
Abstract
Skeletal lesions in the articular processes of cervical vertebrae C2 to C7 were compared between Thoroughbred horses with cervical stenotic myelopathy (17 males, 2 females; age, 6–50 months) and controls (6 males, 3 females; age, 9–67 months). Lesions identified by magnetic resonance imaging occurred with an increased frequency and severity in diseased horses and were not limited to sites of spinal cord compression. Lesions involved both the articular cartilage and trabecular bone and were further characterized using micro–computed tomography and histopathology. The most common histologic lesions included osteochondrosis, osseous cyst–like structures, fibrous tissue replacement of trabecular bone, retained cartilage matrix spicules, and osteosclerosis. Osseous cyst–like structures were interpreted to be true bone cysts given they were a closed cavity with a cellular lining that separated the cyst from surrounding bone. This is the first report of bone cysts in the cervical articular processes of horses with cervical stenotic myelopathy. The morphology and distribution of the lesions provide additional support for the previously proposed pathogenesis that developmental abnormalities with likely secondary biomechanical influences on the cervical spine contribute to equine cervical stenotic myelopathy.
Keywords
Equine cervical stenotic myelopathy (CSM) is a multifactorial disease of the musculoskeletal system that presents clinically with proprioceptive neurologic deficits that are more severe in the pelvic limbs. The disease is characterized by malformations of one or more cervical vertebrae that lead to stenosis of the spinal canal, spinal cord compression, and damage to spinal cord nerve tracts. Proposed etiologic factors include high planes of nutrition, accelerated growth rates, altered ratios of copper and zinc, and inherited genetic determinants. While much is known regarding signalment and clinical diagnosis, the pathogenesis of CSM remains unclear and likely encompasses multiple pathways that result in similar clinical presentations. 17 Over the years, 2 theories have been proposed based on multiple studies. The developmental theory proposes an underlying disorder of bone and cartilage morphogenesis and maturation that leads to cervical vertebral malformations. 13,24 The biomechanical theory, in contrast, proposes a process whereby abnormal mechanical stresses and forces on the cervical column result in structural vertebral changes, leading to stenosis of the canal. 21,26
Prior studies have reported aberrations in vertebral development associated with CSM. A comprehensive examination of lesions suggested abnormal bone and cartilage maturation manifested as osteosclerosis and osteochondrosis. 13 Interestingly, lesions were also observed in the costochondral junction of the ribs supportive of a possible systemic abnormality of bone and cartilage maturation. Further work examined the frequency and severity of osteochondrosis in the articular processes with comparison to the appendicular skeleton and found an increased severity of osteochondrosis lesions in both the axial and appendicular skeleton of CSM horses. 24 It has also been suggested that cervical malformations begin to develop in utero. 12
Conversely, there is support for a model of pathogenesis whereby abnormal biomechanical forces lead to vertebral malformations and canal stenosis. Maturation of equine vertebrae continues until approximately 5 years of age, at which point the vertebral body growth plates close. 28 During this time and even following growth cessation, vertebrae are responsive to biomechanical forces on the neck through Wolff’s law and related variables of mechanical regulation. 4,29 Mechanical variables in the form of strain, oscillation, and vibrations have been demonstrated to affect bone morphology. 9 Lesions consistent with abnormal forces on the neck include degenerative changes of the articular processes, thickening of the dorsal lamina, and hypertrophy of the ligamentum flavum. 21,26
A major knowledge gap in regard to CSM pathogenesis is the mechanism by which these skeletal lesions develop and progress to clinically significant spinal canal stenosis. Rapid development of imaging technologies has allowed for examination of the cervical column in situ for lesions associated with CSM. The present study focused on an assessment of cartilage and bone lesions observed by MRI in the articular processes of CSM horses compared with controls, given that changes in their shape, size, and spatial orientation frequently contribute to spinal cord compression. 6,14 A subset of representative lesions was then further characterized with micro–computed tomography (micro-CT) and routine histopathology. The hypothesis was that bone and cartilage lesions of the cervical vertebral articular processes occur with an increased frequency and severity in CSM horses compared with controls. A better understanding of the distribution and types of lesions that occur within the articular processes will likely lead to greater insight into the etiopathogenesis of CSM in the horse.
Materials and Methods
Magnetic Resonance Imaging
Horses used in the study were identified based on clinical history, neurological assessment, cervical radiographs, and postmortem examination (Suppl. Table S1). Nineteen Thoroughbred horses with CSM (17 males, 2 female; age range 6–50 months with a mean of 18.1 months) were compared with 9 control Thoroughbred horses (6 males, 3 females; age range 9–67 months with a mean of 12.4 months). Case and control horses were identified in collaboration with local veterinary practitioners. All procedures were conducted in accordance and approved by the University of Kentucky institutional animal care and use committee.
