
Abstract
Pulmonary alveolar proteinosis is a rare human disease characterized by accumulation of surfactant in alveoli without generating an inflammatory response. Lung lesions resembling pulmonary alveolar proteinosis were observed in 7 adult tamarins (5 males and 2 females). Gross lesions were characterized by areas of discoloration, slight bulging over the lung parenchyma, and occasional consolidation. Histologic examination of tamarin lung samples revealed intra-alveolar accumulation of amorphous, amphophilic, periodic acid–Schiff-positive, finely granular to dense material. In some cases, type II pneumocyte hypertrophy and hyperplasia were observed with pleural and septal thickening and fibrosis. Large numbers of intra-alveolar foamy macrophages were noted surrounding and/or in the vicinity of the lesions. Immunohistochemical analysis of the lung lesions using polyclonal (surfactant proteins A, B, and C) and monoclonal (surfactant protein D) antibodies revealed the granular material to be composed largely of surfactant protein B, followed by surfactant protein A. Surfactant proteins C and D were present in lesser quantities, with the latter observed surrounding the lipoproteinaceous deposits. Transmission electron microscopy of the affected lungs showed numerous, irregularly shaped osmiophilic lamellar bodies in type II pneumocytes. The cytoplasm in alveolar macrophages was expanded, containing ingested surfactant with swollen mitochondria and rough endoplasmic reticulum. Thoracic radiographs, available in 1 animal, depicted the lesions as small multifocal opacities randomly distributed in cranial and diaphragmatic lung lobes. This is, to the authors’ knowledge, the first report of spontaneous pulmonary alveolar proteinosis in nonhuman primates.
Pulmonary alveolar proteinosis (PAP) is an uncommon disorder in humans, first described by Rosen et al. in 1958. 19 PAP is characterized by the abnormal accumulation of surfactant in alveolar spaces without the presence of inflammatory cells 7,19,21,25 and the consequent interference with gas exchange. This eosinophilic, periodic acid–Schiff-positive accumulation is due to impaired function of alveolar macrophages. 3,7,12,19,21,25 The cause of the disease appears to be multifactorial and has been classified in 3 forms: acquired, secondary, and congenital. 3,7,21,25 The disease presentation varies from subclinical to respiratory failure and death. Spontaneous improvement with resolution may also occur. 19–21,25
Treatment of PAP depends on the form. The current standard therapy for all forms is whole lung lavage to remove the accumulated surfactant. 3,13 Subcutaneous and nebulized administration of granulocyte-macrophage colony-stimulating factor (GM-CSF) has proven useful in treating the idiopathic form. 10,13 The secondary form is treated by removing the offending agent or the predisposing condition. 13 The congenital form has a poor prognosis and is treated with supportive care or lung transplantation. 13 Further reviews of current therapies and the molecular basis of PAP and surfactant homeostasis are available. 3,10,12,13,18,25 Herein we report 7 cases resembling PAP in “moustached tamarins” (Saguinus mystax).
Materials and Methods
Animals
Twenty-four adult tamarins died or were euthanized because of untoward clinical signs and/or poor response to treatment between February 24, 2006, and April 12, 2010; complete necropsies were performed. Clinical records and/or necropsy reports were not available for all animals. Of the 24 tamarins, there were 16 males and 8 females. Sixteen animals were wild caught; 5 were captive born; and the remaining 3 had no data available. From these 24 animals, 15 were used in viral hepatitis studies (hepatitis A virus and hepatitis GB virus type B; Institutional Animal Care and Use Committee approved) and 9 were on a holding protocol (research naïve; Institutional Animal Care and Use Committee approved).
