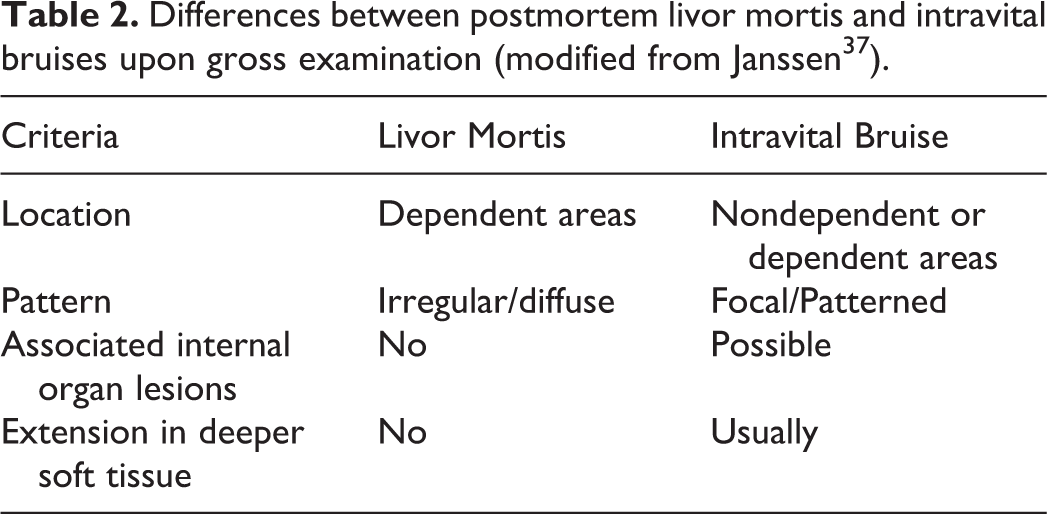
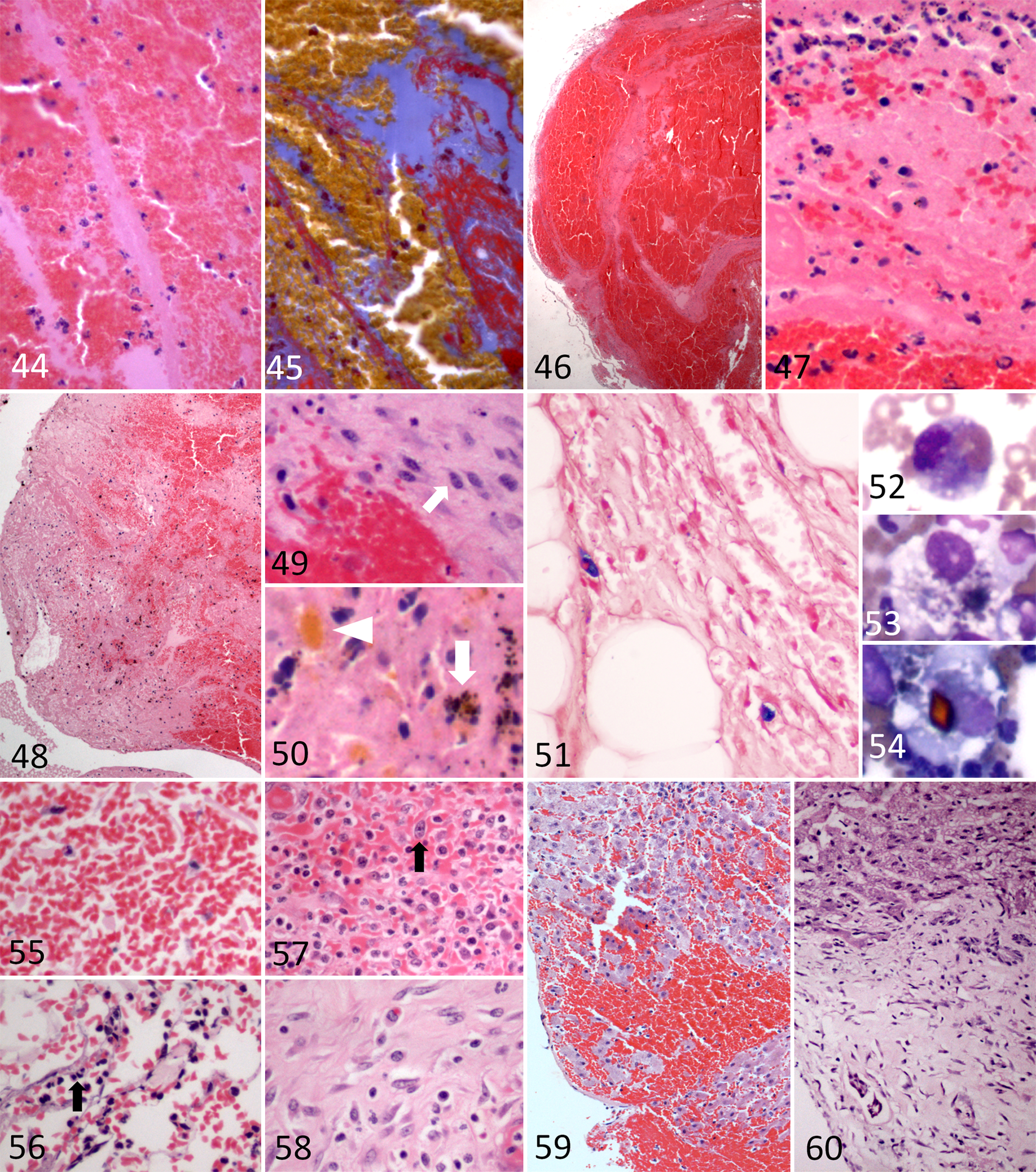
In some forensic cases, the pathologist is asked to determine whether an animal obtained a wound before or after death. A relevant consideration is the differing definitions of death. For lay people and to a large extent also for the law, death is a point in time, defined by the irreversible cessation of brain activity and the spontaneous function of respiratory and circulatory systems. 27 In contrast, clinical death does not occur at a fixed time point but is characterized by the gradual death of individual tissues, which preserve their functions as long as energy (mainly ATP from anerobic glycolysis) is available to accomplish the required biochemical processes. 42 This highlights that there is a gray area between life and death, referred to as the perimortal period. When taking a rigorous forensic approach to this problem, we suggest applying a proposed classification based on 3 categories: (1) definite vital reactions, (2) organ findings that could have occurred at the time of death, and (3) postmortem changes. 37 As a general and safe rule, from a histological point of view, a wound without evidence of an immune reaction or active wound healing, regardless of the presence of fibrin deposition, platelet aggregates, and sparse neutrophils (consistent with those present in circulating blood), should be defined as “wound incurred shortly before or after death.” In contrast, a wound characterized by an active inflammatory or healing reaction, in particular by the invasion of neutrophils, macrophages, and/or fibroblasts, can be defined indisputably as a “vital wound.” 24 Gross and histological examination of skin wounds due to blunt trauma is crucial for the differentiation between antemortem and postmortem injuries. Postmortem abrasions can have many causes, the most common of which is dragging the carcass for transportation purposes. Insect bites, in particular ant bites, are reported in veterinary forensic textbooks as a possible cause of lesions resembling abrasions 50 ; however, we have never observed such lesions. Postmortem abrasions can also be the result of handling the carcass immediately before or after the necropsy. This is important to keep in mind when a second necropsy is requested. Grossly, postmortem abrasions often exhibit a stiff leather-like appearance and orange to brown color, without associated reddening, because of the absence of hyperemia or hemorrhage. Histologically, postmortem abrasions lack vital reactions. However, acute hemorrhage in association with an abrasion should be regarded as a wound that occurred shortly before or after death. 37 Accumulation of neutrophils in the bed of the denuded dermis or surrounding blood vessels at the lesion margins suggests that the lesion occurred during life. In perimortal abrasions, the exuded proteinaceous material can lead to a “leathery” appearance of the denuded dermal surface when the fluid dries off. 39 This often happens when the postmortem interval is prolonged, and it can mimic a postmortem abrasion. Postmortem blunt trauma should in theory not induce bruising because of the lack of blood pressure; however, contusions can still occur for a few hours after death 25 if the body is subjected to trauma. The mechanism is the same as for vital contusions and leads to the rupture of small blood vessels and leakage of blood into the tissue. Contusions must be distinguished from livor mortis (postmortem hypostatic congestion). 