A single assessor performed a neurologic examination on each horse. A grading scale of 0 to 5, where 0 indicated no neurologic deficits and 5 indicated recumbency, was used to classify the severity of clinical signs in the forelimbs and hindlimbs. Standing lateral cervical radiographs were obtained from all horses. Radiographic images were measured and evaluated by a single assessor. Standard minimal sagittal diameter (MSD) intravertebral ratios and intervertebral ratios were calculated from C2 to C7 using Dicom Viewer software (eFilm Workstation; Merge eMed, Chicago, IL). 7,15 After antemortem clinical examination and radiographs, owner-elected euthanasia was performed with an overdose of a barbiturate following American Veterinary Medical Association (AVMA) guidelines. Control horses had normal neurological function but were euthanized for other health-related reasons.
Within 4 hours of euthanasia, the cervical spinal column was disarticulated from the horse but kept intact from C1 to the area of T3 to T5. Loss of cerebral spinal fluid was prevented by placing putty in the vertebral canal at the disarticulation site. Magnetic resonance imaging (MRI) was performed using a 1.5 Tesla magnet with a flexible surface receiver coil and spinal coil. The cervical column was imaged in the neutral position in cranial (C2–C5) and caudal (C4–C7) sections as described previously. 8 Sagittal, transverse, and dorsal plane images using multiple sequences were acquired for each section (Suppl. Table S2).
Localization of Compressive Spinal Cord Lesions
The spinal cord was removed from the vertebral column during disarticulation of intact vertebrae. Intervertebral sites on the spinal cord were identified and labeled during disarticulation. The spinal cord was placed in 10% neutral buffered formalin for fixation and processed routinely for histologic examination. Two to 4 tissue sections were evaluated at each intervertebral site from C1–C2 to C6–C7. Cervical stenotic myelopathy was confirmed by identifying compressive lesions microscopically in the spinal cord at specific intervertebral sites based on the characteristic changes of Wallerian degeneration with the presence of gitter cells, dilated myelin sheaths, spheroids (swollen axons), and fibrosis in appropriate dorsal, lateral, and ventral funiculi within the white matter. 25 Postmortem and histologic examinations were also used to rule out other infectious, inflammatory, or degenerative neurologic diseases of the spinal cord.
An open source DICOM viewer program (Osirix, Geneva, Switzerland) was used to visualize MRI studies. 22 Variations from expected MRI signal intensity were identified as prospective lesions and classified as either superficial or deep based on anatomic location. Superficial lesions involved the articular cartilage and/or subchondral bone with possible extension into the trabecular bone. Lesions within an articular process that did not involve the articular cartilage or subchondral bone were defined as deep. Lesions were then assigned a grade of 0 to 3 based on a scale adapted from previous work (Suppl. Table S3). 23 Lesions were required to be present on a minimum of 2 of the 3 MRI studies (proton density fat saturation, T2 weighted, short tau inversion recovery). A consensus grade was assigned from 2 assessors.
Structural Analyses of Articular Process Lesions
A subset of samples from the above-described sample set was selected for structural analyses. Four separate articular processes with deep lesions and 4 additional separate articular processes with superficial lesions were chosen from individual CSM horses (1 articular process per horse for a particular lesion). Articular processes from control horses with an absence of lesions on MRI were identified to match as closely as possible for anatomical site, sex, and age of the CSM horses (Suppl. Table S4). No horse was repeated within or across groups (superficial or deep groups). Articular process sites varied between groups. Articular processes at intervertebral locations both at and distant from the site of spinal cord compression were included.
For micro-CT image acquisition and visualization, articular processes were removed from the vertebrae and placed in a radiolucent acrylic holder for scanning. A custom micro-CT scanner (150/225 Ffi-HR-CT; BIR, Lincolnshire, IL) with a 225-kV X-ray source, 5-μm focal spot, and image intensifier with a 1024 × 1024–pixel digital camera was used. X-ray power settings were 135 KeV and 0.059 mA with a distance of 703 mm from the X-ray source to the image detector. 27 Both the X-ray source and image detector were fixed while the sample was rotated and translated in the z-axis between them. The source to object distance was 177.5 mm. Scanning was performed using a 360 degree-plus-fan-angle-algorithm in the offset mode with the center of rotation of the sample placed 15 mm lateral to the central axis of the X-ray beam. A total of 107 slices were captured per revolution, with each slice representing a thickness of 30 μm. The final reconstruction of each slice resulted in image arrays of 2048 × 2048 × 30 μm pixels. The resulting image stacks contained 30-μm voxels with a 16-bit gray scale (65 356 gray levels).