Seven animals presented lesions compatible with PAP: 5 were wild caught (3 males and 2 females, 8–10 years old), with 1 male and 1 female being research naïve; 2 were captive born, a 6-year-old set of male twins (Table 1). The monkeys were maintained in accordance with the Guide for the Care and Use of Laboratory Animals 11 and the Animal Welfare Act regulations. Husbandry conditions have been described in detail. 8
Summary of Clinical, Gross, and Histologic Findings in 7 Tamarins With Pulmonary Alveolar Proteinosis a
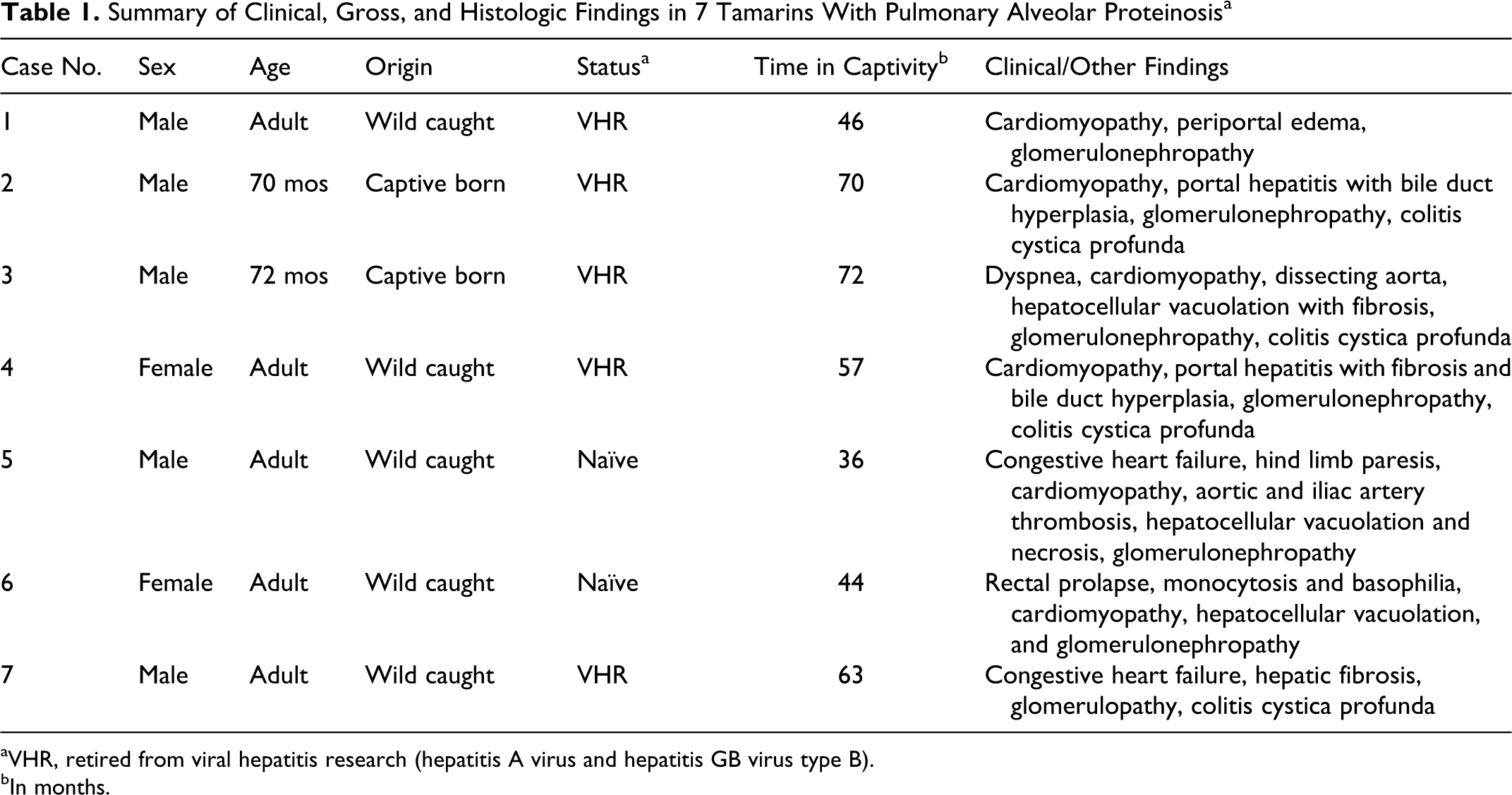
aVHR, retired from viral hepatitis research (hepatitis A virus and hepatitis GB virus type B).
bIn months.
Histochemistry
Tissues from all major organs were fixed in 10% neutral buffered formalin (NBF), embedded in paraffin, with sections cut at 5 μm and stained with hematoxylin and eosin. In addition, lung sections were stained with Masson trichrome, periodic acid–Schiff with and without diastase predigestion, Gram, alcian blue (pH 2.5), elastic van Gieson, toluidine blue, Congo red, and oil red O. 4
Immunohistochemistry
Immunohistochemistry for surfactant proteins A, B, C, and D (SP-A, SP-B, SP-C, and SP-D) was performed on formalin-fixed paraffin-embedded lung sections.
