
Abstract
Late thrombosis of coronary drug-eluting stents is an infrequent but serious complication of percutaneous transluminal coronary angioplasty. The best predictor of this event is the lack of endothelialization of stent struts. The objective of this study is to characterize and quantify the time course of endothelialization of different stents implanted in nonatherosclerotic swine coronary arteries. Thirty-three Carbofilm-coated stents were implanted percutaneously in 11 anesthetized domestic, crossbred pigs (weight 25 ± 3 kg, 2 months old). Each animal received 1 stainless steel stent (SS), 1 cobalt-chromium stent (CCS), and 1 tacrolimus-eluting stent (TES) in each coronary artery. Follow-up periods were 1 day (n = 9 stents), 3 days (n = 9 stents), and 7 days (n = 15 stents). Longitudinal sections of the stented vessels were examined using scanning electron microscopy. At 1 day, there was scarce, patchy endothelialization with areas of fibrin; the endothelialization rate was similar for all the stents (SS, 29% ± 23%; CCS, 29% ± 24%; TES, 31% ± 25%; P = .9). At 3 days, there were more endothelial cells but with immature features and giant cells over fibrin; the endothelialization was greater in SS and CCS than in TES (SS, 79% ± 14%; CCS, 81% ± 17%; TES, 46% ± 9%; P = .007). At 7 days, arteries showed better endothelialization with few giant cells; the endothelialization was greater in SS and CCS than in TES (SS, 95% ± 4%; CCS, 98% ± 4%; TES, 79% ± 9%; P = .01). In conclusion, the described model is useful for the analysis of endothelialization of coronary stents and facilitates measurement of its rate of formation and characterization of the involved cell types.
Keywords
Coronary stents are universally used in the percutaneous treatment of coronary artery disease. The major limitation of these devices is the development of a hyperproliferative response to vessel injury, causing restenosis in up to one third of the cases. The use of drug-eluting stents (DES) has reduced this rate of restenosis to single-digit figures.22,45,47 Nevertheless, DES have revived the fear of stent thrombosis, a potentially lethal complication,17,31 that had been previously reduced to rates below 2% after the generalized use of dual antiplatelet treatment.4,25 After the widely publicized controversy over a higher rate of stent thrombosis with DES, particularly regarding late (30 days to 1 year) and very late (1 year and beyond) stent thrombosis,7,36 different causal factors have been identified. One of these causal factors is a significant delay in the normal reendothelialization of DES-implanted arteries.10,11,19,21,28 The high antiproliferative power of the selected drugs eluted from current DES (eg, sirolimus, paclitaxel, everolimus, and zotarolimus) and their relative lack of cellular specificity may explain this issue. In addition, the polymers used in many of these devices may play an important role, being implicated as the cause of hypersensitivity reactions, delamination, and endothelial dysfunction.1219,29,48
DES have undergone a thorough efficacy analysis in different animal models. 34 The swine coronary arteries are the preferred model because of their similarity to the human anatomy and their suitability to analyze the restenosis induced by overstretch injury.40,41 One month after the implantation, the swine arteries show a restenosis response similar to that observed in humans at 6 months.
However, there is disparity between nonclinical and clinical rates of reendothelialization. Although 1 month after the implantation, the stent endothelialization may be complete in animals,2,12,21 observations from human necropsies show these stents may not fully endothelialized even several years after implantation.10,19,28
These differences between the animal model and humans led us to carry out this study with the following objectives: to create an endothelialization calendar for the struts of different stents in a swine model with normal coronary arteries and to characterize the cellular response that these devices trigger using scanning electron microscopy (SEM).
Methods
Animal Model and Procedure
Eleven animals were used to assess the progress of endothelialization, selecting 3 different follow-up periods: 1 day (3 animals), 3 days (3 animals), and 7 days (5 animals). The animals (domestic pigs, Large White race) were selected from the experimental farm of our university. They were 2 months old with a mean weight of 25 ± 3 kg. All the experimental procedures and animal handling were conducted according to the European and local general directives for the protection of experimental animals (Directive 86/609/CE, R.D. 223/1988) and under the supervision of the bioethics committee of our university. The animals were pretreated with clopidogrel (300 mg) and aspirin (325 mg) 1 day before the procedure. After the procedure, the animals received aspirin (100 mg) and clopidogrel (75 mg) throughout the study period. This dual antiplatelet treatment is the recommended protocol used in humans.
The surgical and intravascular procedures were performed as described previously: 32 the animals were sedated with a combination of ketamine (5 mg/kg), midazolam (0.5 mg/kg), and atropine (0.04 mg/kg) by intramuscular injection. Subsequently, propofol (4 mg/kg), atracurium besylate (0.5 mg/kg), and fentanyl (2 mg/kg) were administered intravenously to achieve the appropriate grade of anesthesia verified by the absence of a limb withdrawal reflex. After the intubation, the anesthesia was maintained with isoflurane 1.5 to 3.0% (1.5 L/min). A 7F introducer sheath was inserted into a carotid artery by surgical cut down. Heparin (200 IU/kg) was administered intravenously. A 40-cm, 6F-modified AL1 guiding catheter (Cordynamic-Iberhospitex S.A., Barcelona, Spain) was placed into both coronary ostia under fluoroscopic guidance. Heart rate, blood pressure, and electrocardiogram (ECG) were monitored throughout the procedure.
Implantation of Stents
The premounted, balloon-expandable stents were supplied by the manufacturer (CID Carbostent & Implantable Devices [formerly Sorin Vascular Therapy] s.r.l., Saluggia, Italy), and the implantation was performed at our institution.
