
Abstract
Canine toxic epidermal necrosis (TEN), a rare and life-threatening cutaneous drug reaction, traditionally has been described as full-thickness devitalization of the epidermis with minimal dermal inflammation; however, few reports detail the histologic findings. We characterize the clinical features and histologic variations of 3 canine TEN patients. Clinically, irregular erythematous and purpuric macules evolved into widespread and severely painful erosions. The number of eroded mucosae varied; however, periocular and perilabial mucocutaneous junctions frequently were affected. Thirteen of 17 biopsies were evaluated. Apoptosis at multiple epidermal levels was the most common pattern of epidermal necrosis (12/13 biopsies, 92%). In contrast, full-thickness coagulation necrosis was present less often (7/13 biopsies, 52%). Lymphocytic interface dermatitis was the predominant inflammatory pattern, and intraepidermal lymphocytes, along with fewer histiocytes, were present to some degree in all samples along with lymphocytic satellitosis of apoptotic keratinocytes. The sequence of changes points to lymphocyte-mediated keratinocyte apoptosis as an early step in lesion development with subsequent variation in progression to coagulation necrosis among patients. Histopathologic changes overlapped with those reported for erythema multiforme, in contrast to traditional histologic descriptions of canine TEN. A specific algorithm for assessment of drug causality in epidermal necrolysis (ALDEN) was applied for each patient; carprofen was associated with a probable score for causality in 1 dog. Clinicians should be encouraged to take multiple biopsies in TEN suspect cases as nearly 25% of all biopsies lacked epithelium and were not diagnostic.
Toxic epidermal necrolysis (TEN), previously called Lyell syndrome, is a delayed-type cutaneous immune reaction involving cytotoxic T-lymphocyte and natural killer cell activation. 18 The currently accepted clinical classification in humans and dogs defines Stevens-Johnson syndrome (SJS) and TEN as variants of the same disease spectrum that are different from subsets of erythema multiforme (EM) in characteristic clinical appearance and causality. 4,12
Traditionally, human EM and SJS/TEN have been differentiated by the degree of inflammation and pattern of epidermal necrosis. Erythema multiforme is characterized by lymphocyte-rich inflammation that targets epidermal keratinocytes (satellitosis) and induces apoptosis at multiple epidermal levels. In contrast, lesions of SJS/TEN have fewer leukocytes and more extensive to full-thickness coagulative epidermal necrosis. 20,23 Histopathologic findings in canine EM and SJS/TEN often overlap, making it difficult to subcategorize the different EM-TEN group entities based on histopathologic features alone. 12 To complicate this issue further, current canine dermatology review publications and textbooks continue to define TEN as having full-thickness devitalization of the epidermis with minimal dermal or epidermal inflammation. 10,16,28 Unfortunately, histopathologic descriptions of well-defined canine TEN cases are lacking in the literature.
Drugs are thought to induce most cases of SJS/TEN, but infectious triggers dominate in EM, which implicates drug withdrawal as a crucial requirement for therapy and prognosis of SJS/TEN. 12,24 A new disease-specific algorithm, Assessment of Drug Causality in Epidermal Necrolysis (ALDEN), has been recently validated for human patients with SJS/TEN, and it shows superiority to previous algorithms. 24 However, veterinary algorithms for assessing causal drug exposure in SJS/TEN cases are not standardized or commonly used, resulting in suspicion without definitive proof of drug association. 10,16,28
The aim of this study was to characterize the clinical skin lesions and histopathologic features of biopsies from 3 dogs with TEN. For the first time, we applied the ALDEN algorithm to assess drug causality in these dogs.
Materials and Methods
Case Selection
We identified 3 dogs in which a diagnosis of TEN was made based on an international consensus clinical classification validated for humans
4,30
and modified in 1998 for use in dogs.
12
A diagnosis of TEN was made if the dog’s disease fulfilled the following criteria: an acute disease evolution (ie, less than 7 days between the inception of the first skin lesions and the appearance of visible epidermal detachment); and the presence of erythematous and/or purpuric macules and patches with easily detachable epidermis, with or without blisters; and the presence of epidermal detachment on more than 30% of the body surface area (BSA); and/or the presence of eroded mucosae; and/or the presence of prodromal signs such as lethargy, anorexia, fever, ocular discharge, conjunctivitis, pruritus, or skin pain that precede skin lesions by 3 to 14 days.
4,12
Estimation of the percentage of BSA detachment in dogs was calculated, as for human patients with TEN, with a simple and rapid burn unit method, the so-called rule of nines, which divides the body into regions that are multiples of 9% of total BSA. 4 In dogs, each forelimb represents 9%; each rear limb 2 nines, or 18%; the head and neck 9%; and the dorsal and ventral thorax/abdomen each 18% of total BSA. 7
Histologic Methods
Hematoxylin and eosin–stained histologic sections from every skin and mucosal biopsy sample collected from each case (Table 1) were reviewed. Four clinical skin biopsies were available from dog No. 1 and 5 from dog No. 2. Seven skin samples were collected from dog No. 3 at postmortem. One sample of mucosa was also available for dog No. 3, yielding a total of 17 biopsies. For each biopsy sample, specific histologic changes were evaluated for severity using a standard scale of minimal, mild, moderate, and marked. 12 When biopsy samples were bisected to create 2 histologic sections, changes were assessed for the section with the most developed lesions.
Summary of Inclusion Criteria for 3 Dogs With Toxic Epidermal Necrolysis.