Briefly, tissues were cut into 5-μm sections and placed onto slides. For SP-A, SP-B, and SP-D, sections were deparaffinized and dehydrated, and heat-induced antigen retrieval was performed with Diva Decloaker solution pH 6.2 (Biocare Medical, Concord, CA): 20 minutes for SP-A and SP-B and 30 minutes for SP-D. Slides were processed in a DAKO autostainer (DAKO, Carpinteria, CA).
For SP-A and SP-B, Background Sniper (Biocare) was applied as a protein block. Slides were incubated for 1 hour at room temperature with either anti-SP-A antibody (Millipore, Temecula, CA; catalog No. ab3420, rabbit polyclonal, species reactivity: human, mouse, rat, primate; dilution 1:500) or SP-B mature (Abcam, Cambridge, MA; catalog No. ab40876, rabbit polyclonal, species reactivity: mouse, sheep, cow, and human; dilution 1:500). Mach 4 Universal AP Polymer (Biocare) was used as detection system, Vulcan Fast Red (Biocare) as chromogen, and CAT hematoxylin (Biocare, dilution 1:1) as counterstain.
For SP-D, endogenous peroxidase was blocked with Peroxidazed 1 (Biocare); endogenous biotin, with a commercial avidin–biotin blocking kit (Vector Laboratories, Burlingame, CA); and protein, with 10% mouse serum (Jackson ImmunoResearch, West Grove, PA), as followed by incubation for 1 hour at room temperature with a mouse monoclonal biotinylated antibody to SP-D (Abcam, catalog 15695, clone IIE11, species reactivity: human and rat, dilution 1:40). Furthermore, 4plus Streptavidin HRP Label (Biocare) was used as a detection system, Vector NovaRed (Vector) as chromogen, and Weigert’s iron hematoxylin (Electron Microscopy Sciences, Hartfield, PA; dilution 1:1) as counterstain.
For SP-C, a Leica Bond-Max Automated System (Leica Microsystems, Bannockburn, IL) was used with the Bond Polymer Red Refine Detection Kit (Leica). Slides were placed in the autostainer, and subsequent steps were performed by the automated system in the following order: deparaffinization with Bond Dewax Solution (Leica), heat-induced antigen retrieval with Bond Epitope Retrieval Solution 1 (Leica), protein block with Background Sniper (Biocare), incubation with rabbit polyclonal to SP-C at room temperature (Abcam, catalog No. 28744; species reactivity: human and mouse; dilution 1:100), detection with Polymer AP and Mixed Red Refine (Leica), and counterstained with CAT hematoxylin (Biocare, dilution 1:1). Positive and negative controls were run for each sample and each antibody.
Electron Microscopy
For transmission electron microscopy (TEM), formalin-fixed tissues from case No. 3 and from a normal tamarin lung were transferred to 2.5% glutaraldehyde overnight, then to phosphate buffer 0.1M at 7.2 pH, and to 1% osmium tetroxide. Following fixation, the samples were washed in 0.2M sodium cacodylate, dehydrated through a graded ethanol series, and embedded in epoxy resin (EMBed 812 resin Electron Microscopy Sciences). In 2 animals (case Nos. 2 and 3), the areas of interest were trimmed from the paraffin block, washed 3 times in xylene for 30 minutes each, changed to 2:1 propylene oxide:EPON, 1:2 propylene oxide:EPON, and embedded in EMBed 812 resin (Electron Microscopy Science). Thin sections (80 nm) were obtained with a ultramicrotome, placed onto 300 mesh copper grids, and stained with saturated uranyl acetate in 50% methanol and then with lead citrate. The grids were viewed in a JEM-1200EXII electron microscope (JEOL Ltd, Tokyo, Japan) at 80 kV, and images were recorded on a XR611M midmounted 10.5-Mpixel CCD camera (Advanced Microscopy Techniques Corp, Danvers, MA).
Radiography
Thoracic radiographs were available for 1 animal (case No. 6). Images were taken in right lateral and dorsoventral recumbency with a Fuji X-ray machine (setting: 68 kVp, 75 mAs).