Three different stents were used: (1) stainless steel stent (SS; Tecnic), 100-μm strut thickness; (2) cobalt-chromium alloy stent (CCS; Chrono), closed-cell design, 80-μm strut thickness; and (3) tacrolimus-eluting stent (TES; Carbostent DES), based on the stainless steel stent with 110-μm strut thickness, polymer free, with abluminal reservoirs loaded with 2.3 μg/mm 2 tacrolimus. All the stents were coated with a high-density turbostratic carbon film (Carbofilm coating) and were highly biocompatible and thrombo-resistant.3,32,37 Tacrolimus is a macrolide produced by Streptomyces tsukubaensis with strong immunosuppressive actions. 24 It is highly lipophilic and traverses the cell membrane without dependence on cell surface receptors. The intracellular receptors or immunophilins are the FK binding proteins (FKBP, including FKBP12). The T-immunophilin complex binds with high affinity to inhibit the calcineurin-calmodulin complex. 15 It inhibits platelet and neutrophil recruitment, expression of endothelial adhesion molecules, and free radical and inflammatory cytokine release. 46
The stents were implanted according to a predetermined scheme (random block design) in each coronary artery: right coronary, left anterior descending, and left circumflex. Every animal received a SS (3.5 mm diameter, 15 mm length), a CCS (3.5 mm diameter, 16 mm length), and a TES (3.5 mm diameter, 15 mm length) in the proximal segment (at less than 5 mm away from the origin) of each coronary artery. All stents were deployed at nominal pressure (9 atm), allowing a higher pressure in a second inflation if the relation to the vessel was less than 1.1 to obtain light-to-moderate injury (10–20% overstretch). The stent-to-artery ratio was analyzed in the postimplantation angiographic images.
Analysis and Sample Processing
Euthanasia was performed according to the follow-up protocol. The animals were sedated with a single intramuscular dose of azaperone (2 mg/kg), with subsequent intravenous administration of heparin (400 IU/kg) and euthanasia agent T-61 (InterVet, Salamanca, Spain) with embutramide, mebezonium iodide, and tetracaine at a dose of 0.3 ml/kg. Immediately after euthanasia, the hearts were harvested and the coronary arteries were perfused in situ with phosphate-buffered saline (PBS) and then fixed with 10% neutral-buffered formalin at 60 to 80 mm Hg. After 24 hours, the vessels were carefully excised from the heart and bisected longitudinally under a dissecting microscope.
Both halves were processed for scanning electron microscopy to analyze the endothelialization as described elsewhere. 9 The luminal surfaces of the bisected halves of each stent were examined en face in a JSM-6480 LV (JEOL, Tokyo, Japan) scanning electron microscope, obtaining low-power digital images (25×) and details of characteristic areas with higher magnification (200–1000×). The adequate discrimination of endothelial cells was based on morphological features: polygonal cells with distinctive limits between them, prominent nuclei and irregular size, highly orientated and exhibiting a cobblestone-like phenotype, and appearing as a confluent flattened monolayer. 30 Other cell types were characterized regarding their size and morphological aspects (Fig. 1). Lymphocytes (7–8 μm) have numerous microvilli on their surface; monocytes (15 μm) are covered by a number of surface folds and projections of variable size; neutrophils (10–12 μm) show a number of shallow surface folds. Nevertheless, the accurate discrimination of the cellular type can be hard because, in some cases, monocytes closely resemble neutrophils, 6 and even neutrophils and at least some monocytes are not readily distinguishable from lymphocytes by SEM.1,50,51 The referred cellular size is orientative because the critical-point drying procedure for SEM can reduce the cellular diameter. 39