50 There are some features that can assist in the differentiation between a bruise and an area of lividity (Table 2). 37 In birds, copious reddening of the calvarium is a postmortem artifact that can easily be misinterpreted as antemortem blunt trauma to the head. 66 Similarly, petechial hemorrhages can develop in the pericardium due to rigor mortis, 33 mimicking intravital hemorrhages. Histologically, livor mortis can be discerned from acute bruising as in the former red blood cells should be confined to blood vessels, at least in the first phases, whereas they have extravasated in the latter. In the late stages of livor mortis, when red blood cells cross the endothelial barrier, acute bruising cannot be distinguished from areas of livor mortis. 37 Indeed, histological findings resembling acute intravital hemorrhages have been observed in human dead bodies within the first hours after death, 55 and a histological comparison of hemorrhages that occurred immediately prior to the death of an animal with those induced not long after death did not reveal any differentiating features. 37 The presence of fibrin within areas of hemorrhage has in the past been considered as an indicator of vital origin. 37 However, several studies have since demonstrated that specific stains for fibrin can yield a negative result in intravital wounds and a positive result in postmortem hemorrhages. 28,51 The presence of a distinct fibrin network, in particular at the periphery of hemorrhages, has been indicated as evidence that the hemorrhage occurred during life. 37 However, because of the lack of objective parameters to assess this particular pattern, its use as forensic evidence is currently not appropriate. Fibrin presents as pale eosinophilic fibrillar material in hematoxylin and eosin–stained sections (Fig. 44) and special stains, such as phosphotungstic acidic hematoxylin or Martius scarlet blue (MSB), should be applied to confirm its identity. We prefer MSB (Fig. 45) because it can distinguish between newly formed fibrin (yellow) and older fibrin (red). 3 After an acute hemorrhage, represented by extravasated red blood cells and multifocal small areas of fibrin network (Fig. 46), leukocytes start to emigrate. The interpretation of vital hemorrhage based on neutrophils requires the presence of large numbers of neutrophils that form aggregates or groups, while small numbers can originate passively from the circulating pool during formation of the hemorrhage. However, it has been suggested that pooling of groups of neutrophils at the margin of a focal hemorrhage (Fig. 47; and in particular in a hematoma) can be the result of a simple redistribution of the blood cells. 