Results
Gross lesions were indistinct at necropsy but noticeable in affected formalin-fixed lung lobes as discrete multifocal areas of discoloration, distributed primarily at the periphery of the lobes, with irregular borders and a cream to light yellow tint (0.2-1.0 cm3). Some areas bulged slightly from the lung parenchyma, and some were contracted and consolidated. Upon microscopic examination, affected areas were characterized by intra-alveolar accumulation of fine to dense granular amphophilic material, with some presenting a strong eosinophilic rim, foamy alveolar macrophages, and ghost cell remnants (Figs. 1, 2). Inflammation of adjacent alveolar septa was not a prominent feature, but the interstitium was occasionally expanded by mild lymphocytic infiltrates. There was multifocal mild to moderate hypertrophy and hyperplasia of type II pneumocytes with variable interstitial fibrosis confirmed by Masson trichrome. The intra-alveolar material was periodic acid–Schiff positive and diastase resistant (Fig. 3). Presence of bacteria (Gram stain), mast cells (toluidine blue), and amyloid (Congo red) was ruled out. Using alcian blue (pH 2.5), some intra-alveolar deposits stained a very light blue, and some deposits were reactive to the counterstain, nuclear fast red. Oil red O stained the deposits with a reddish hue, indicating a lipid component. All samples had deeply basophilic round lamellar microcalcifications in different stages of development and numbers, placed frequently within alveoli but also within bronchioli, bronchi, and the lipoproteinaceous material.
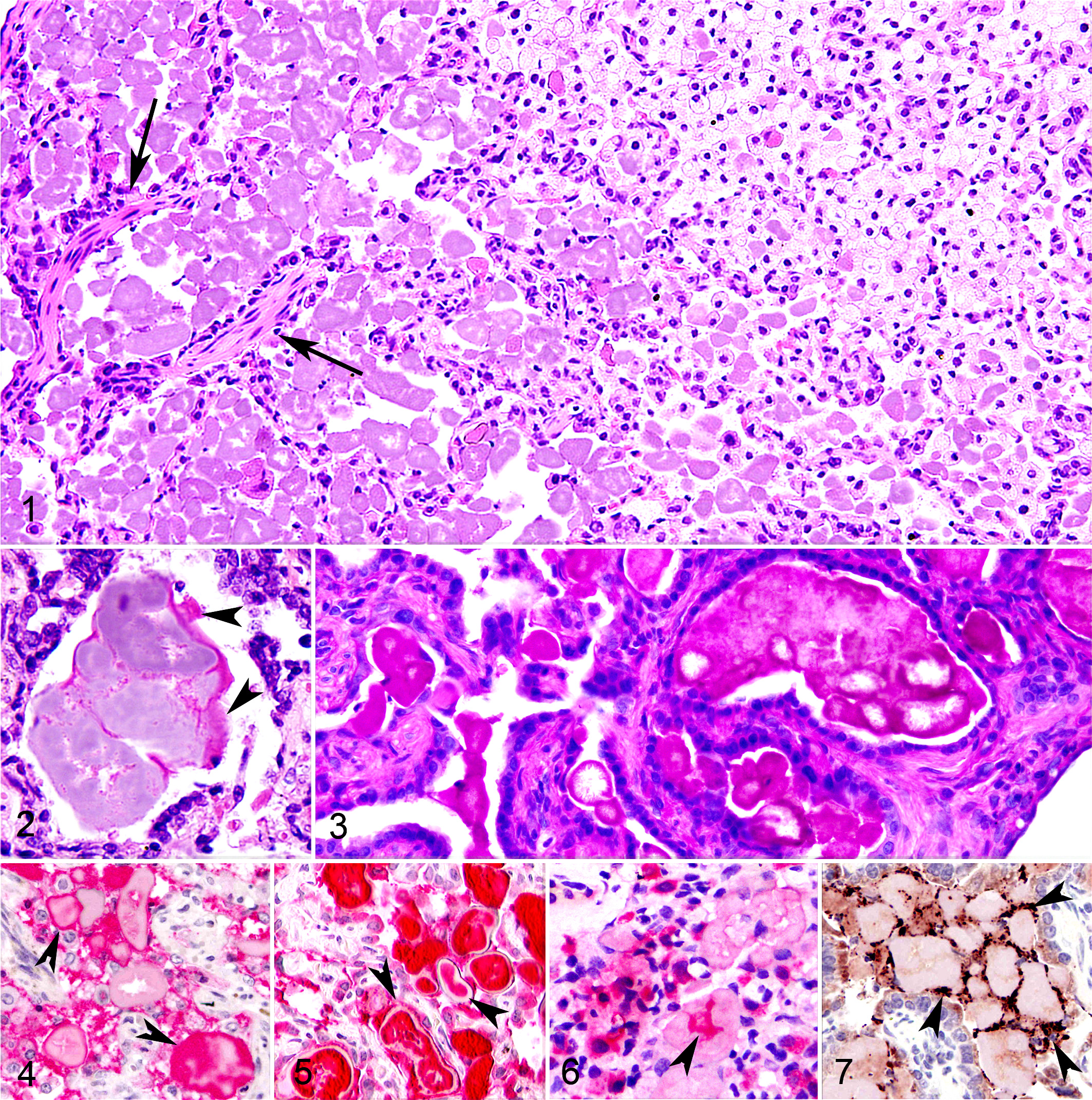
There were random foci of emphysema and atelectasis with mildly thickened pleura over affected areas. Pleural infolding was noted in peripheral lesions, associated with contraction and fibrous scarring (Fig. 3). Of the 7 animals, 4 exhibited discrete foci of osseous metaplasia.