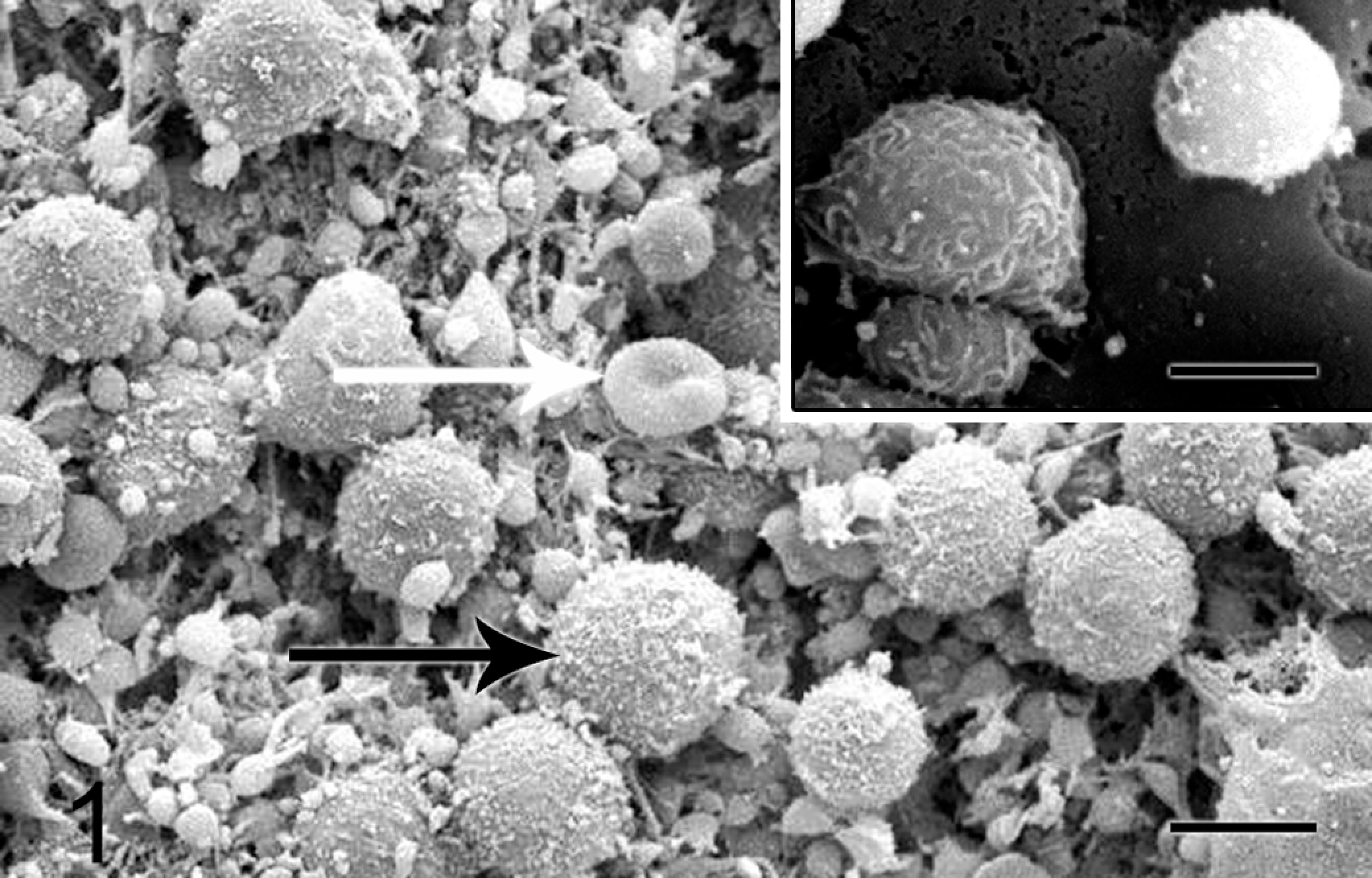
Characterization of the overlining material: on a mat of fibrin and platelets (small rounded cell fragments), presence of lymphocytes (<8 μm with surface microvilli, black arrow) and red blood cells (characteristic concavity, white arrow). Neutrophils (left in the inset) show shallow surface folds and are bigger (10–12 μm) than lymphocytes (right in the inset). Bars = 5 μm.
The ImageJ 1.4 software (National Institutes of Health, Bethesda, Maryland) was used to quantify the endothelial coverage of the stent. To calculate the total stent area, the whole luminal surface of the artery was measured in each sample and then corrected by the ratio of metal to artery supplied by the manufacturer (SS 14.3%, CCS 12.5%, TES 17.5%; Fig. 2). The nonendothelialized area over the struts was measured. We calculated the rate of endothelialization (%E) using the following formula: %E = 100 × [1 – (nonendothelialized area/total stent area)].

To calculate the stent area in each specimen, the whole luminal surface covered by the stent was measured (area enclosed with the black outline) corrected for the metal-to-artery ratio. The nonendothelialized area over the struts includes white areas (uncovered struts) + black areas (struts covered by fibrin/giant cells). Bar = 1 mm.
Statistical Analysis
The variables are presented as mean ± standard deviation. Data were analyzed for overall differences among different stents and follow-up periods using one-way analysis of variance (ANOVA). Probability values of P < .05 were considered significant.
Results
All the animals survived the stent implantation procedure and completed the scheduled follow-up period. In total, 33 stents were deployed (9 in the 1-day group, 9 in the 3-day group, and 15 in the 7-day group), achieving a final stent-to-artery ratio of 1.16 ± 0.06 without differences between stents (SS, 1.17 ± 0.06; CCS, 1.16 ± 0.07; TES, 1.16 ± 0.07; P = .87). The mean deployment pressure (atm.) was also similar for the 3 groups: SS, 9.4 ± 1.8; CCS, 9.3 ± 0.9; and TES, 9.4 ± 1.8 (P = .97). There were no episodes of subacute stent thrombosis. One animal developed infection of the surgical wound without further consequences. All samples were adequately analyzed except one stent (7-day group) showing a drying artifact that precluded the characterization of the different cellular types over the stent. Although the endothelialization of the stent struts in the edges (both proximal and distal) seemed to be better than those in the middle part, no significant differences were detected. No relation was found between the endothelialization rate and the treated artery, the deployment pressure, or the stent-to-artery ratio.
Results at 1 Day (Fig. 3)
The greater part of the stent structure appeared naked or covered by a thin layer of fibrin, platelets, and inflammatory cells. The latter were also present in a moderate amount around the stent struts. The vessel surface between struts showed preserved endothelium. The stent reendothelialization showed a patchy distribution: isolated endothelial cells began to cover the struts from the edges to the center. There were no differences (P = .9) in the endothelialization rate between the SS (29 ± 23%), CCS (29 ± 24%), and the TES (31 ± 25%).
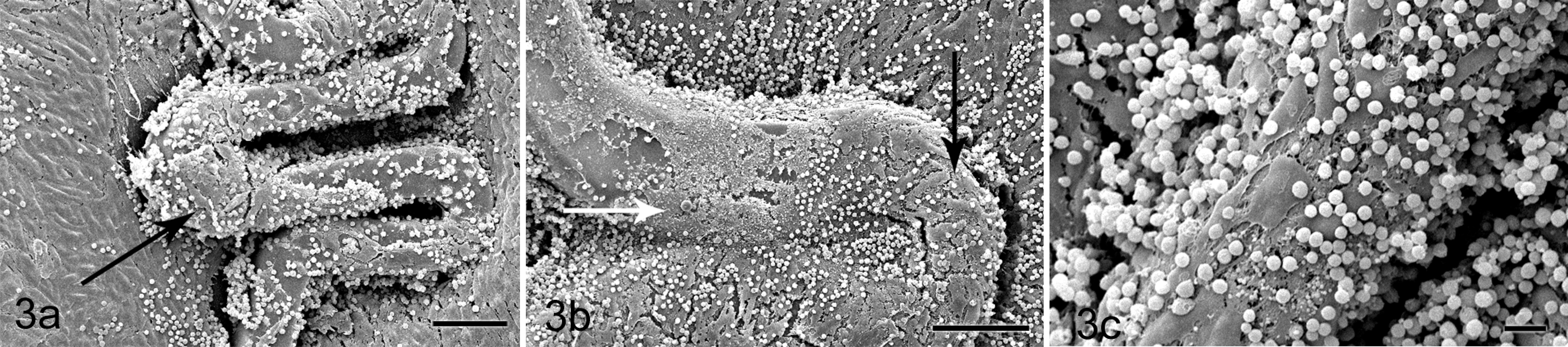
Day 1. (a) Sparse endothelial cells begin to cover the stent struts from the edges (black arrow). Bar = 100 μm. (b) The metallic surface of the stent appears mostly naked, with some areas covered by fibrin (white arrow). Bar = 100 μm. (c) Abundant inflammatory cell component. Bar = 20 μm.