37 It should also be stressed that the literature lacks systematic investigations into the magnitude of neutrophil recruitment in different types of wounds, 5 suggesting that the assessment of infiltrating neutrophils is not very useful for determining the lesion age and therefore cannot be applied in forensic cases. In our experience, assessment of vitality based on the presence of neutrophils should be applied carefully and only when there is clear evidence of perivascular extravasation of neutrophils into the tissue immediately adjacent to (but not part of) the hemorrhage. 7 In subsequent phases, within the hemorrhages, the amount of fibrin increases, forming a more intricate and substantial network (Fig. 48). The presence of mononuclear cells and/or fibroblasts 24 (Fig. 49) as well as hemosiderin or hematoidin 37 (Fig. 50) is indisputable evidence of intravital hemorrhage. Postmortem changes can render the determination of the vitality of a bruise challenging, mainly because of the hemolysis of red blood cells and the loss of cellular details in leukocytes. However, in our experience, special stains, such as MSB or Perl’s Prussian blue, are still useful in tissues with moderate postmortem changes (Figs. 45 and 51, respectively). Also, in some circumstances, cytology can yield better morphological details at the single-cell level, allowing identification of erythrophagocytosis (Fig. 52), hemosiderin (Fig. 53), or hematoidin (Fig. 54). A similar approach can be taken for open wounds such as lacerations. Although some authors suggest that neutrophils can be motile for 12 hours after death, 39 experimental studies using animal models have clearly demonstrated that migration of leukocytes from undamaged vessels is impossible from the moment of cardiac arrest, even when the cells maintained their amoeboid motility. 37 In addition, inflammation does not proceed in a dead animal, 13 although one study found that neutrophils migrate for some hours after death when chemotactic substances were applied into the subcutis of rats immediately after death. 1 These findings indicate that perivascular accumulation of a substantial number of neutrophils (3–4 cells in at least 2 different areas 37 or 10 cells in a single area 7 have been suggested) close to the margins of the open wound are evidence that a lesion has developed before death. 62 The concepts described above can be extended to wounds in internal organs. We consider large blood clots attached to the wound margins in association with lacerations of organs such as spleen and liver as a suggestion of an intravital lesion, in particular when they are seen together with a hemoperitoneum. Unfortunately, most forensic cases involve a short time between the lethal blow and the death of the animal when it is not possible to definitively determine whether a lesion occurred antemortem or postmortem. 25 Thus, postmortem examination is just one part of the puzzle that each forensic case represents.
Differences between postmortem livor mortis and intravital bruises upon gross examination (modified from Janssen 37 ).
Indicators of the vitality and timing of lesions of blunt force trauma.