The intra-alveolar deposits reacted strongly to SP-B in all lung samples, and it was the most abundant, followed by SP-A (Figs. 4, 5). For both SPs, in some cases either the periphery or the center reacted, and the rest remained unstained; free form was noted lining the alveoli and inside alveolar macrophages and type II pneumocytes. SP-C exhibited a strong reaction in type II pneumocytes, but the intra-alveolar material stained weakly (Fig. 6). SP-D reactivity was strong but limited to the periphery of the deposits; in type II pneumocytes, it was very weak (Fig. 7).
To establish a reference point in the ultrastructural features, normal lung tissues from a clinically healthy S. mystax (confirmed by light microscopy) were processed with affected animal samples for TEM examination. Compared to normal tamarin lung, the lung lesions in the tamarins were characterized by thickened alveolar septa consisting of large numbers of irregularly arranged collagen fibers, some fibroblasts, few type I pneumocytes, and numerous type II pneumocytes. Type II pneumocytes contained increased numbers of osmiophilic lamellar inclusion bodies in the cytoplasm, which were variable in size and staining intensity, abnormally shaped, and often coalesced (Fig. 8). Attenuation of type II pneumocyte surface microvilli and swelling of mitochondria and rough endoplasmic reticulum were observed. In some areas, the alveolar spaces contained large numbers of alveolar macrophages free in alveoli and large amorphous dense aggregates consisting of what appeared to be compacted surfactant and cellular debris. The alveolar macrophages were swollen and had numerous phagolysosomes containing amorphous rounded bodies or lamellar structures resembling type II pneumocyte lamellar inclusion bodies. These most likely represented ingested surfactant. TEM examination did not reveal a possible etiologic agent.
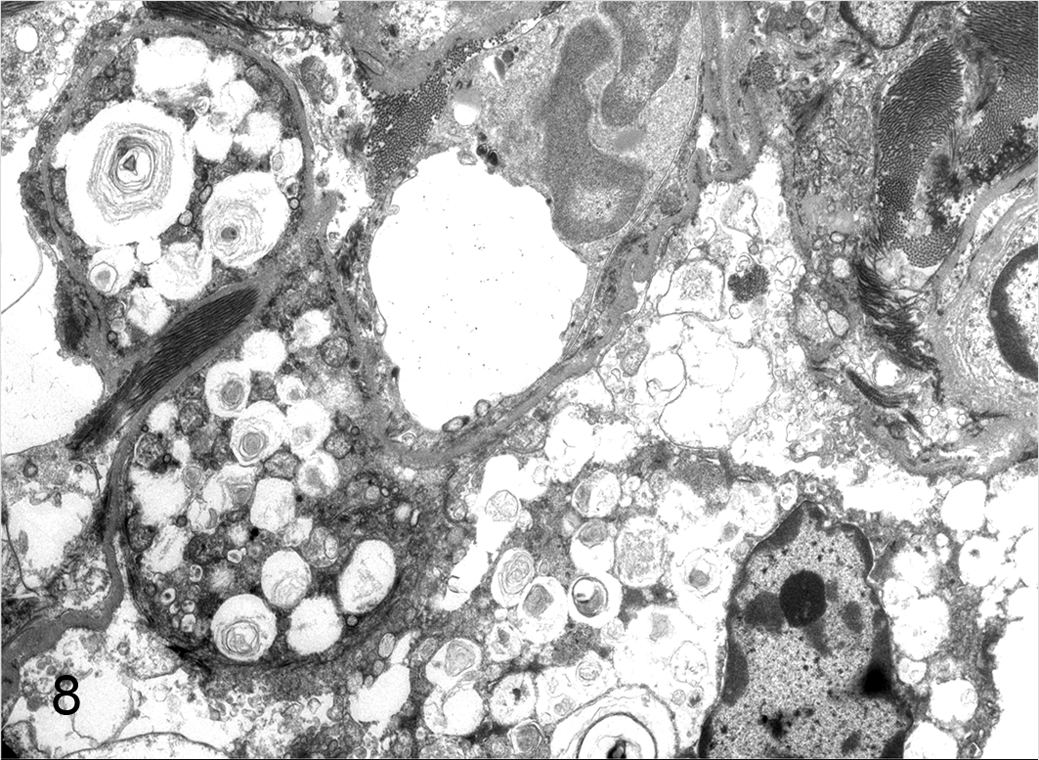
Lung; moustached tamarin, case No. 3. Type II pneumocytes showing variably sized, abnormally shaped, coalescing, lamellar inclusion bodies. Note capillary in center of the image. Transmission electron microscopy, uranyl acetate and lead citrate.