Results at 3 Days (Fig. 4)
More struts showed coverage by endothelial cells, but features consistent with immaturity (eg, loose intercellular connections) were still present. Giant cells and other inflammatory cells and microthrombi were variably evident. The endothelialization rate of the SS (79 ± 14%) and CCS (81 ± 17%) was significantly higher than endothelialization of the TES (46 ± 9%, P = .007).
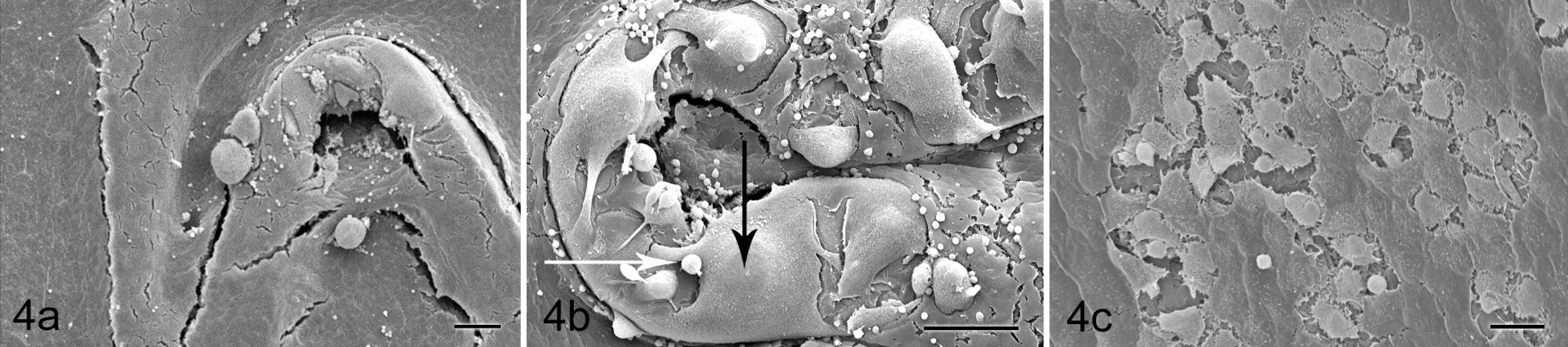
Day 3. (a) The endothelial layer covers a wider area with less inflammation. Bar = 100 μm. (b) Giant cells of different sizes and shapes are present over areas lacking endothelial cells (white and black arrows). Bar = 100 μm. (c) The intercellular connections appear loose. Bar = 20 μm.
Results at 7 Days (Fig. 5)
A homogeneous endothelial layer was observed covering most of the metallic structure of each device. Fibrin clusters or giant cells were observed over the few struts not covered by endothelial cells. The endothelialization rate of the SS (95 ± 4%) and CCS (98 ± 4%) was almost complete, whereas the TES showed a quite high rate (79 ± 9%) but significantly lower than the SS and the CCS (P = .01).
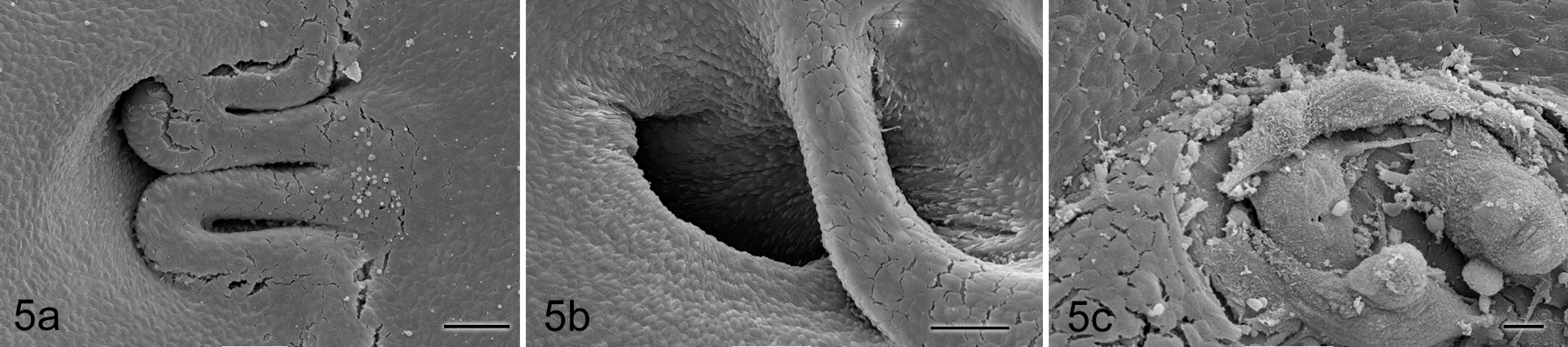
Day 7. (a) The endothelial layer is almost complete. Bar = 100 μm. (b) Endothelial cells are present even over stent struts not apposed to the vessel wall, floating over the origin of small side branches. Bar = 100 μm. (c) Wherever the endothelial cells do not cover the struts, giant cells and some fibrin can be observed. Bar = 20 μm.