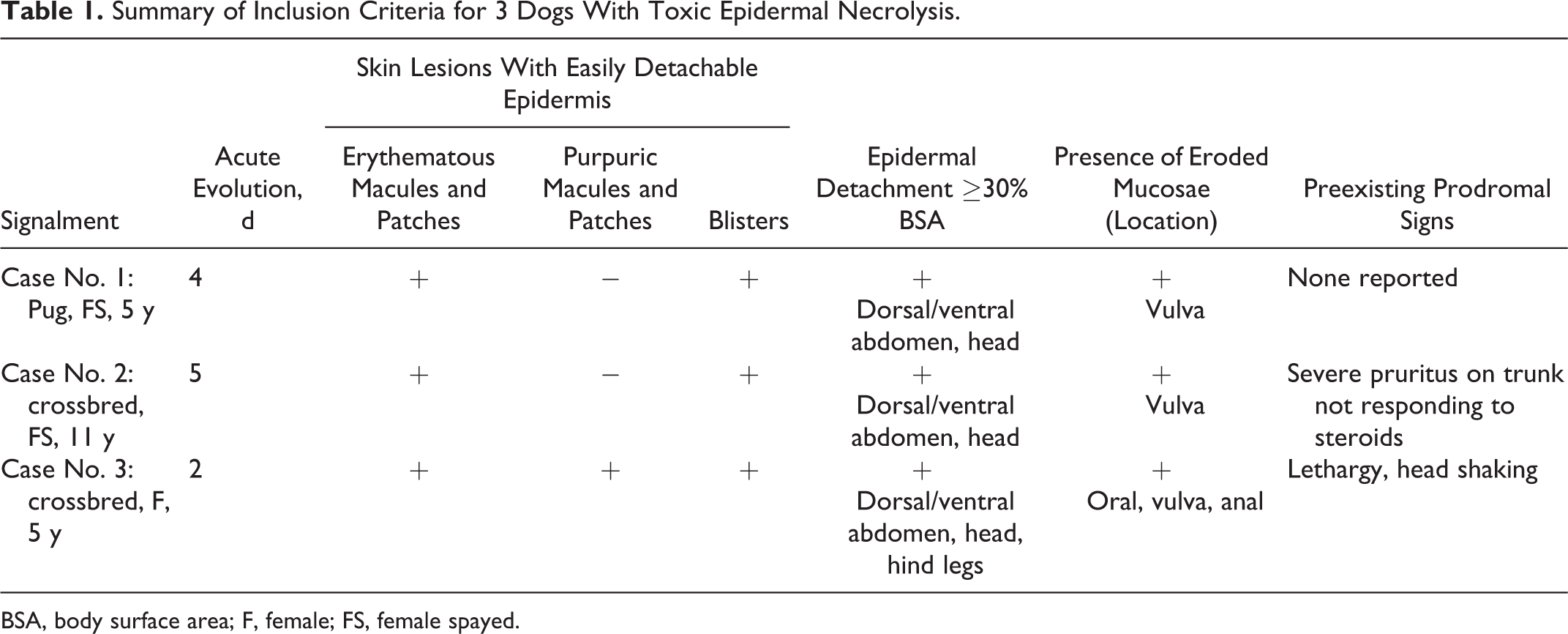
BSA, body surface area; F, female; FS, female spayed.
Biopsies were assessed for patterns of epidermal necrosis that included full-thickness or partial-thickness laminar coagulation necrosis; the latter was either superficial or deep. The degree of apoptosis (single-cell necrosis) of keratinocytes was evaluated in the stratum basale, predominately deep layers, predominately superficial layers, or multiple epidermal layers; in the latter, apoptosis involved the stratum basale, stratum spinosum, and stratum granulosum concurrently. Progression of apoptosis to coagulation necrosis in the epidermis was observed as apoptotic keratinocytes entrapped in coagulation necrosis. The early presence and persistence of apoptosis was determined by observing entrapment of apoptotic bodies in layers of the stratum corneum above active keratinocyte apoptosis in the epidermis directly below. Ulcers were recorded, as was the pattern of necrosis at ulcer margins. Epidermal hydropic degeneration (intracellular edema) and spongiosis (extracellular edema) were recorded.
Inflammatory infiltrates and patterns of infiltration were characterized in the epidermis and dermis separately, including the degree and character of interface dermatitis. Dermal inflammation was not assessed below ulcers. Finally, the amount of lymphocytic satellitosis of apoptotic keratinocytes was determined, as was the extension of epidermal and inflammatory changes into hair follicle epithelium.