Thoracic radiographs available from 1 animal (case No. 6) showed randomly distributed small, patchy, radiopaque areas in the lungs (Fig. 9).
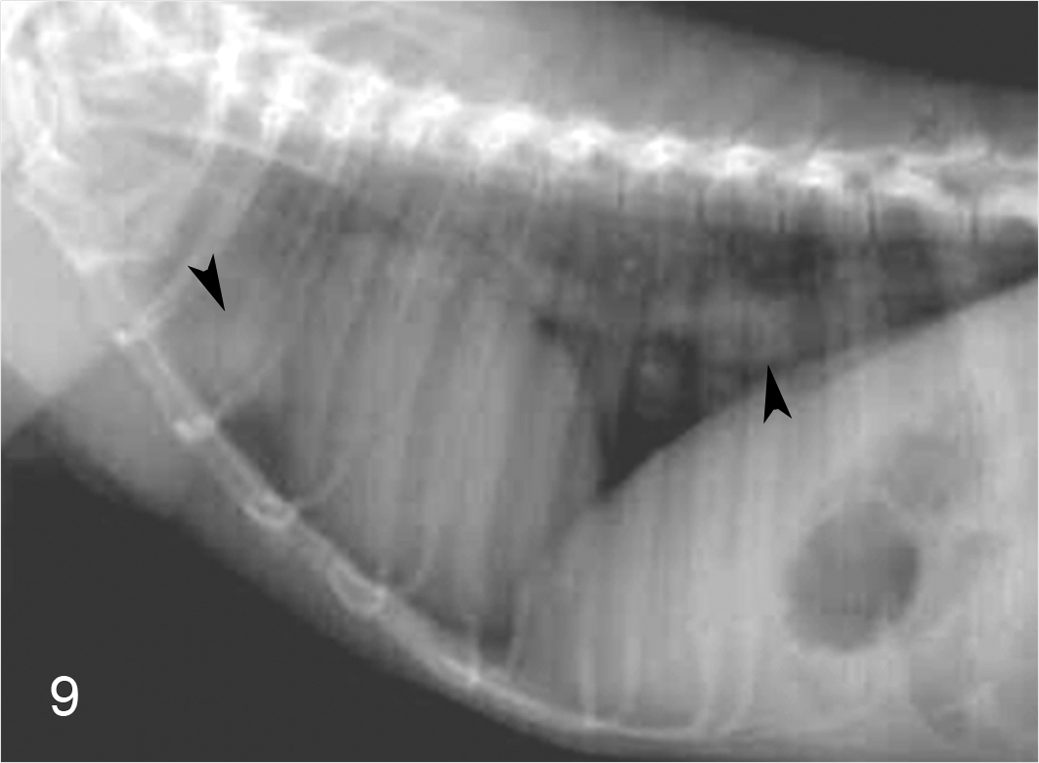
Lung; moustached tamarin, case No. 6. Left lateral thoracic radiograph showing discrete radio-opaque areas on cranial and diaphragmatic lung lobes (arrowheads). Radiograph.