Figures 6 to 9 depict and summarize the global endothelialization results at different time points.
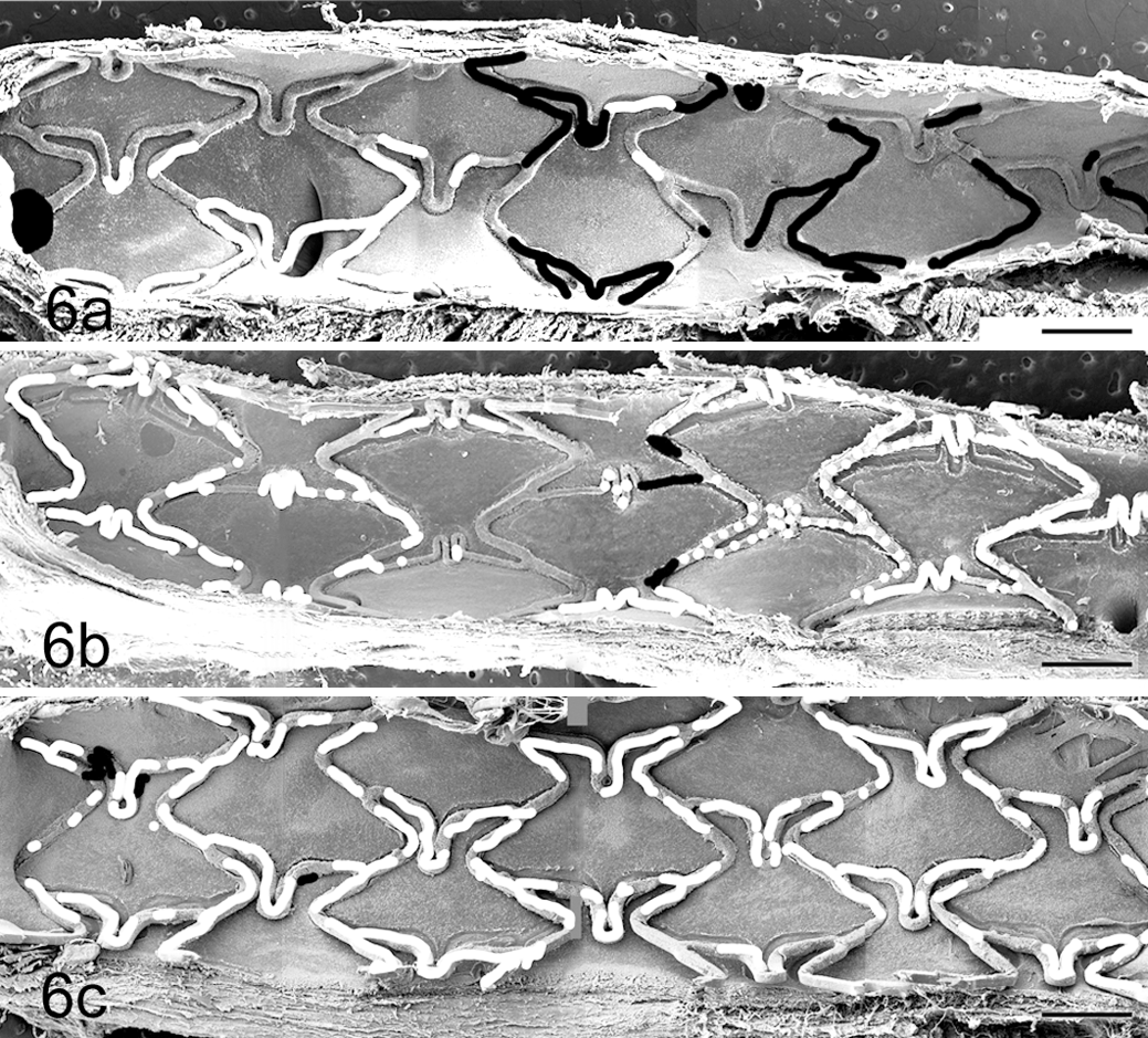
Comparison of endothelialization of the different stents at 1 day. (a) Stainless steel stents, (b) cobalt-chromium stents, and (c) tacrolimus-eluting stents. The endothelialization assessment is depicted with black and white areas over the images (white areas: uncovered struts; black areas: struts covered by fibrin/giant cells). All the stents are oriented in the same way: proximal segment to the left, distal segment to the right. Bars = 1 mm.