Image stacks were imported into VGStudio Max for construction of 3-dimensional (3D) models of the articular processes (v1.2.1; Volume Graphics, Heidelberg, Germany). Regions of interest were identified based on localization from MRI data demonstrating the lesions for imaging purposes. Threshold parameters were set for detection of bone. The cranial- or caudal-most point of the articular margin was identified on MRI and used as the starting point for measurements to localize the lesion.
To determine trabecular bone volume, image stacks containing 200 slices were imported into ImageJ (National Institutes of Health, Bethesda, MD) at 25% of the total image size to reduce computational memory requirements. 1 Volumetric coordinates were determined for each image stack, and trabecular bone morphometric quality assessment was performed using a custom bone volume analysis program in MATLAB (v7.1; The Mathworks, Natick, MA). Trabecular bone volume (BV) was calculated as percentage of total volume (TV) of the articular process and reported as bone volume fraction (BV/TV).
Histologic Assessment of Articular Process Lesions
A representative subset of articular process lesions identified on MRI from both CSM and control horses was assessed histologically for descriptive purposes in 3 classifications: superficial, deep, and mixed. The superficial and deep classifications have been described previously. The mixed classification included sites that contained separate superficial and deep lesions within the same articular process. The breakdown of the selected articular process sites histologically evaluated in each classification was as follows: superficial lesions, CSM (n = 9) and controls (n = 3); deep lesions, CSM (n = 7) and controls (n = 2); and mixed, CSM (n = 4). No mixed lesions were identified in control horses. No horses were repeated within a classification, although in some cases, independent lesions from the same horse were used across classifications.
Samples were processed by excising transverse sections from the regions of interest using a scroll saw based on MRI localization and measurements. Resulting sections from the articular processes were decalcified using Decalcifier Rapid S (Labsco, Louisville, KY), embedded in paraffin, and 5-um sections were processed routinely for hematoxylin and eosin staining.
A subset of sections was further characterized using immunohistochemistry. The peroxidase-based method was applied using primary antibodies directed against vimentin (Dako, Carpinteria, CA) and cytokeratin AE1/AE3 (Fisher Scientific, Waltham, MA) using a DakoCytomation Autostainer (Dako) on formalin-fixed, embedded, 5-μm sections. The cytokeratin AE1/AE3 sections were pretreated with proteinase K at room temperature for 5 minutes for antigen retrieval. The positive control tissue for cytokeratin was equine small intestine. The positive control tissue for vimentin was equine lymph node.
Statistical Analyses
A generalized linear statistical model was used to determine if there were significant differences in the frequency of articular process lesions, defined as the number of lesions per articular process across the cervical column identified by MRI, between CSM and control groups. In this model, lesion count was regressed on group using the Poisson regression (SAS 9.3; SAS Institute, Cary, NC). For assessment of severity, a generalized linear equation was also employed. A multinomial model was used to account for the grading scale of 0 to 3. Significance was defined as P < .05.
A generalized linear model was used to determine if there were significant differences in trabecular bone volume fraction of the articular processes from CSM horses with deep lesions compared with controls, CSM horses with superficial lesions compared with controls, and then a combination of the deep and superficial groups compared with controls (SAS 9.3). Significance was defined as P < .05.
Results
MRI Lesion Frequency Analysis
Significant increases of lesion frequency, approximating a 2- to 3-fold change, were identified in CSM horses (P < .05) for comparisons using all lesions at all sites, all superficial lesions at all sites, all deep lesions at all sites, and deep lesions at noncompression sites (Table 1). Within the group of CSM horses, there were individuals with compression and others without compression at each vertebral site. Therefore, the corresponding control data set used for comparison was the same for all comparisons.
Frequency Analysis of Articular Process Lesions Identified on MRI From C2 to C7 in CSM and Control Horses.a
CSM, cervical stenotic myelopathy; MRI, magnetic resonance imaging.
aFrequency is defined as the number of lesions per articular process across the cervical column; data are presented as the mean ± SEM. *P < .05.
bWithin the group of CSM horses, there were individuals with compression and others without compression at each vertebral site. Therefore, the corresponding control data set used for comparison was the same for all comparisons.
cThis classification includes articular processes not involved at the histologic site(s) of spinal cord compression.
MRI Lesion Severity Analysis
In addition to the number of articular process lesions, severity of the lesions was assessed between CSM and control horses. The same categories of anatomic location of the lesion within the articular process, as well as location in the cervical column with respect to cord compression, were analyzed. A significant increase in the relative amount of more severe lesions was observed in CSM horses for all categories (P < .05), except for superficial lesions at noncompression sites (Suppl. Figs. S1–S9).
Microarchitectural and Trabecular Bone Volume Assessment
A subset of grade 2 and grade 3 lesions identified on MRI was imaged using micro-CT for assessment of trabecular bone volume fraction and to evaluate trabecular bone architecture. No significant differences in trabecular bone volume were found (P > .05) when comparing the articular processes with superficial lesions to controls, articular processes with deep lesions to controls, or combination of the 2 groups (Table 2).