Discussion
Human PAP was originally classified in 3 clinical forms: idiopathic, acquired or primary; secondary; and congenital. 13,17,21,25 However, it is more aptly described as a clinical syndrome caused by a heterogeneous group of disorders. 10,22 More than 90% of all cases of PAP are classified as a primary acquired disorder of unknown etiology. 7,14,21,26 Recently, investigators have proposed to classify the idiopathic form as autoimmune due to the finding of increased serum values of autoantibodies against GM-CSF. 3,13,21,25 GM-CSF is a potent stimulator of myeloid hematopoiesis 13 and is necessary for the terminal differentiation and function of alveolar macrophages, 3,23 which are responsible for clearance of surfactant from alveoli. 13,21,25
Secondary PAP develops with such conditions as immune deficiency syndromes, chronic inflammation, hematologic malignancies, pharmacologic immune suppression, inhalation of inorganic dust or toxic fumes, and some chronic infections, representing 5 to 10% of cases. 3,7,10,25 It was believed that the development mechanism of secondary PAP was unrelated to autoantibodies against GM-CSF, but 2 recent cases were reported in which people had elevated titers of autoantibodies against GM-CSF after exposure to industrial dust inhalation. 5,14
Congenital PAP is very rare, representing approximately 2% of cases. The disease manifests in the neonatal period and has very poor prognosis. 7 It is caused by rare gene mutations that include SP-B deficiency/mutation, SP-C mutations, GM-CSF receptor β or α chain abnormalities, and ATP-binding cassette transporter A3 (ABCA3) gene mutations. 3,10,13,22
We were unable to identify the trigger for development of PAP in the moustached tamarins. We hypothesized that experimental viral hepatitis might be related to the pathogenesis of PAP, since 5 of 15 animals enrolled in such studies presented with the lesions. An environmental factor was also considered as a possible cause due to the high incidence (33.33%) of PAP in these 15 animals; thus, secondary PAP was postulated and a genetic component considered (captive-born twins developed the disease). Finding 2 of 9 research-naïve animals (22.22%) with PAP housed in a different location downplayed the importance of the virus as an etiologic factor and encourages consideration of a secondary origin.
Although acquired or immune-mediated PAP represents 90% of all reported human cases, 7,13,21 the incidence of this clinical form has been estimated to be 3.7 per million of population. 12 In experiments in which the secondary clinical form is induced following exposure to a noxa that impairs the function of alveolar macrophages, the accumulation of varying amounts of surfactant is present in all exposed animals, which supports our hypothesis of secondary PAP in tamarins. 10,24
The clinical manifestations of the disease in humans are nonspecific respiratory symptoms, including dyspnea, cough, chest pain, fatigue, and weight loss, and, in some cases, low-grade fever. 13,22 None of these signs were noted in the tamarins included in this report except in case No. 3, which had an annotation in its medical record of abnormal breathing and nasal discharge 3 years before its death (Table 1). However, this symptom is nonspecific and accompanies many respiratory diseases. 16 A male preponderance in developing PAP has been suggested in the literature. 7,12,13,19,21,22 We cannot assert this in tamarins due to the small number of cases we studied. However, it is worth noting that 5 males and 2 females were affected.
Case No. 6 presented monocytosis and basophilia, both of which may be present in certain myeloproliferative disorders, 15 as listed as cause for secondary PAP; 3,10,12 even though this animal was not evaluated to confirm or discard such affection, we consider this a noteworthy fact.