Assessment of Drug Causality
To assess for the probability of a drug causing TEN, we used the ALDEN algorithm as for humans (see Suppl. Table S1). 24 This algorithm was applied to every drug given to each canine patient at any time in the 2-week period preceding and including the probable index day. The probable index day represents the day when the TEN symptoms first started, including prodromal signs. For assessment of the prechallenge parameter for veterinary drugs, we used the World Health Organization’s (WHO’s) anatomical therapeutic chemical (ATC) codes (http://www.whocc.no/atcddd) for evaluation of molecular structure similarity. Drugs were considered similar if they shared an ATC code up to the fourth level (ie, chemical subgroup); they were considered identical if they shared an ATC code up to the fifth level (ie, chemical substance). A total score, varying from –12 to +10, was assigned to each drug taken by each patient. The scores attributed to each drug were pooled in categories aimed at reflecting causality: “very probable,” score ≥6; “probable,” score 4–5; “possible,” score 2–3; “unlikely,” score 0–1; and “very unlikely,” score <0. 24
Results
Clinical Summary
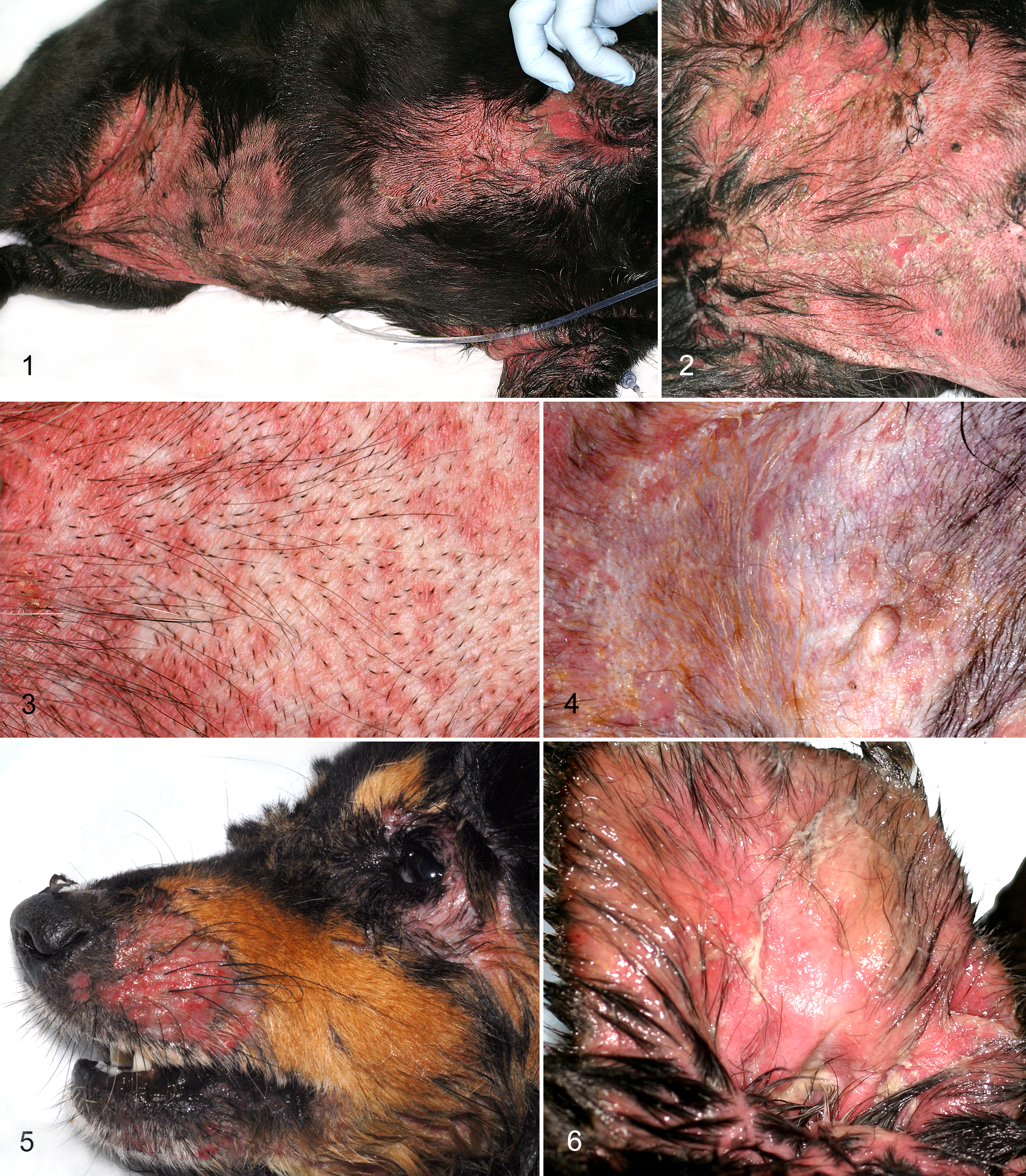
Toxic epidermal necrolysis was diagnosed in 3 dogs (Table 1). The most common skin lesions were erythematous (all dogs) and purpuric (dog No. 3) macules/patches of irregular shape and size that rapidly evolved into widespread, confluent erosions with detached or easily detachable epidermis (Figs. 1–4). A positive pseudo-Nikolskiy sign, 9 in which epidermal separation could be elicited by applying lateral pressure on erythematous but not normal-appearing skin, was seen in all cases. Although owners reported visible blistering in each case, large sheet-like areas of superficial epidermal peeling without preexisting blisters were seen in all dogs (Fig. 1). All dogs had at least 1 mucosa affected (Table 1). The periocular and perilabial areas were the most commonly affected mucocutaneous junctions (Fig. 5). In all dogs, concave pinnae were bilaterally moist and eroded, usually at the onset of the skin lesions (Fig. 6). While the dorsal and ventral interdigital spaces exhibited hemorrhagic erosions and detached epidermis in 1 dog (dog No. 3), sloughing of the paw pads or claws was not a feature in any patient. The TEN skin lesions were painful in all dogs, with 2 dogs having extremely severe pain and pruritus (dog Nos. 2 and 3). All dogs were initially treated with supportive therapy and glucocorticoids. As the disease rapidly progressed, the owners elected euthanasia in all cases.