Comparison of Trabecular Bone Volume Fractions of Articular Processes.a
CSM, cervical stenotic myelopathy.
aThe data show the percentage of total volume occupied by trabecular bone in the articular process based on micro–computed tomography (CT) analyses. Trabecular bone volume fraction data are presented as the mean ± the standard error.
An absence of bone was observed for superficial lesions in the 4 articular processes examined. In contrast, perilesional regions frequently exhibited trabecular thickening consistent with areas of bone sclerosis (Figs. 1, 2). Analyses of deep lesions on micro-CT demonstrated that they were not composed of bone and are interpreted as osseous cyst–like lesions or fibrous tissue replacement of bone (Figs. 3, 4). This finding was observed in all 4 articular processes analyzed in the deep lesion group.
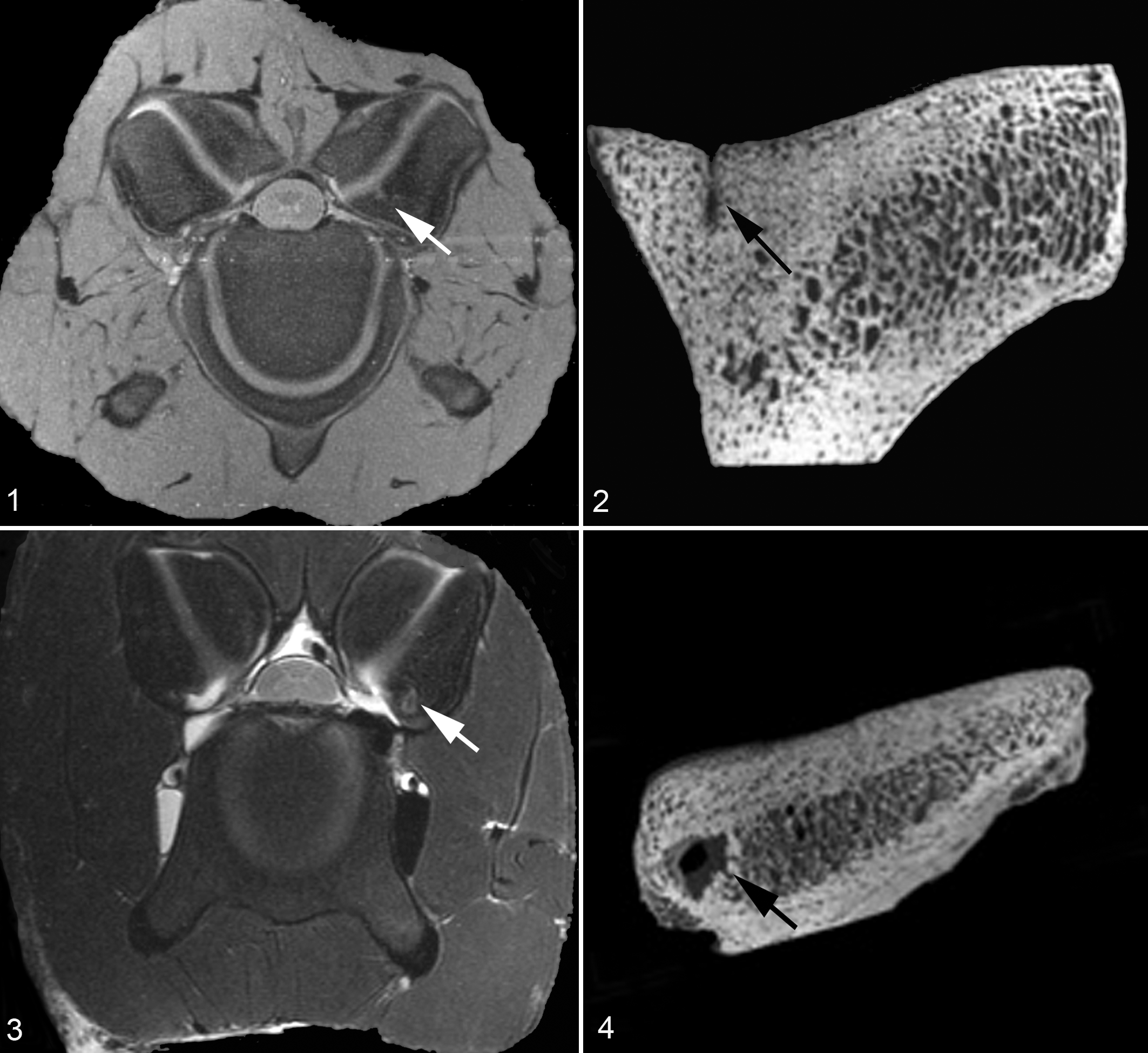
Bone sclerosis, left cranial articular process C4; equine No. 15, cervical stenotic myelopathy (CSM).