Estimating the Timing of Lesions due to Blunt Trauma
Estimating the timing of wounds is one of the most challenging aspects of a forensic examination, in particular since precise information on the time span between the application of a blunt trauma and the death of the animal is often of primary relevance for the investigation. In veterinary medicine, this task is challenging mainly because reference data are largely missing for domestic species, as the literature on the topic focuses on animal models and humans. 19,20,24,37,44 This pitfall has recently been highlighted, since differences in healing vary greatly even between genetically close species. 9,53,79,80 As an example, it has been shown that healing starts earlier and proceeds faster in laboratory animals than in humans, 37 but quite surprisingly, differences in wound healing have even been found between horses and ponies. 79,80 Different animal species have been used as models of wound healing in humans, and some of the data can be adopted as a reference for the age determination of wounds involving the same species. Nonetheless, the lack of precise data that can be used to support the conclusions is a professional challenge for the veterinary forensic pathologist who faces criminal cases in which the interpretation needs to be made “beyond any reasonable doubt” rather than “on the balance of probabilities.” Thus, data provided in the present review should be used only as a “guide” for the interpretation of results. Despite such caveats, wound healing in mammals is represented by a chronological order of events, 20,42 and the chronological order of different wounds (relative timing) can be established in animals that exhibit more than 1 lesion. This evidence can help to unravel important features of the case, such as the confirmation of repeated assaults on the animal.
Enzymes involved in inflammation and wound healing are characterized by different activity peaks when investigated by biochemical methods. As an example, histamine and serotonin levels peak between 0 and 2 hours after a wound has been produced, while esterases peak between 8 and 48 hours. 5,37 Immunohistochemical expression of fibrinogen, fibronectin, and C5b-9 in wounded tissues of dogs and mice is greater at more than 60 minutes compared with 0 to 30 minutes, 29 while the transcription of cyclooxygenase 2, interleukin-1, and monocyte chemotactic protein–1 peak within the first 24 hours after infliction of experimental wounds in rabbits. 2 These experimental studies need further validation before their results can be applied routinely to forensic practice; however, they represent promising approaches to evaluating the very early phases of wound healing after trauma.