Histopathology Results
A total of 13 of 17 biopsy samples, representing all 3 dogs, allowed for a diagnosis of an epidermal necrotizing disease of the EM-TEN spectrum, whereas complete ulceration and loss of follicular epithelium left 4 biopsies nondiagnostic. While all samples lacked dermal necrosis, multiple patterns of epidermal necrosis and inflammation were present in the same case.
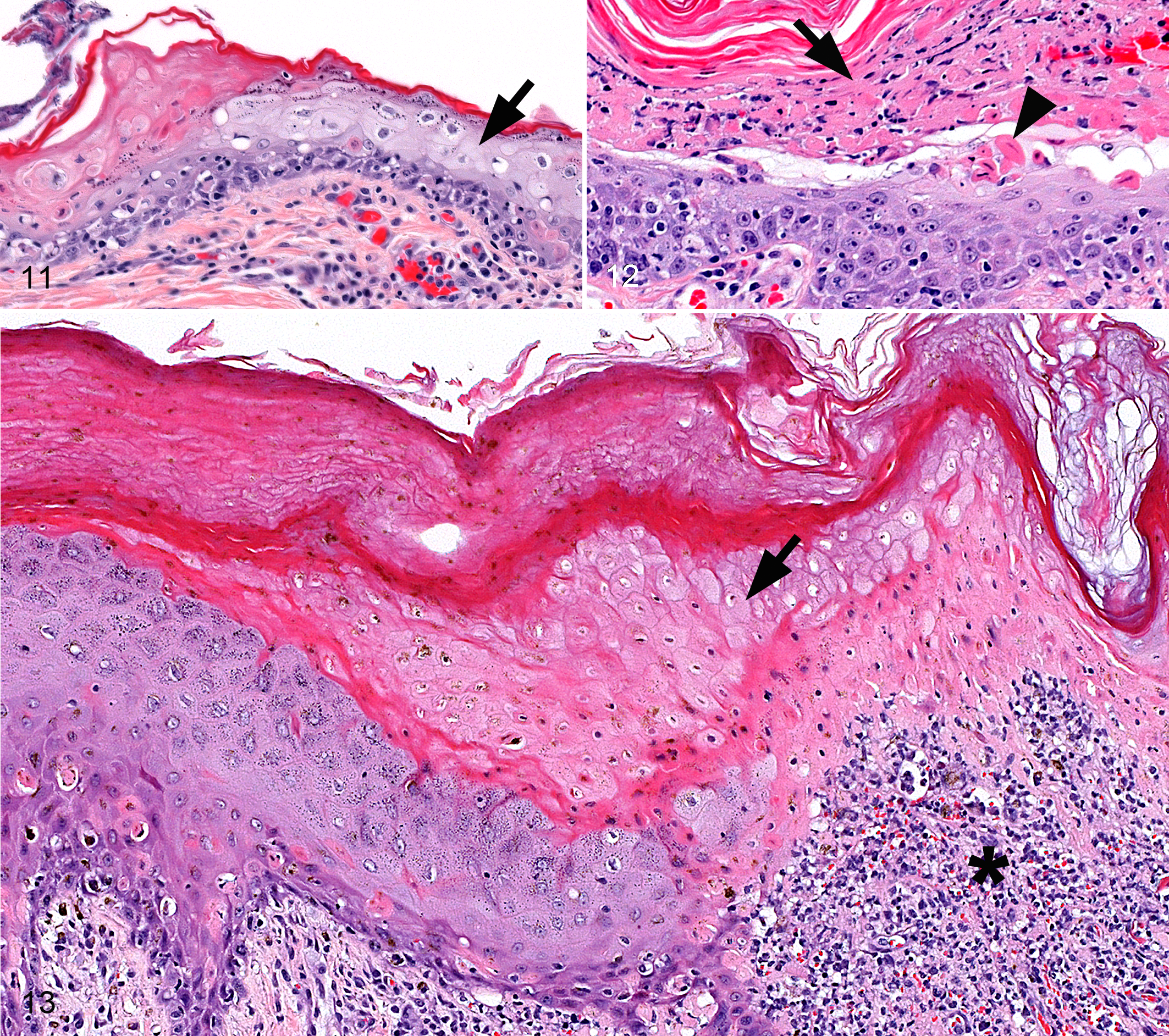
Apoptosis at multiple epidermal levels was the most common pattern of necrosis and was present in all dogs (12/13 biopsies, minimal to marked; Fig. 7). In some biopsies, apoptosis predominated in the superficial epidermis (4/13 biopsies, mostly marked; Fig. 8), while in others, it predominated in the deep epidermis (9/13 biopsies; Figs. 9, 13), where it mirrored the severity of basal cell apoptosis (12/13 biopsies, minimal to marked). Apoptosis was sometimes restricted to ulcer margins, where it became confluent (2/13 biopsies; Fig. 7) or restricted to the margins of full-thickness epidermal coagulation necrosis (5/13 biopsies; Fig. 9). Full-thickness epidermal coagulation necrosis was seen least often (7/13 biopsies; Figs. 9–11, 13). Areas of laminar epidermal necrosis (9/13 biopsies; Fig. 12) were mostly superficial, were sometimes deep, affected a very small or large area of the epidermis, and merged with full-thickness necrosis in some biopsies. When marked, superficial laminar necrosis caused separation of the upper epidermis.