Histologic Assessment
A summary of the histologic lesions affecting articular processes is provided in Table 3. All superficial-only lesions (12/12) identified in CSM and control horses were consistent with varying degrees of osteochondrosis. Both osteochondrosis manifesta (OM) and osteochondrosis dissecans (OCD) were observed (Figs. 5–11). Since the lesion grading categories were based on size, both OM and OCD were seen in grade 2 and grade 3 categories. Associated with the cartilaginous defects was a moderate to severe thickening and remodeling of the subchondral bone, which extended variably into the trabecular bone of the articular process.
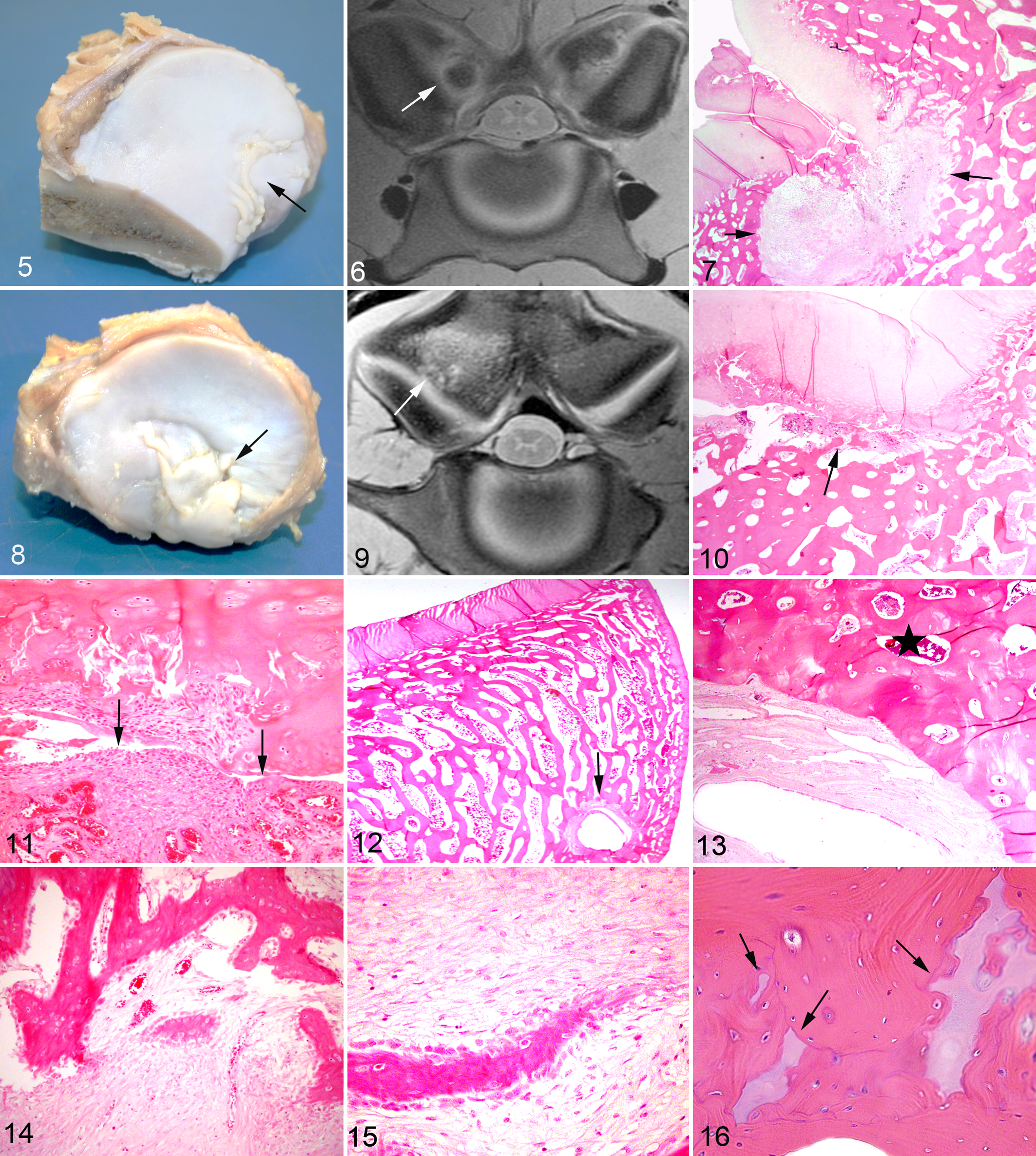
Osteochondrosis manifesta, left caudal articular process C6; equine No. 12, cervical stenotic myelopathy (CSM).