Despite the large number of studies, there is not a general consensus in human forensic pathology on the usefulness of histopathological examinations for wound age determination. While DiMaio and DiMaio 25 are of the opinion that histology cannot provide useful data, other authors consider histology as a useful method to determine the age of wounds. 19,24,37 However, the variable and partly discordant results of the variety of studies on wound healing limits their use as reference data for forensic examinations. 37 It seems that, ironically, human forensic pathologists face a similar problem to their veterinary counterparts, when they have to extrapolate data from animal studies for use as evidence in court. 24,43 In general, it might be more appropriate and effective to ask for information on the suspected time when the wound was inflicted and to convey whether the morphological features are consistent or not consistent, rather than trying to accurately age a wound. 44
Abrasions and Contusions
The gross appearance of abrasions is only vaguely indicative of their timing. 39 Histology, however, is used for the dating of abrasions, based on known chronological processes (Table 3). 67 Although the chronological sequence is similar in domestic animals, there are no studies that have investigated the duration of each phase.
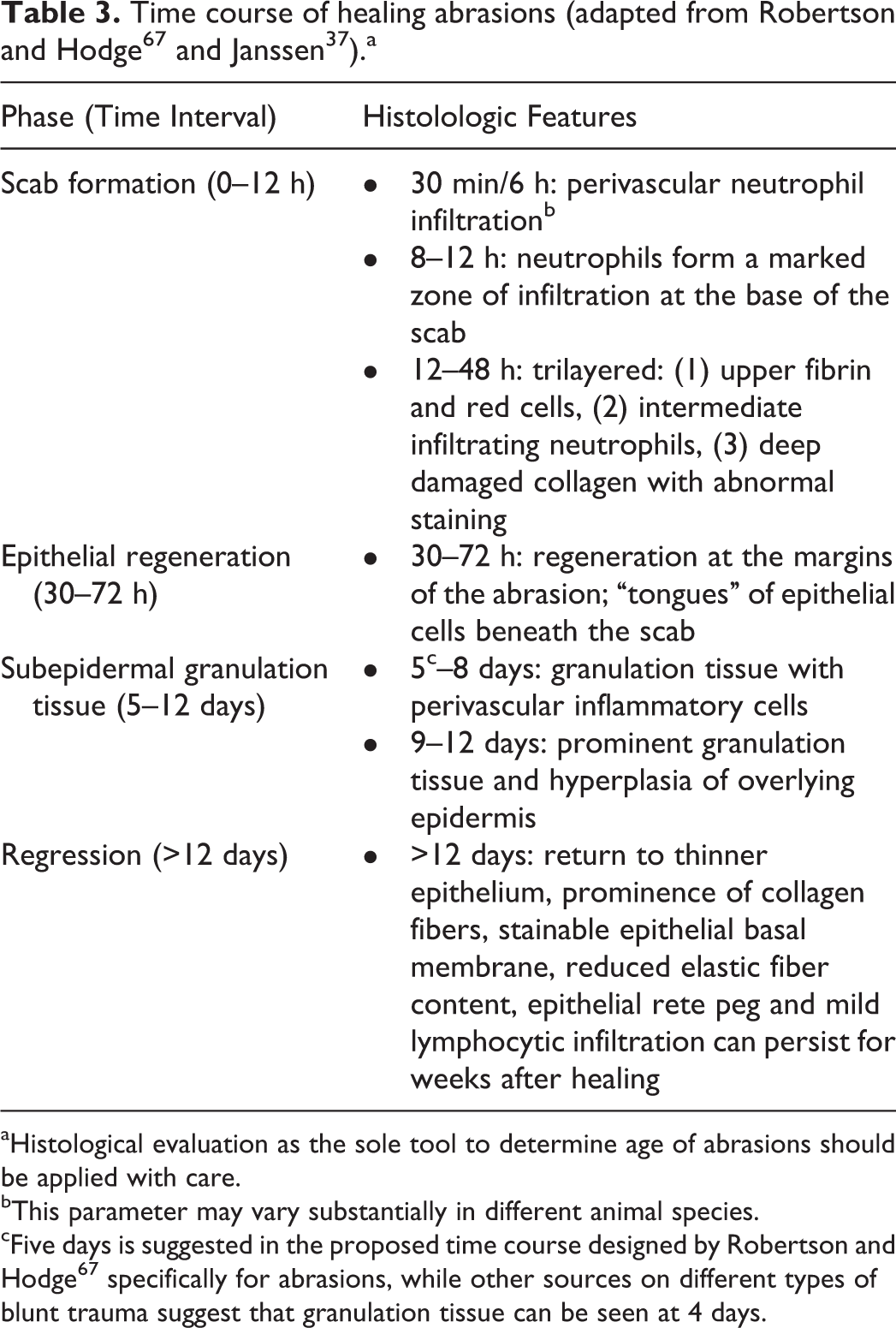
aHistological evaluation as the sole tool to determine age of abrasions should be applied with care.
bThis parameter may vary substantially in different animal species.
cFive days is suggested in the proposed time course designed by Robertson and Hodge 67 specifically for abrasions, while other sources on different types of blunt trauma suggest that granulation tissue can be seen at 4 days.
Contusions of humans are sometimes dated according to their gross features of changes in skin color 45 or by more objective methods such as instrumental analysis. 74,77 However, this approach has been criticized for its unreliability. 26 In domestic animals, with the exception of poultry, 52 similar attempts have so far not been made, and the hair coat of most animals would likely hamper this determination. Histological analysis of the sequential time-related changes in hemorrhages allows the age determination of covered subcutaneous hemorrhages (Table 4), 6 but some aspects must be considered. Experimental studies have investigated the time points when leukocytes first appear in the tissue: in guinea pigs, 37 rats, 37 swine 65 and sheep, 47 neutrophils were detected at 30 minutes, 1 hour 30 minutes, 4 hours 30 minutes, and 8 hours, respectively. However, it should be noted that the named time points were the first time points studied in the different species; from a forensic point of view, this implies only that neutrophils first appeared in tissues during the time span before the examined time point. Nonetheless, these data confirm that inflammatory reactions develop more slowly in humans than in laboratory rodents. 