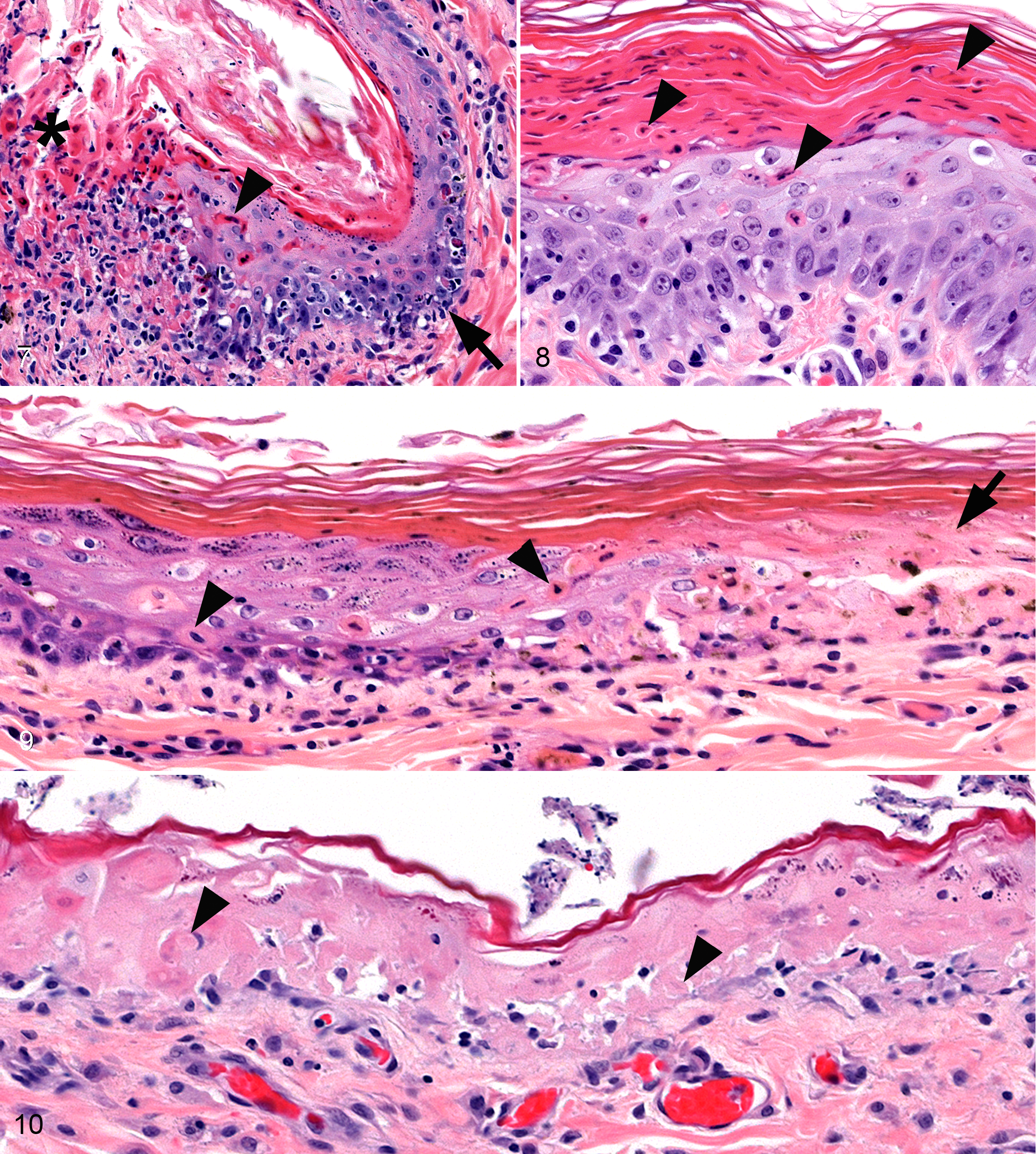
The progression of early apoptosis to coagulation necrosis was indicated by entrapment of apoptotic keratinocytes, some with lymphocytic satellitosis, in zones of coagulation necrosis (7/13 biopsies; Fig. 10), whereas ongoing keratinocyte apoptosis below apoptotic bodies entrapped in hyperkeratotic stratum corneum provided evidence of early and sustained apoptosis at the same epidermal location (4/13 biopsies; Fig. 8). Conversely, rapid progression of coagulation necrosis in some biopsies was supported by retention of a normally thin stratum corneum and a lack of epidermal hyperplasia, significant entrapment of apoptosis, or entrapment of inflammatory cells in full-thickness necrotic areas (Fig. 10).
Interestingly, the type and combination of necrosis patterns varied among cases. In dog No. 1, apoptosis and laminar coagulation necrosis dominated in the superficial epidermis, and ulcers were least developed. In dog No. 2, for only a short distance from ulcer margins, apoptosis dominated in the basal layer, progressed to apoptosis at multiple epidermal levels, and became confluent at the ulcer margins with marked lymphocytic satellitosis. In dog No. 3, apoptosis dominated in the basal layer and lower epidermis at lesion margins and progressed to mostly full-thickness coagulation necrosis.
Ulcers were frequently observed (14/17 biopsies), and some ulcers were accompanied by marked surface bacterial colonization. While spongiosis was not a feature of biopsies, hydropic degeneration of keratinocytes was common (9/13 biopsies), bordering apoptosis or coagulation necrosis, and was observed entrapped in zones of coagulation necrosis in some areas (Fig. 11). Follicular epithelial necrosis developed mostly in the infundibulum and mirrored epidermal necrosis patterns in each dog.