Lesions Observed on Histopathologic Examination of Articular Processes Selected From Magnetic Resonance Imaging.a
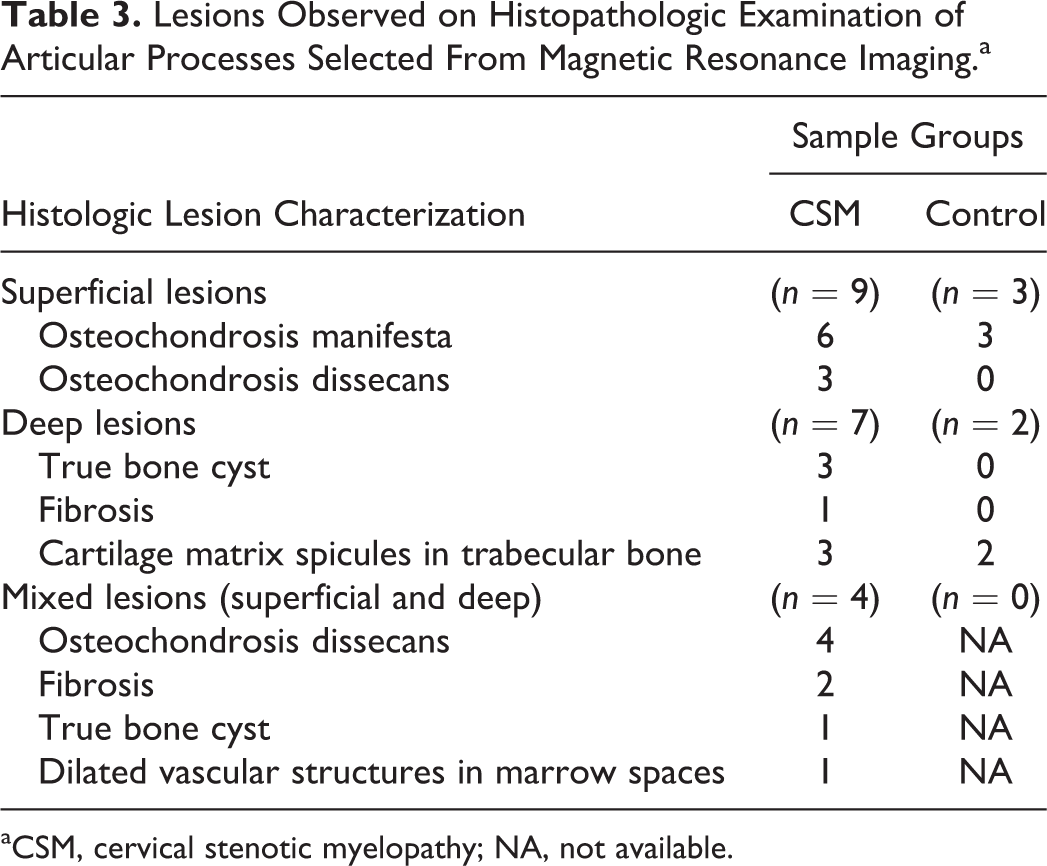
aCSM, cervical stenotic myelopathy; NA, not available.
Deep-only lesions in CSM horses were composed of cyst-like structures within the trabecular bone (3/7) (Figs. 12, 13), fibrous tissue replacement of trabecular bone (1/7) (Figs. 14, 15), and retention of variably sized foci of cartilaginous matrix within trabeculae (3/7) (Fig. 16). Thickened trabecular bone (osteosclerosis) was often observed adjacent to the cyst-like structures (Fig. 13). The cyst-like structures were interpreted as true bone cysts due to being lined by layered polygonal cells and surrounded by organized fibrous connective tissue (Suppl. Fig. S10). The cells that lined cyst lumens were negative for cytokeratin in all 4 cases (0/4). In contrast, the cells were moderately diffusely positive for vimentin (4/4) (Suppl. Fig. S11a,b). The 2 deep lesions identified in control horses were both composed of small to moderate amounts of cartilaginous matrix surrounded by trabecular bone. No cysts in the articular processes of control horses were observed.
Mixed lesions had features of both the superficial and deep classifications. Consistent with the superficial-only lesions, the superficial component of the mixed lesions fell under the spectrum of osteochondrosis. The deep lesions away from the articular surface were composed of areas of fibrous replacement of trabecular bone with active bone remodeling (2/4) (Figs. 14, 15), true bone cysts (1/4), and groups of dilated vascular structures interpreted as veins (1/4).