5 The published studies used different time points, study designs, and semiquantitative methods to assess the presence/absence of infiltrating neutrophils, which likely accounts in part for the observed variation. The identification of hemosiderin in the tissues, based on the demonstration of Perl’s Prussian blue–positive material in the cytoplasm of macrophages (Fig. 51), is an important tool for the dating of hemorrhages. The more recent literature states that they appear at 2 to 3 days 37,52 or 4 days 51 after acute hemorrhage. The extent of hemosiderin formation depends on the magnitude of the initial hemorrhage, and the amount of hemosiderin decreases as the wound ages. Moreover, if more recent acute hemorrhage occurred at the same site, hemosiderin again forms after 2 to 4 days. 24 Slight or absent hemosiderin deposits cannot provide information on the time of wound infliction. 77 Erythrophagia precedes formation of hemosiderin within a contusion; however, only scarce information is available regarding the time when erythrophages first appear (Fig. 52); one report describes their appearance in hemorrhagic lungs within 30 minutes, 59 likely due to the constant presence of alveolar macrophages, while they have been shown to first appear in the skin within 15 hours. 77 Hematoidin is the final hemoglobin breakdown product (Figs. 50 and 54) and can be detected in animal tissues after 7 to 11 days. 31,78 Few studies have specifically been performed in domestic animal species: in calves and lambs, a 3-time-point evaluation system was established for subcutaneous bruises: (1) only neutrophils (8 hours); (2) equal number of neutrophils and macrophages (24 hours); (3) macrophages, spindle cells, and newly formed capillaries (48 hours). 47 In a more rigorous but less routinely applicable study on bruises in sheep, a 2-step grading system was applied: (1) (1–20 hours) characterized by a high probability of observing endothelial cell hypertrophy and a low probability of observing neutrophils; (2) (24–72 hours) with an increasing probability of observing neutrophilic exudation, macrophages, and initial fibrosis. 75 The age of an animal can affect wound healing, 34 and this can affect the relevance of experimental findings. For example, 2 recent ruminant studies used juvenile animals, which could lead to misinterpretation of findings in older animals, in which healing is known to proceed more slowly. 37
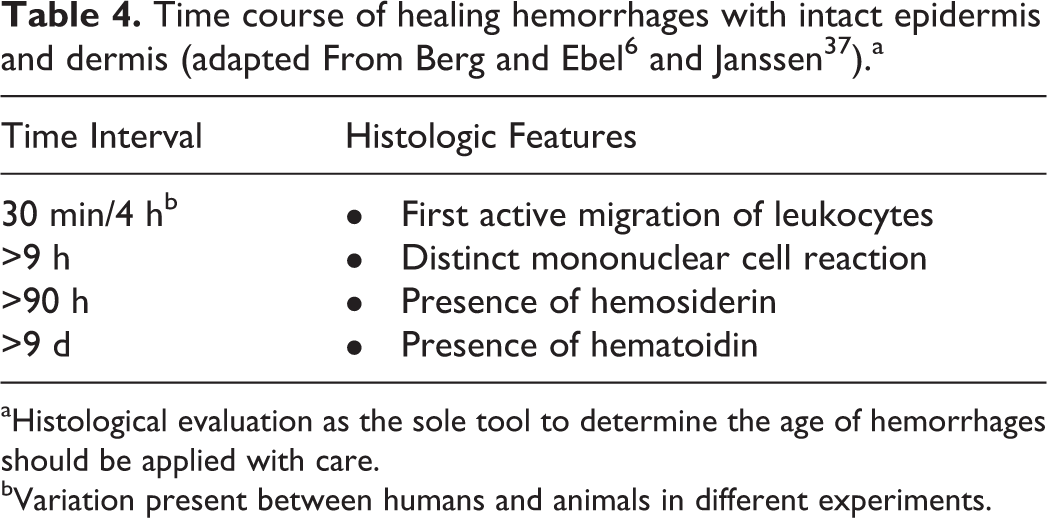
aHistological evaluation as the sole tool to determine the age of hemorrhages should be applied with care.