An epidermal inflammatory cell infiltrate was common (13/13 biopsies)—mostly lymphocytic exocytosis and lymphocytic satellitosis of apoptotic cells—and was mostly moderate to marked. Macrophages were also present in the epidermis (8/13 biopsies, mostly minimal). Lymphocytic satellitosis of apoptotic cells was present in all samples with apoptosis (13/13 biopsies, minimal to marked). Lymphocytic interface dermatitis was the most common inflammatory pattern in biopsies (13/13 biopsies, minimal to moderate; Figs. 7, 9, 13) and was often only seen in small areas, such as those bordering an ulcer. Perivascular dermatitis was equally common. The dermal inflammatory cell infiltrate underlying epidermal necrosis was generally minimal to mild and dominated by lymphocytes but was moderate in 2 biopsies and marked in 1 biopsy (Fig. 13). Macrophages were present less often (8/13 biopsies, minimal to mild). Plasma cells and neutrophils were common below ulcers but were not observed beneath intact epidermis. Occasionally, macrophages and rarely a few multinucleated histiocytic giant cells infiltrated the adjacent dermis and basal area of necrotic epithelium. Similar inflammation as in the epidermis targeted hair follicles and predominately involved the infundibulum.
Assessment of Drug Causality
The ALDEN algorithm was applied for each drug (Table 2). None of the 3 dogs had any known liver or kidney function alterations that could have been considered in the ALDEN calculation. Dog No. 1 presented with a history of tramadol (Tramadol Hydrochloride; Amneal Pharmaceuticals, Bridgewater, NJ) administration 3 times daily for treatment of bilateral patellar luxation during the last 12 months and received a booster vaccination (Nobivac canine 1- DAPPvL 2 +Cv; Intervet/Schering-Plough Animal Health, New York, NJ) 7 weeks before the probable index day. The ALDEN was not applied for the vaccine because a causal link between TEN and vaccinations has not been established, 2 and the time between application and probable index day exceeded 2 weeks. Dog No. 3 was given a 10-day course of oral carporfen (Rimadyl; Zoetis, Kalamazoo, MI) twice daily with the last dose administered 11 days before the probable index day. Importantly, this patient was rechallenged with carprofen after the probable index day due to severe pain and lack of initial suspicion of TEN. Only in dog No. 3 was drug causality assessed as probable for carprofen; the ALDEN categorized causality for tramadol in dog No. 1 as very unlikely, while in dog No. 2, no known drug administration was found.
Causality Assessment Using Algorithm of Drug Causality for Epidermal Necrolysis (ALDEN) for 3 Canine Cases of Toxic Epidermal Necrolysis.
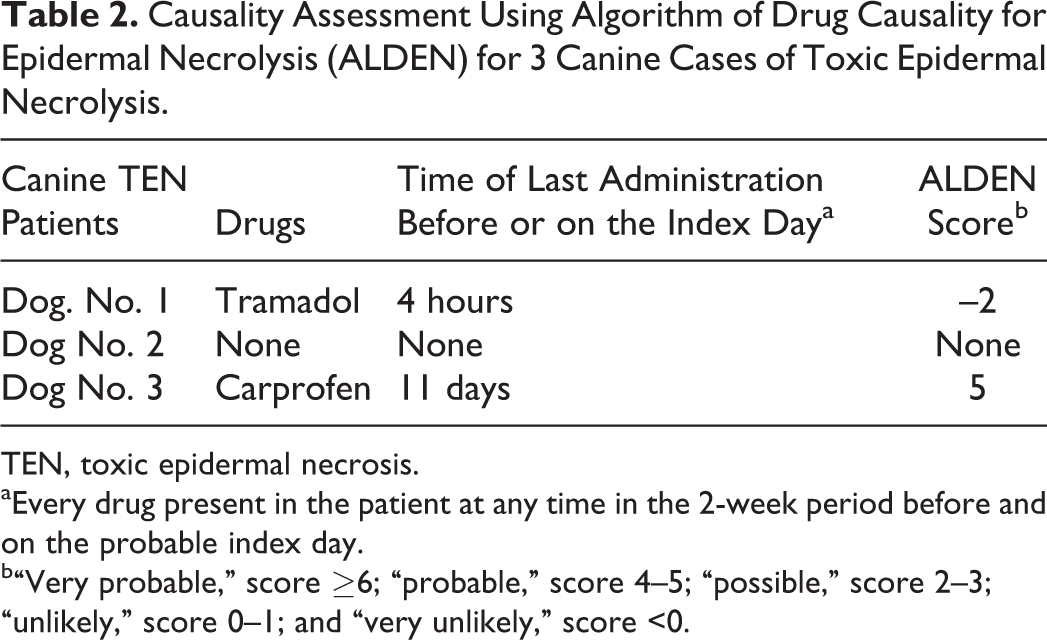
TEN, toxic epidermal necrosis.
aEvery drug present in the patient at any time in the 2-week period before and on the probable index day.
b“Very probable,” score ≥6; “probable,” score 4–5; “possible,” score 2–3; “unlikely,” score 0–1; and “very unlikely,” score <0.