Discussion
The objective of these experiments was to evaluate and compare the frequency and severity of skeletal lesions in articular processes of cervical vertebrae identified by MRI between CSM and control horses. A representative subset of the lesions was further characterized using micro-CT and histopathology. Lesion frequency, location, and severity were assessed within the cervical column as a whole, at the site of cord compression, and away from the site of compression. While lesions were observed in both control and CSM horses, frequency was significantly increased in the CSM group. Lesion frequency was higher in the CSM horses across the entire cervical column for both superficial and deep lesions, as well as for deep lesions at noncompression sites. In addition, identified lesions had an increased severity in the CSM horses. These data support previous work that concluded abnormalities in the neck of CSM horses are generalized and not limited to the site of compression. 24
A variety of histologic lesions of the articular processes were observed. All of the superficial lesions identified on MRI that were evaluated using histopathology fell under the continuum of osteochondrosis (OC). OC is a developmental disease that results from localized failure of endochondral ossification. Recently, efforts to improve nomenclature for OC have resulted in 3 categorizations: osteochondrosis latens, osteochondrosis manifesta, and osteochondrosis dissecans (OCD). 31 Osteochondrosis latens is a focal area of cartilage necrosis within the epiphyseal cartilage. When cartilage necrosis extends into the adjacent subchondral bone, it is classified as osteochondrosis manifesta. The most severe manifestation, osteochondrosis dissecans, occurs when the integrity between the cartilage and bone is lost, resulting in formation of a cartilage flap or loose body. Osteochondrosis manifesta lesions were observed in control and CSM horses, whereas OCD was seen only in CSM horses. The presence of OCD in CSM horses is consistent with the observation of more severe lesions associated with CSM pathology. On micro-CT, the 4 superficial lesions (confirmed as either osteochondrosis manifesta or osteochondrosis dissecans on histology) evaluated had loss of bone structure consistent with the retention of cartilage through failure of endochondral ossification. Osteochondrosis in the cervical column of CSM horses has been reported previously. 13,24 Findings in this study further substantiate the association of OC with CSM. It is important, however, to distinguish osteochondrosis from complex invaginations of articular epiphyseal cartilage; the latter lack foci of necrotic cartilage and are not defects in endochondral ossification.
Deep lesions on MRI displayed a variety of histologic changes. An interesting finding in the CSM horses was the presence of osseous cyst–like structures within the trabecular bone, away from the articular surface. To the authors’ knowledge, this is the first report of these lesions in the articular processes of CSM horses. On micro-CT, all 4 articular processes with deep lesions were visualized as focal areas devoid of trabecular bone structure (Fig. 4). Histopathology confirmed that 3 of the 4 deep lesions analyzed using micro-CT were structures composed of an empty lumen, lined by layered polygonal cells, and surrounded by organized fibrous connective tissue. Classically, bone cysts are characterized as simple, subchondral, or aneurysmal. 3 Recent work has identified true cysts and pseudocyst types. True cysts are closed cavities with a distinct lining that is not necessarily epithelial in origin. In contrast, pseudocysts are not separated from the surrounding tissue by a distinct lining. 19 Structures observed in the articular processes fit with the true cyst classification. The exact cause of bone cysts is unknown. Suspected causes include vascular malformations, hemorrhage, ischemic necrosis, occlusion of venous drainage, or developmental abnormalities. 3,5,10
The identification of these bone cysts generates the following question: are these structures related to osteochondrosis in some fashion? As noted earlier, OC is a developmental problem of endochondral ossification affecting bone and cartilage in diarthrodial joints. Subchondral bone cysts adjacent to the articular cartilage have been described with OC. It is unknown if the cysts in the current study were a manifestation of chronic OC or an unrelated entity. Their localization was frequently deep in the trabecular bone, away from the articular cartilage–subchondral bone interface, which could confound the relationship with OC.
While the identification of the bone cysts is novel in the articular processes in CSM cases, there are previous reports of this lesion in other bones of the horse. Bone cysts have been reported in appendicular joints, including the fetlock joint, carpal joint, tarsal joint, navicular bone, and phalanges. The presence of these lesions is often associated with trauma but can also be related to developmental factors. 2,16 They can be either incidental or clinically significant. If the surrounding bone is normal, then cysts are usually interpreted as incidental. In cases where adjacent sclerosis is observed, cysts are considered significant. 16 Using these criteria, both incidental and significant cysts were observed in the CSM horses.