bVariation present between humans and animals in different experiments.
Lacerations
Lacerations are open wounds; hence, they are expected to undergo healing by secondary intention. 42 In human forensics, histopathological determination of wound healing is guided by a large amount of partially discordant research data. 20,44 Moreover, experimental studies intrinsically lack all the contributing factors and concurrent conditions found in forensics cases that can affect the course of open wound healing; these are described below. For these reasons, histological evaluation as the sole tool to determine the age of open wounds should be applied with care. The studies of Raekallio 62 –64 on the healing of open wounds in adult humans and lab animals characterize different functional areas in the wound: a “central zone” extending from the wound edge up to 500-μm deep into the tissue is characterized mainly by necrotic changes. Surrounding this, there is a 100- to 200-μm-wide “peripheral zone” with the cellular infiltration of the healing process. In this area, neutrophils predominate over macrophages (approximate neutrophil/macrophage ratio of 4:1) at 12 to 16 hours, whereas at 16 to 24 hours, the ratio changes in favor of the macrophages (neutrophil/macrophage ratio of 1:2.5). Such studies 37,63,64 led to the development of a scheme for the histological assessment of open wounds 24,77 (Table 5). Consecutive phases of wound healing are histologically evident as an early phase of acute hemorrhage (Fig. 55) followed by an increase in extravasated and extravasating neutrophils (Fig. 56), leading to an increase in infiltrating mononuclear cells and a decrease in neutrophils (Fig. 57), followed by fibroblast proliferation and a reduction in numbers of infiltrating inflammatory cells (Fig. 58). Starting from approximately day 4, newly produced collagen fibers increase in both number and size for several weeks after the scar formation has begun. 69 A few studies in domestic animals have been performed. A chronological scheme is proposed for healing wounds after the application of ear tags in cattle and buffalo, 53,69 but this system it is of limited general use since it examines only 1 specific anatomical structure and inflicting object. Similarly, a recent study on open wounds in pigs does not provide data that can be applied easily in forensic practice, since the studied parameters are based on knowledge of the initial size of the wound. 81
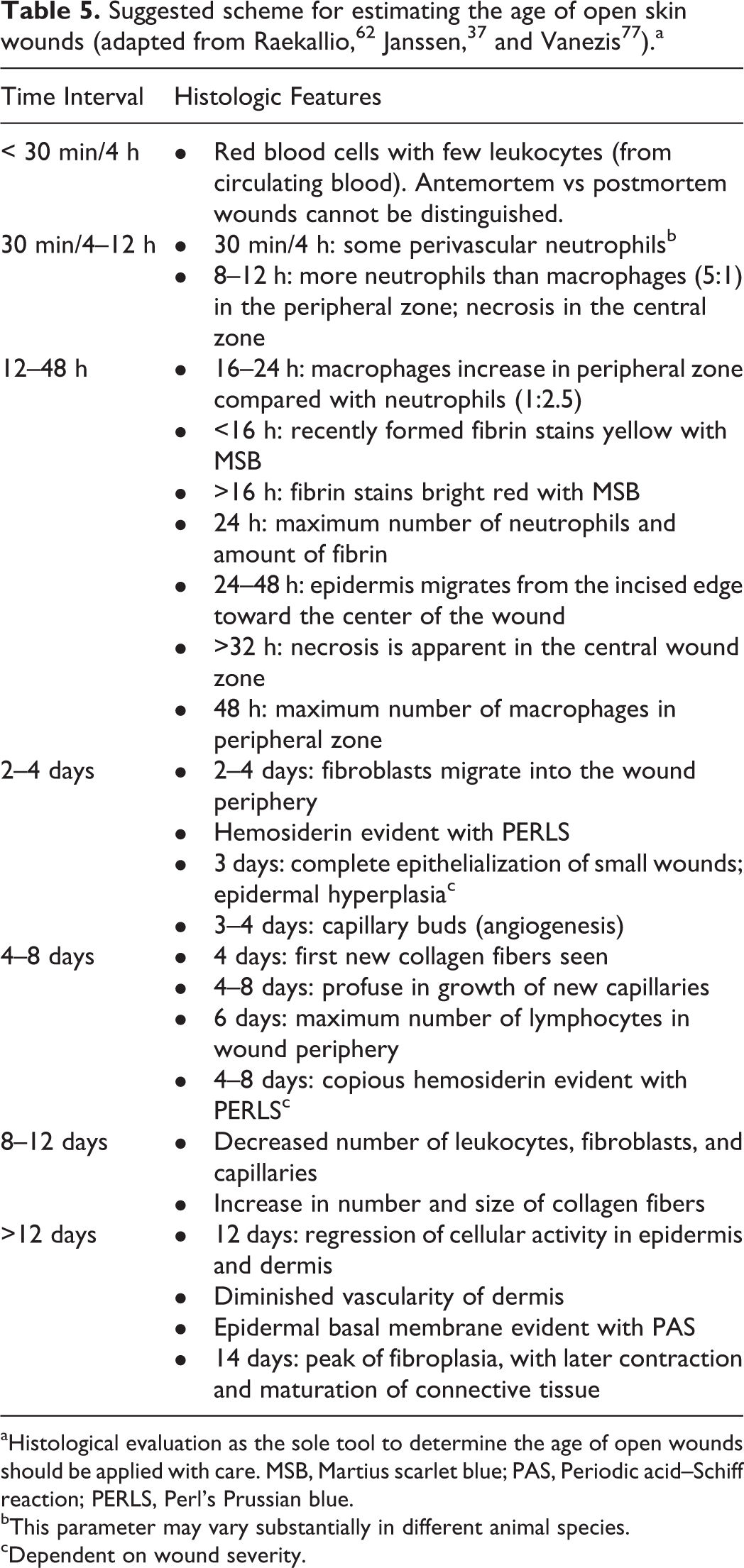
aHistological evaluation as the sole tool to determine the age of open wounds should be applied with care. MSB, Martius scarlet blue; PAS, Periodic acid–Schiff reaction; PERLS, Perl’s Prussian blue.
bThis parameter may vary substantially in different animal species.
cDependent on wound severity.