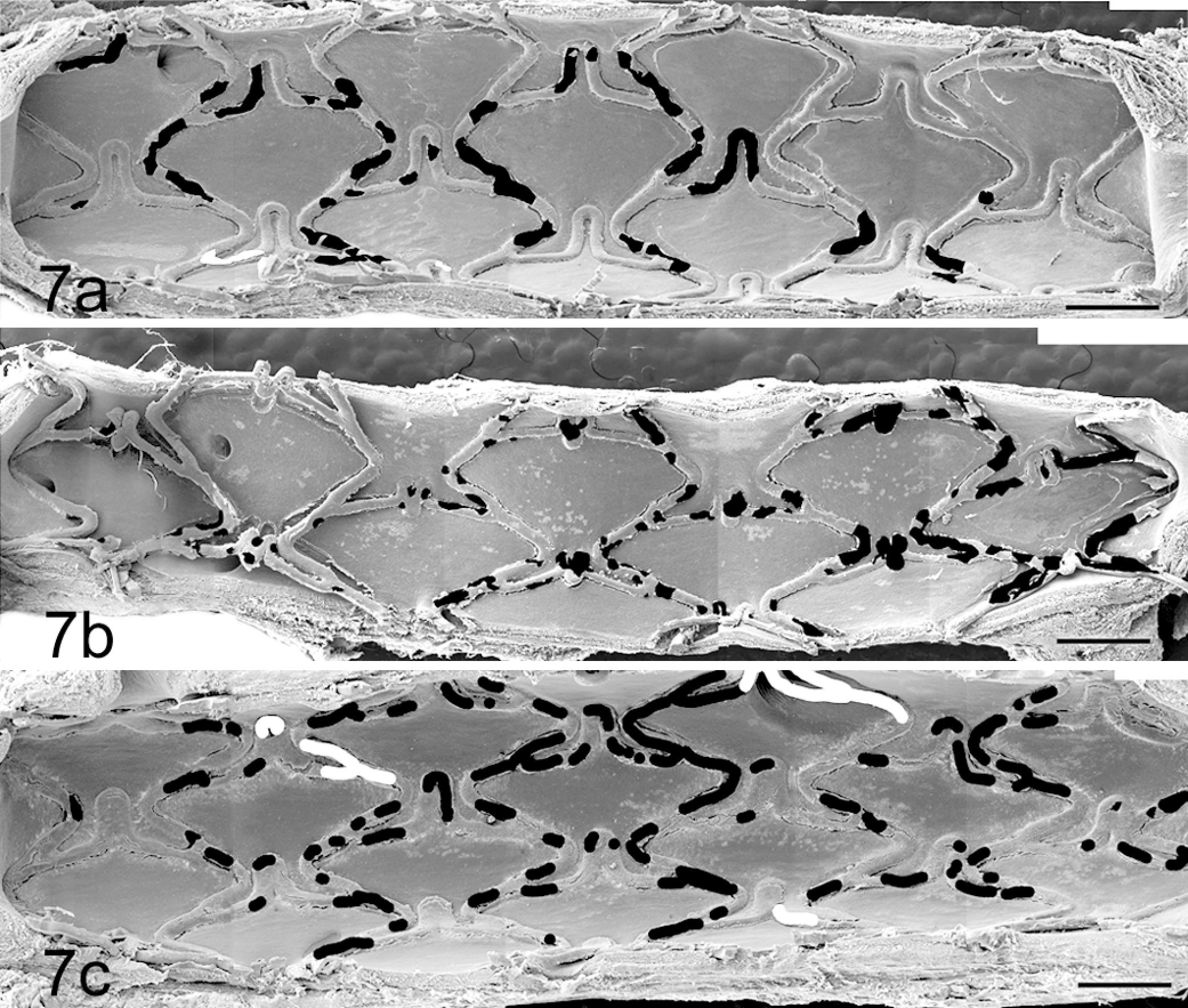
Comparison of endothelialization of the different stents at 3 days. (a) Stainless steel stents, (b) cobalt-chromium stents, and (c) tacrolimus-eluting stents. The endothelialization assessment is depicted with black and white areas over the images (white areas: uncovered struts; black areas: struts covered by fibrin/giant cells). All the stents are oriented in the same way: proximal segment to the left, distal segment to the right. Bars = 1 mm.
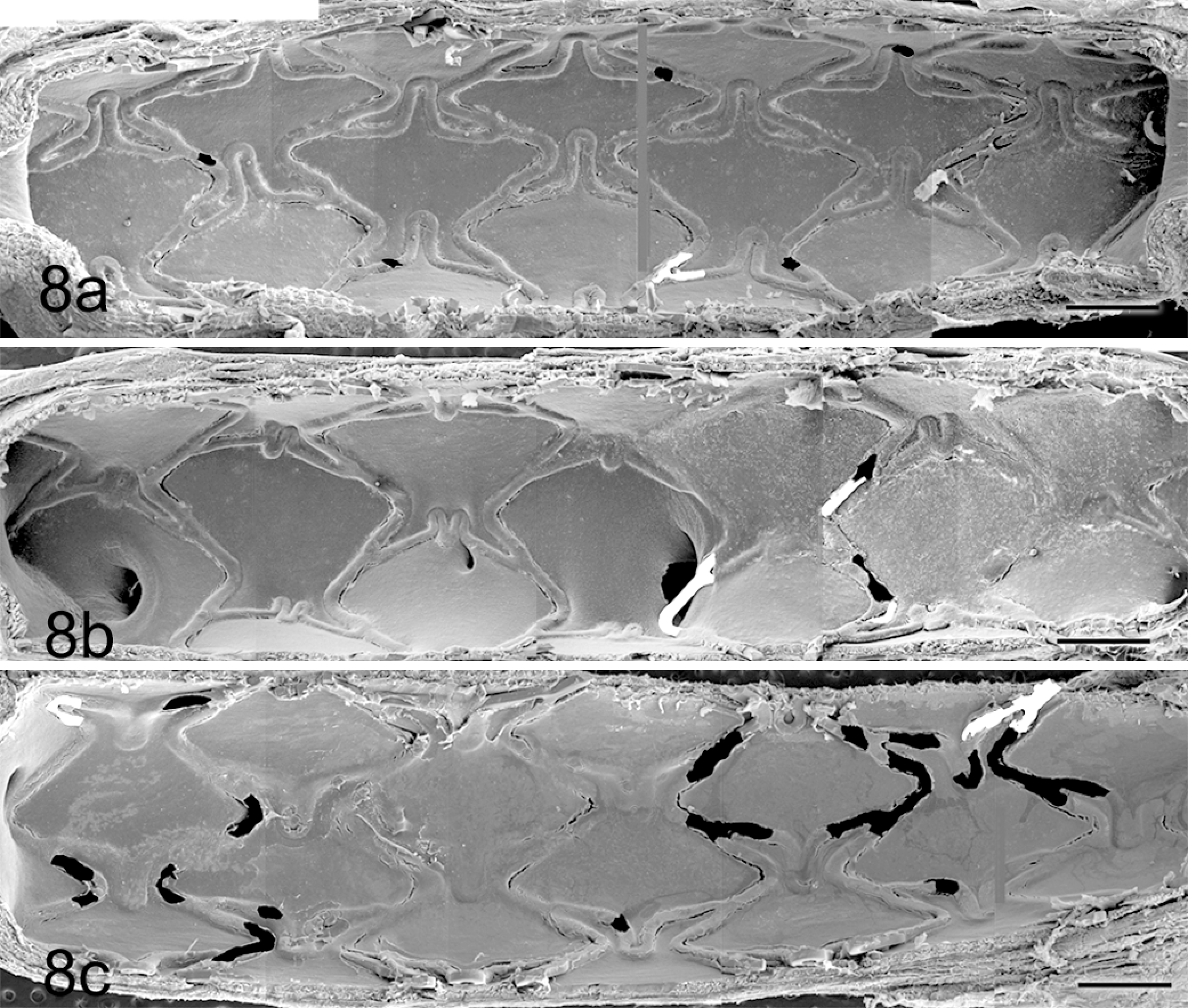
Comparison of endothelialization of the different stents at 7 days. (a) Stainless steel stents, (b) cobalt-chromium stents, and (c) tacrolimus-eluting stents. The endothelialization assessment is depicted with black and white areas over the images (white areas: uncovered struts; black areas: struts covered by fibrin/giant cells). All the stents are oriented in the same way: proximal segment to the left, distal segment to the right. Bars = 1 mm.