Discussion
We describe 3 cases of canine TEN, a rare life-threatening skin disease characterized by extensive destruction of the epidermis and mucosal epithelium that is homologous to TEN in humans. 4,12 A clinical consensus classification has characterized human TEN skin lesions as flat atypical targets or macules with or without blisters and concurrent epidermal detachment of more than 30% of the body surface. 4 Recently, the classification of human TEN has been slightly modified by the inclusion of a flat typical target missing the palpable ring as an additional lesion. These lesions are short-lived and usually evolve into flat atypical targets. 29,30 Importantly, this modified classification postulates that lesions of EM are normally raised, while skin lesions of SJS and TEN are always flat. Notably, SJS/TEN lesions can blister in the center, and this does not denote raised lesions according to current definitions. The clinical usefulness of this new modified human classification scheme 29,30 has yet to be determined in veterinary medicine. All dogs reported herein initially exhibited flat erythematous macules and patches, with 1 dog also having flat purpuric macules on the ventral abdomen. Flat typical or atypical target lesions were not seen in any of our cases, nor have they been reported in any dog with TEN.
In dogs and humans, the main clinical sign distinguishing TEN from SJS is the amount of body surface area with epidermal detachment, which is defined as any necrotic skin that is already detached (eg, blisters, erosions) or that is detachable (ie, areas with a positive pseudo-Nikolskiy sign) at the worst stage of the disease. 4,9,11 Some humans initially exhibit epidermal detachment over less than 10% of their body surface, an extent typical of SJS, but progress to 30% of the body surface area in a few days, which is more typical of TEN. 4,6 Similarly, epidermal detachment progressed to more than 30% of body surface over a period of 2 to 3 days in all 3 of our canine cases. This progression illustrates that the timing of clinical lesions should be taken into account when classifying SJS/TEN in dogs. Different authors have reported the presence of a direct Nikolskiy sign in dogs with TEN. 10,16 A direct Nikolskiy sign is the ability to separate the epidermis from the dermis by application of lateral digital pressure on normal-appearing skin distant from any lesions; it is characteristic for pemphigus vulgaris. 9 In contrast, the pseudo-Nikolskiy denotes the same ability applied to erythematous skin and most commonly presents in SJS or TEN lesions; it is not specific to SJS/TEN. 9,11 All 3 dogs reported herein exhibited a pseudo-Nikolskiy sign but not a direct Nikolskiy sign.
The current diagnostic classification of human TEN does not depend on the presence of mucosal involvement, although in more than 90% of patients, erythema and erosions of buccal, oral, and/or genital mucosae are seen. 4,11 This might be because the initial classification was primarily based on severe, hospitalized cases that had widespread mucous membrane involvement. 4 The current classification for canine TEN stipulates “involvement of at least two mucosae” as one of the clinical diagnostic criteria. 12 We propose that this diagnostic criterion in dogs be revised because 2 of our patients had only 1 mucosal site affected despite exhibiting sufficient clinical and histologic features to confirm the diagnosis of TEN. Strict adherence to this criterion could potentially prevent an early diagnosis of TEN and affect patient survival if aggressive TEN-directed therapy is not immediately instituted. Humans with TEN may describe influenza-like prodromal signs characterized by malaise, nausea, vomiting, anorexia, headache, chest pain, myalgia, arthralgia, fever, cough, rhinitis, conjunctivitis, pharyngitis, and/or pruritus. 11,22 The prodromal phase lasts from 1 day up to 2 weeks, and it typically precedes the development of characteristic cutaneous lesions by a few days. 11,22 Although detecting some of these can be challenging, Gross et al 10 reported fever and malaise as prodromal signs in canine TEN. Pruritus has been reported in 28% of humans with SJS or TEN; 22 severe generalized pruritus, pain, and lethargy with head shaking were seen as prodromal signs in 2 of our dogs.
In our cases, histopathologic changes overlapped with descriptions of EM and SJS/TEN. 10,12 This observation is in contrast to previous descriptions of canine TEN, which emphasize full-thickness coagulation necrosis of the epidermis and absent or minimal inflammation as key diagnostic features. 10,16 These features were seen in only 1 case and were not as common in biopsies as were lesions traditionally considered diagnostic for EM—namely, lymphocytic interface dermatitis and apoptosis at multiple epidermal levels with lymphocytic satellitosis, 10,12 which were present to a variable degree in all cases. In addition, full-thickness epidermal necrosis is not unique to TEN and occurs in the centers of human EM major lesions. 20,23 Our results are consistent with TEN in humans, 19 in whom histopathologic examination confirms but lacks specificity to differentiate EM and SJS/TEN. Furthermore, this reinforces the findings of Hinn et al, 12 which emphasized the need for clinical information to differentiate these conditions in dogs. In our study, nearly 25% of all skin biopsies lacked epithelium and were not diagnostic. As a result, we recommend the collection of multiple skin biopsies (a minimum of 6 biopsies, 8 mm in diameter) to confirm a clinical diagnosis of TEN. Biopsies should include ulcer margins and adjacent, intact, viable epidermis in zones of erythema to ensure capture of active epidermal necrosis.