Another interesting lesion observed in several cases was varying degrees of fibrous replacement of marrow elements and trabecular bone often surrounded by marked bone remodeling (Figs. 14, 15). This fibrosis was observed both with and without OC lesions of the articular process. The remodeling bone was characterized by haphazardly arranged trabeculae that contained numerous irregularly distributed osteocytes, were lined by osteoblasts (woven bone), and exhibited scalloped basophilic cement lines indicative of active bone resorption and replacement. These foci of fibrous connective tissue and collagen surrounded by bone remodeling could represent sites of previous injury that were in the process of stabilization and repair. Foci closer to the articular surface could be a response to adjacent chronic OC lesions. The cause of the fibrous foci deeper in the trabecular bone is unknown but interesting nonetheless. One possibility is the deeper lesions could be previous bone cysts that collapsed and were healing. Areas of fibrosis, as well as the true bone cysts, could also represent healing and resolution of OC lesions, as has been reported in pigs. 18 Identifying the original cause of these lesions may help clarify contributing steps in CSM pathogenesis.
Spicules composed of various amounts of cartilage matrix were observed in the trabecular bone of both control and CSM horses. This feature likely represents modeling of the bone through the growth phase. As mentioned previously, equine vertebral development continues until growth plate closure at approximately 5 years of age. 28 This lesion was identified primarily in horses younger than 2 years, which is consistent with the majority of vertebral growth and development occurring by puberty.
The final deep lesion observed was characterized by well-defined, prominent venous sinuses scattered in the marrow spaces adjacent to the articular surface near OC lesions and deep in the trabecular bone of an articular facet from CSM equine No. 8. Hematopoietic elements in these areas were rare. The significance is unclear but could represent a reparative process.
Varying degrees of trabecular bone sclerosis were observed adjacent to the superficial and deep lesions. Previous studies have described trabecular bone sclerosis in the dorsal lamina and vertebral body endplates of vertebrae in CSM horses. 13,21,26 Bone sclerosis can develop due to impaired function of osteoclasts and osteoblasts, as well as metabolic signals that affect normal remodeling and resorption. However, osteosclerosis can also occur as a compensatory response to increased mechanical stress, with suppression of bone resorption resulting in an increase of bone mass as described by Wolff’s law. When occurring in response to biomechanical forces, areas of osteosclerosis contain normal-sized lacunae. 20,21,30 This was observed for the sclerotic regions of subchondral and trabecular bone in the current study, implicating biomechanical forces as the cause rather than an impairment of normal bone turnover from cellular or hormonal mechanisms.
Given previous reports and the observations in the current study of osteosclerosis in the articular processes, the trabecular bone volume of the entire articular process in CSM and control horses was evaluated. Although mean trabecular bone volumes were numerically greater in CSM horses in each category (Table 2), the differences were not significant. Combining samples from the superficial and deep lesion groups yielded a P value of .051. Given the extent of trabecular bone thickening identified in the superficial, deep, and mixed lesions during histologic examination, it is quite possible that with an increase in sample size, significant trabecular bone volume differences would be evident.
Other comparisons that were not significant included the frequency of superficial lesions at compression sites, frequency of superficial lesions at noncompression sites, and the severity of superficial lesions at noncompression sites. A possible explanation is that all superficial lesions in this study were identified as some form of osteochondrosis. Prevalence of osteochondrosis in the Thoroughbred is estimated at ∼25% and has been documented in the cervical column of horses previously. 11,13,24 The prevalence of osteochondrosis in general and its observation in both control and CSM horses in this study may explain the lack of significance in several of the superficial lesion comparisons.
Taken together, the data reported here provide further evidence that developmental abnormalities during cervical vertebrae growth and maturation are important in the pathogenesis of equine CSM, manifested as both osteochondrosis and possibly true bone cysts. It will be useful to investigate if increases in the frequency and severity of similar bone and cartilage lesions are observed in other regions of the vertebral column, as well as in the appendicular skeleton in CSM horses. In contrast, osteosclerosis may reflect a compensatory response in still-maturing CSM horses to abnormal biomechanical stresses on the cervical column. Therefore, both developmental and biomechanical mechanisms may lead to the bone and cartilage changes observed in CSM. A model where biomechanical changes are secondary to primary developmental issues seems more likely. The intersection of developmental and biomechanical influences in the growing horse sets the stage for a complex interaction of variables that leads to the pathology observed in CSM. There is a variety of critical time points in utero and during postnatal development necessary for synchronous skeletal growth and maturation. Future studies focusing on associations of CSM etiologic factors (high planes of nutrition, abnormal growth rates, abnormal copper and zinc levels, inherited genetic determinants) with specific bone and cartilage pathology in cervical vertebrae will help further elucidate the pathogenesis of equine CSM.
Footnotes
Acknowledgements
We sincerely thank contributing owners and veterinarians for their support of this study. We also gratefully acknowledge Dr Alan Loynachan for critical review of the manuscript as well as the technical assistance of Sara Welsh, Susan Minnis, Eva Langlois, Adriel Stizes, and Emily Zurkuhlen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported financially by the Grayson-Jockey Club Research Foundation, the Morris Animal Foundation, the Lourie Foundation, and the Maxwell H. Gluck Equine Research Center.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.