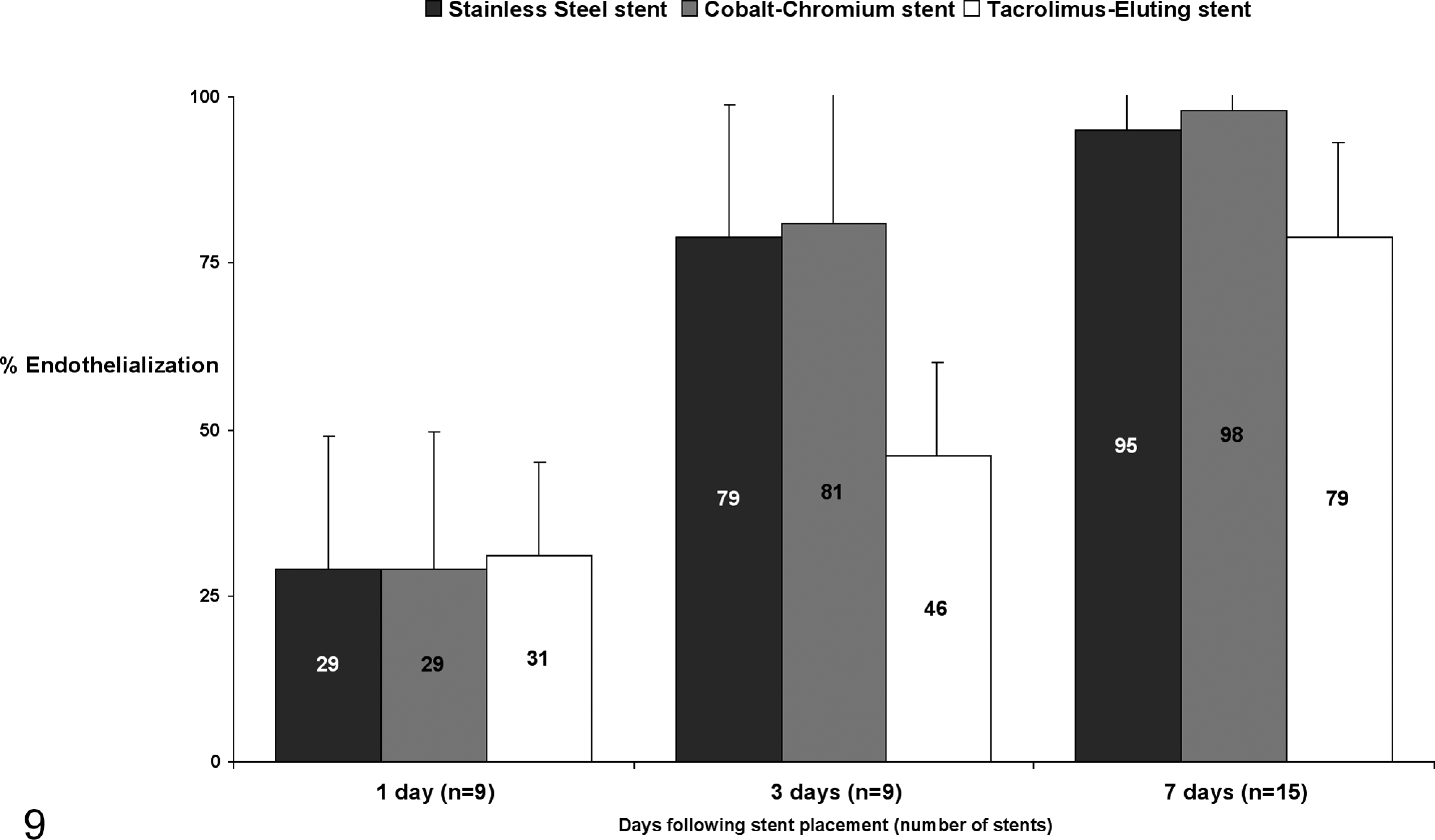
Bar chart. % Endothelialization of the stents at different time points.