We identified keratinocyte apoptosis to be an early event in TEN lesion development in the dogs evaluated, based on the presence of apoptotic cells either entrapped in areas of epidermal coagulation necrosis underlying normal startum corneum or incorporated into the stratum corneum over ongoing epidermal necrosis. In addition, lymphocytic satellitosis was commonly observed even with early apoptosis. Taken together, lymphocyte-mediated cytotoxicity of individual keratinocytes appears as an early step in TEN lesion development in some dogs, which is consistent with the proposed pathogenesis of drug- or drug/peptide-specific T-lymphocyte and/or natural killer–cell initiation of TEN in humans. 25 Based on the histomorphology of our cases, progression of this early lymphocyte-mediated apoptosis lesion can vary considerably. In 1 dog, lesions progressed rapidly to full-thickness coagulation necrosis of the epidermis without significant leukocyte influx, similar to classic descriptions of TEN. 10,16 In the other dogs, apoptosis with lymphocytic satellitosis remained the dominant pattern of necrosis, and progression to coagulation necrosis was relatively limited, was sometimes only laminar, or was not visualized. Lymphocyte-derived granulysin is considered an important soluble mediator of epidermal necrosis in humans with TEN, and it would be interesting to know if dogs progressing rapidly to full-thickness necrosis have increased lesional granulysin or other soluble mediator(s) to explain this variation. 5,25 Transition to a soluble mediator of cell death might explain the development of inflammatory cell–poor lesions in dogs. In contrast, the dogs that do not make such a transition could retain direct lymphocyte-mediated cell death as the dominant necrosis pattern, develop cell-rich lesions, and thereby mimic lesions of EM histologically. The common observation of epidermal zones of hydropic degeneration in this study could indicate a component of cellular injury occurring via soluble mediator(s). In addition to granulysin, multiple soluble mediators have been proposed in TEN that might work alone or in concert to induce keratinocyte death, including electrophilic drug metabolites, reactive oxygen species, nitric oxide, soluble Fas-ligand, and/or tumor necrosis factor (TNF)–α. 25 Although lymphocytes were the dominant cell type in the epidermis in this study, macrophages (likely dendritic-type cells) were also present in the epidermis in lower numbers, which has been described in people as possibly playing an important pathogenic role such as lymphocyte co-stimulation or contribution of soluble mediators of cell injury, such as TNF-α, TRAIL, and TWEAK. 25
Dermal necrosis was not present in any of the 17 biopsies in this study despite large ulcer development and bacterial colonization in some cases. Therefore, the presence of well-developed dermal necrosis below active epidermal necrosis, especially early in skin lesion development, may be a valuable criterion for excluding TEN. This is important because the exact depth of skin necrosis, when shallow, can be difficult to determine clinically, and histologic examination aids disease classification. There are examples in the literature of cases reported to be TEN 1,13,26 that lacked sufficient clinical criteria for TEN and had evidence of dermal necrosis; these were more likely examples of thermal injury or vascular disease in which dermal necrosis can be a feature.
In the current TEN classification of humans and dogs, drugs appear to be the major causal factor. 24 Immediate withdrawal of suspected medication is a crucial requirement for improving TEN prognosis in humans. 8 Currently, the ALDEN algorithm has been validated for, is highly specific to, and is recommended for assessing drug causality in human SJS/TEN cases. 24 An important requirement for applying the algorithm is a precise clinical history to allow for the determination of the probable index day, the day when prodromal signs started. In our study, there was no drug association found in 2 dogs while 1 dog showed a probable ALDEN score for carprofen. Carprofen hypersensitivity has been suspected as the cause of drug eruption resembling Sweet syndrome in 2 dogs 27 and as a cause of neutrophilic dermatitis and vasculitis in 1 dog. 15 To the authors’ knowledge, this is the first reported association between carprofen and TEN. Carprofen belongs to the propionic acid class of nonsteroidal anti-inflammatory drugs (NSAIDs), including ketoprofen, ibuprofen, naproxen, benoxaprofen, and fenoprofen, 6 with which carprofen shares an ATC code up to the fourth level (WHO). Currently among NSAIDs, oxicam derivatives are associated with a higher risk and acetic acid derivatives with a lower risk for SJS and TEN. 24 The propionic acid derivatives are thought not to be associated with significant risk, although probable ALDEN risk has been shown for ketoprofen and naproxen. 24 Furthermore, several human patients with ibuprofen-induced TEN were recently reported. 3,14 Interestingly, similar to current human data, 1 of our cases presented with only long-term tramadol administration, for which the ALDEN showed a very unlikely association to TEN. 24 Although the generally accepted hypothesis is that SJS and TEN are nearly always drug related, epidemiologic studies have shown that only approximately 65% of SJS and TEN cases in humans are induced by drugs. 21 However, with the application of the ALDEN, cases became attributable to certain previously unidentified drugs. Still, 15% of patients remain for which drug causality cannot be implicated. 24 Growing suspicion exists that some cases may be caused by infections such as Mycoplasma pneumoniae, but strong evidence for this assertion is lacking. 17 The current conclusion is that a very small fraction of SJS and TEN cases are idiopathic. 24
In conclusion, this study identifies histologic variation in the patterns of necrosis and degree of inflammatory cell infiltrate in the skin of dogs with TEN and illustrates histologic overlap between EM and TEN. Therefore, a pathologist’s microscopic interpretation should be restricted to an umbrella diagnosis of an EM-TEN epidermal necrotizing disease, and further subclassification of the different entities should depend on patient history, clinical signs, and skin lesion extent. In suspect TEN cases, clinicians should be encouraged to take multiple biopsies since nearly 25% of all skin biopsies in this study lacked epithelium and were not diagnostic. Application of algorithms for drug causality, such as the ALDEN, in more canine cases will help to validate their use and provide stronger evidence for drug causation in TEN. Applying the ALDEN in this study successfully identified carprofen as the probable cause for TEN in a dog for the first time.
Footnotes
Acknowledgements
We acknowledge Sandra Horton for excellent histology preparations of samples.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.