Open wounds exhibit age-dependent differences in the speed of healing, with delayed epithelialization and development of granulation tissue in older animals. 73 When dating a wound, additional factors, such as the inhibitory effect of iatrogenic or morbid conditions that affect the animal need be considered. Factors that inhibit wound healing in humans include irradiation, corticosteroids, scurvy, diabetes, hepatic cirrhosis, uremia, denervation of the wounded area, loss of blood, cold, cerebral concussion, shock, and any general debilitating condition. 5 In veterinary medicine, common factors that affect wound healing are infection, malnutrition, tissue ischemia, hypoproteinemia, leukopenia, drug administration, and repeated episodes of trauma. Therefore, a thorough and complete postmortem examination should always be performed, and the clinical history should be disclosed and considered.
Blunt Trauma to Bone and Muscle
Studies on subcutaneous bruises often include also bruises in superficial muscles, and the data for the timing of the latter can be extrapolated from those results. When the blunt trauma causes muscle damage in addition to hemorrhage, muscle regeneration and repair follow in a chronological order of events. 76 This can serve as a guide: (1) appearance of macrophages (12 hours), (3) myotube formation and contact with the closest viable segment of the original fiber (10–14 days), (3) presence of centralized nuclei in myofibers (7–21 days). A similar time course is available for healing fractures 15 : (1) grossly unstable fracture with hematoma only (0–24 hours), (2) unstable fracture with histological evidence of undifferentiated mesenchymal cells and neovascularization (24–48 hours), (3) unstable fracture with earliest evidence of woven bone (36 hours), (4) stable fracture with evidence of primary callus of bone and hyaline cartilage (4–6 weeks), (5) stable fracture with evidence of woven bone progressing to lamellar bone (months–years). These guidelines, for which the original evidence is not always available, are intended for a general assessment. A precise time estimation of an unfixed fracture can be more challenging than expected, since mechanical factors profoundly affect the repair of the bone, 17 and great differences exist between different animal models even when the same model is used in different species. 58 In our experience, histological examination of all the fractures can be very useful, in particular when it identifies fractures in different healing stages, as these are commonly found in cases of abuse, while they are not seen in animals hit by motor vehicles. 52
Blunt Trauma to Internal Organs
With the exception of brain injuries, information on the timing of lesions in internal organs is scarce. When a skin injury is found that corresponds to an internal wound, the determination of the age of the former can serve to establish the time course of the internal blunt trauma. Several studies have been performed in humans that provide data on the age of subarachnoid and subdural hemorrhages and cerebral contusions. 19,36,46,48,61 In contrast, there are to our knowledge no studies on the timing of brain injuries in domestic animals, and only fragmentary information is available on time-related histological changes in the brain of domestic animals after injury. For detailed information on timing of neuropathology of trauma, the reader is referred to the review in this journal issue on traumatic brain injury. 30
The liver is one of the most commonly injured organs in the abdominal cavity, and it would be useful to know the timing of liver lesions that occur without obvious changes in the skin or the thoracic/abdominal wall. Acute liver ruptures are characterized, not surprisingly, by extravasated red blood cells (Fig. 59). An increased number of leukocytes in the liver seems not to be suitable for age determination of liver wounds in guinea pigs, 38 whereas proliferation of mesenchymal cells (Fig. 60) is not expected before 24 hours postinjury. 37
Conclusions
Lesions due to blunt force trauma are commonly encountered in forensic veterinary pathology practice. Lesions in domestic animals are comparable (even if not identical) to those described in human forensic pathology, and accurate information can be gathered from the macroscopic and microscopic examination of blunt trauma in animals, in order to understand its mechanics and provide evidence to the court. At the time of the present review, literature on wound aging in domestic animals is still scarce. Understanding species differences in wound healing is crucial for a scientific evidence-based approach to the determination of wound age and the vitality of lesions.
Footnotes
Acknowledgements
We thank Professor Anja Kipar and Dr Alexandra Malbon, Institute of Veterinary Pathology, Vetsuisse Faculty, University of Zurich, for the critical revision and editing of the manuscript. We are grateful to Dr Sean Taylor, Lockgate Animal Forensics Ltd, for kindly providing Figure 34; Dr Ranieri Verin, Veterinary Pathology, School of Veterinary Science, University of Liverpool, for providing Figures 17 and 18; and Dr Martina Piviani, School of Veterinary Science, University of Liverpool, for kindly provifing the specimen of Figure 54.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.