Discussion
The results of this study prove the described model as a useful tool to construct an endothelialization calendar for different stents and to characterize the elicited cellular response. Our key findings are the complete endothelialization of the bare metal stents in 7 days (without differences between the SS and the CCS, although they clearly differ in the strut thickness), the acceptable but significantly lower endothelialization rate of the TES, and the gradual decrease of the inflammatory response.
In our model, the bare metal stents (SS and CCS) show almost complete endothelialization at 7 days. Finn et al 12 have found a similar rate of endothelialization after 14 days in a swine model with different cobalt-chromium stents. A complete endothelialization of these stents was not observed until 28 days after the implantation in the rabbit iliac artery model.12,21 Different susceptibility and reactivity to vascular injury between animal species and structural differences between iliac and coronary arteries may explain the differences between the results obtained in swine and rabbits.40,41,49 The discrepancy between our results and previous data in swine12,21,27 could be explained by some methodological differences such as greater endothelial denudation caused by previous balloon inflation and by the potential “pro-healing” role of the Carbofilm coating.3,32,37 The achieved stent-to-artery ratio could also be a key factor in the different studies. Finn et al 12 do not detail the achieved ratio in their swine group. Higher overstretching causes greater vessel injury and, consequently, more restenosis;13,42 it is not clear if greater injury also correlates with faster reendothelialization.40,41 To avoid a potential hyperproliferative reaction, only light-to-moderate oversizing of the stents was performed.
The endothelialization rate of the TES (Carbostent DES) at 7 days (79 ± 9%) compares favorably with previous results, although methodological differences render this comparison quite difficult. 35 Joner et al 21 described the endothelialization rates of different DES at 14 days in the rabbit iliac model: 64 ± 27.5% (everolimus-eluting stent), 30.2 ± 14.2% (zotarolimus-eluting stent), 26.8 ± 15.8% (paclitaxel-eluting stent), and 6.4 ± 4.2% (sirolimus-eluting stent). Only at 28 days did they observe endothelialization rates more than 60% in the sirolimus, paclitaxel, or zotarolimus stents. Nevertheless, other authors have demonstrated complete endothelialization in the swine coronary model with paclitaxel-eluting stents at 20 days, with a high endothelialization rate at 10 days. 2 Therefore, the different animal models and methodologies make it difficult to establish direct comparison between the results.
A principal objective of this study is the characterization of the cellular response that the stents elicit. One day after the implantation, the stent is mainly uncovered or covered by a thin layer of fibrin and platelets, with a moderate inflammatory reaction. At 3 days, the predominant cell type is inflammatory, including lymphocytes, macrophages, and few multinucleated giant cells. The presence of giant cells in particular has been previously reported, but their role in the endothelialization process remains unclear. 2 Nevertheless, the amount of giant cells is similar in the 3 groups. At 7 days, the nonendothelialized areas are covered by giant cells with sparse lymphocytes, monocytes, and neutrophils. Two aspects of the arterial response arise from these findings: (1) the evolution of the inflammatory response and (2) the contribution of different cellular and noncellular (eg, fibrin) structures to coverage of the stent struts.
The inflammatory response has been typically described in depth, surrounding the stent struts in the cross-sectional analysis of the artery.11,52 The luminal inflammation can also be assessed using SEM: bare metal stents show a decreasing inflammatory reaction with time, while DES show a persistent (even increasing) inflammatory reaction. 33 Nevertheless, the Carbostent DES showed an evolution of the acute to subacute inflammatory response to be similar to the bare metal stents. The absence of a polymer as drug vehicle and the high biocompatibility of the Carbofilm coating could explain this finding. The presence of nonendothelial structures over the stent implies some practical considerations. Different studies have used image techniques, such as optical coherence tomography (OCT)8,26 or angioscopy, 44 to analyze the endothelialization of the stent in vivo. All of them have focused the analysis on the detection of the uncovered struts. In light of our results and other previous data, 43 it is obvious that the presence of covered struts does not entail an adequate endothelialization.
Although the use of a young, healthy animal can be considered a limitation, it is the recommended model by the different consensus documents.40,41 The experts' recommendations suggest time periods shorter than 14 days to evaluate the endothelialization in the swine model. However, it is stated that “if confluent endothelium is present within 28 days of treatment of stent placement, this finding does not necessarily assure favorable human endothelial reaction. However, if the porcine model suggests substantial or long-term endothelial toxicity as manifested by incomplete endothelialization of the stent, this observation suggests but does not prove potential problems with vascular biological compatibility.” 40 Different models of disease (eg, diabetes, hyperlipidemia) are becoming increasingly popular for the evaluation of DES.520,35,38 They could provide vascular responses closer to human patients, but they are still not validated. Another potential limitation of the study is the lack of functional assessment of the endothelium. As some morphological features (loose intercellular connections) observed at 3 days suggest endothelial immaturity, endothelial function in addition to form is an important consideration in addressing DES safety. Different studies are evaluating endothelial functionality using immunohistochemical techniques12,18,20,27,38,52 or analyzing the in vivo vascular reactivity to different vasodilators, endothelium dependent or independent.14,16,23 However, the clear illustration and correlation of these results regarding endothelial form and function from a preclinical to a clinical setting have not been established. This is a critical deficit and emphasizes the importance of studies as the one presented herein to allow for better assessment of the safety of interventional devices for the treatment of coronary artery disease.
Conclusions
The described swine model with normal coronary arteries is useful to measure and compare the endothelialization of coronary stents, assessing their evolution and characterizing the involved cellular types. Future studies using this model should complete the information with the analysis of elicited inflammation, the assessment of the functionality of the observed endothelium, and the translation of preclinical results to clinical relevance.
Footnotes
The author(s) declared that they had no conflicts of interests with respect to their authorship or the publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Unrestricted research grant from CID Carbostent & Implantable Devices s.r.l., Saluggia, Italy.