We followed the work of Rosen et al in confirming the nature of the material in alveoli. 19 Masson trichrome and elastic van Gieson stains demonstrated mild to marked multifocal interalveolar septal thickening due to collagen deposition. Periodic acid–Schiff stain revealed the amorphous alveolar material as intensely positive and resistant to diastase digestion, although globular areas were unreactive (Fig. 3), resembling what has been reported in the literature. 10 With alcian blue (pH 2.5), the reaction was a very pale light blue, indicating a low amount of carboxylated and sulfated acid mucopolysaccharides and glycoproteins. 4
Marked interstitial fibrosis, also observed in humans with PAP, 9,13,19,22 was present in 2 tamarins (case Nos. 2 and 4). Lung fibrosis has been described in rodents exposed experimentally to silica dust to produce secondary PAP. 9 Cholesterol crystal clefts within the eosinophilic material in the alveoli have been occasionally reported in humans, but this was not observed in the tamarins. 5,7
In normal lungs, a thin layer of surfactant lines the alveolar surface and reduces surface tension, preventing collapse of the lung. In humans, surfactant is composed by lipids (90–95%) and proteins (5–10%; SP-A, SP-B, SP-C, and SP-D). 12,18 SP-A and SP-D are large hydrophilic collectin proteins involved in host defense, whereas SP-B and SP-C have a small molecular weight, are hydrophilic, and are involved in maintaining the surface tension in the air-liquid interface. 18 In human PAP, the accumulation of surfactant has been shown to be due to lack of clearance of all 4 SPs and precursors of SP-B by alveolar macrophages and to an abnormal secretion of transport vesicles containing precursors of SP-B. 2 The dynamics of the interaction among the different SPs and their role in human PAP have been extensively reviewed in the literature. 1–3,18
For immunohistochemical identification of the 4 SPs, titration runs were performed using tamarin lung tissue processed under optimal circumstances; within 48 to 72 hours postfixation in 10% NBF, type II pneumocytes and alveolar macrophages in control tissues were positive for all SPs. Affected animal samples were not kept in 10% NBF under optimal conditions, but we obtained consistent staining of the lipoproteinaceous material; however, this was not the case for type II pneumocytes and alveolar macrophages, in which the staining was either strong, weak, or absent. Since our study was not controlled, we cannot interpret the staining reactivity in these cells. Based on our observations, SPs contained within the accumulated surfactant withstands long fixation time (> 1 year) in 10% NBF.
Upon immunohistochemical examination, the strong eosinophilic areas present in some of the lipoproteinaceous aggregates (Fig. 2) reacted strongly against SP-D (Fig. 7). There are 2 reports of similar findings in humans, in which the intensely eosinophilic coarse granules within the fine granular substance in the alveolar spaces reacted positively to SP-D and were negative to SP-A and KL-6, a mucin-like glycoprotein that is expressed in type II pneumocytes. 14,17
Ultrastructural analysis of tamarin lungs by TEM were consistent with previous reports in humans with PAP where the lesions are characterized by amorphous electron-dense material in alveolar spaces and alveolar wall thickening, due to increased amounts of collagen and type II pneumocyte hypertrophy and hyperplasia, with numerous cytoplasmic osmiophilic lamellar bodies, some irregularly shaped. 22 Intra-alveolar macrophages were enlarged, containing numerous phagolysosomes with irregularly shaped and variably sized osmiophilic lamellar bodies resembling ingested surfactant.
The pattern of opacities observed in the thoracic radiographs of case No. 6 were nonspecific. Radiographic findings in PAP have been described as ground glass opacities and areas of consolidation in the lungs, but this pattern of diffuse lung disease is not exclusive and is seen in other conditions. 7,10,12,16
Animal models include mice deficient in GM-CSF, which develop lung lesions similar to PAP in humans. 6,23 A notable difference is the extensive lymphoid hyperplasia, predominantly B cells, around lung airways and blood vessels. This characteristic has not been described in humans, and we did not find this in tamarins either. Recently, PAP has been experimentally reproduced in cynomolgus monkeys by intravenous injection of patient-derived GM-CSF autoantibodies after immunosuppression with rituximab and cyclophosphamide. 20 Other experimental animal models include rodents in which lesions similar to PAP were reproduced by inhalation of inorganic dusts. 5,24
Additional lesions noted on microscopic examination in these animals were colitis cystica profunda (4 of 5; gastrointestinal tract of 2 animals were unavailable), cardiac hypertrophy and fibrosis (7 of 7), and chronic nephropathy (6 of 7). Mild to moderate subintimal thickening of pulmonary arteries concomitant with heart disease were present in 4 animals. One animal (case No. 4) had a pentastomid nymph in the lung.
Major advances in understanding the pathogenesis of human PAP have been achieved in recent years. However, basic questions remain about its pathophysiology and the extent to which environment and genetics play as factors in the disease. Based on our observations and the similarities of human and tamarin PAP, S. mystax could be a suitable animal model for the study of this disease. To our knowledge, there are no reports of spontaneous PAP in animals.
Footnotes
Acknowledgements
This study was supported by the Intramural Research Program of the National Institutes of Health, National Institute of Allergy and Infectious Diseases (NIAID), Comparative Medicine Branch, the Office of Research Services, and a NIAID contract to SoBran Inc. We thank Dr Robert Purcell and Dr Sue Emerson for kindly letting us use tamarin tissue samples from their previous studies and Dr Richard Herbert for providing Saguinus mystax radiographs and tissue samples.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.