
Abstract
A case of cardiac hamartoma in a 2-month-old squirrel monkey is reported. The monkey showed a loss of appetite and died suddenly. Microscopically, an encapsulated nodular lesion was found at the right atrial wall. The lesion consisted of irregularly shaped, slender myocytes intermingled with a few fibroblasts and collagen fibers. Neither nuclear atypia nor inflammatory cell infiltrate was seen. The constituting cells had stratified striations in the cytoplasm and reacted immunohistochemically for desmin, indicating the nature of myocytes. Based on the above findings, a diagnosis of cardiac hamartoma was made. This is the first case of cardiac hamartoma in this species.
Keywords
The term hamartoma refers to an excessive and focal noninvasive overgrowth of disorganized collections of tissue components native to the organ in which it occurs. 23 Hamartoma is considered to be congenital; therefore, the growth may cease when the affected organ reaches maturity. 23 The first description of cardiac hamartoma in humans was recorded in 1988. 26 To our knowledge, so far 22 cases of human cardiac hamartoma have been reported in the English literature, with the incidence being predominantly young men (Table 1). Histologically, human cardiac hamartomas consist of demarcated masses of irregularly shaped or hypertrophied mature myocytes with a variable amount of collagen fibers and fatty tissues; such myofibers in occasional cases show fibromuscular disarray resembling hypertrophic cardiomyopathy. 3 Human cardiac hamartoma preferentially develops in the ventricle wall and has occasionally been reported to occur in the atrium. 1 In veterinary medicine, cardiac hamartoma is rare; only one case of congenital cardiac hamartoma found in the right atrium of an 8-year-old female dog has been reported. 16 The present report describes histopathologic and immunohistochemical features of a cardiac hamartoma encountered in a squirrel monkey. This is the first case of cardiac hamartoma in this species.
Cardiac Hamartoma Reported in Humans a
a F, female; M, male; y, year; m, month; RV, right ventricle; LV, left ventricle, RA, right atrium; VS, ventricular septum; IS, interventricular septum; PI, pulmonary infundibulum; N/A, not available.
Case History and Necropsy Findings
A 2-month-old female squirrel monkey (Saimiri sciureus) (205 g in body weight) was presented to an animal hospital with a history of fever (38.6°C) and loss of appetite. The cause of such clinical signs was not determined at that time. The monkey suddenly died 1 week later, and a necropsy was performed. The lungs were highly congested; significant gross findings were not observed in other organs.
Histopathology and Immunohistochemistry
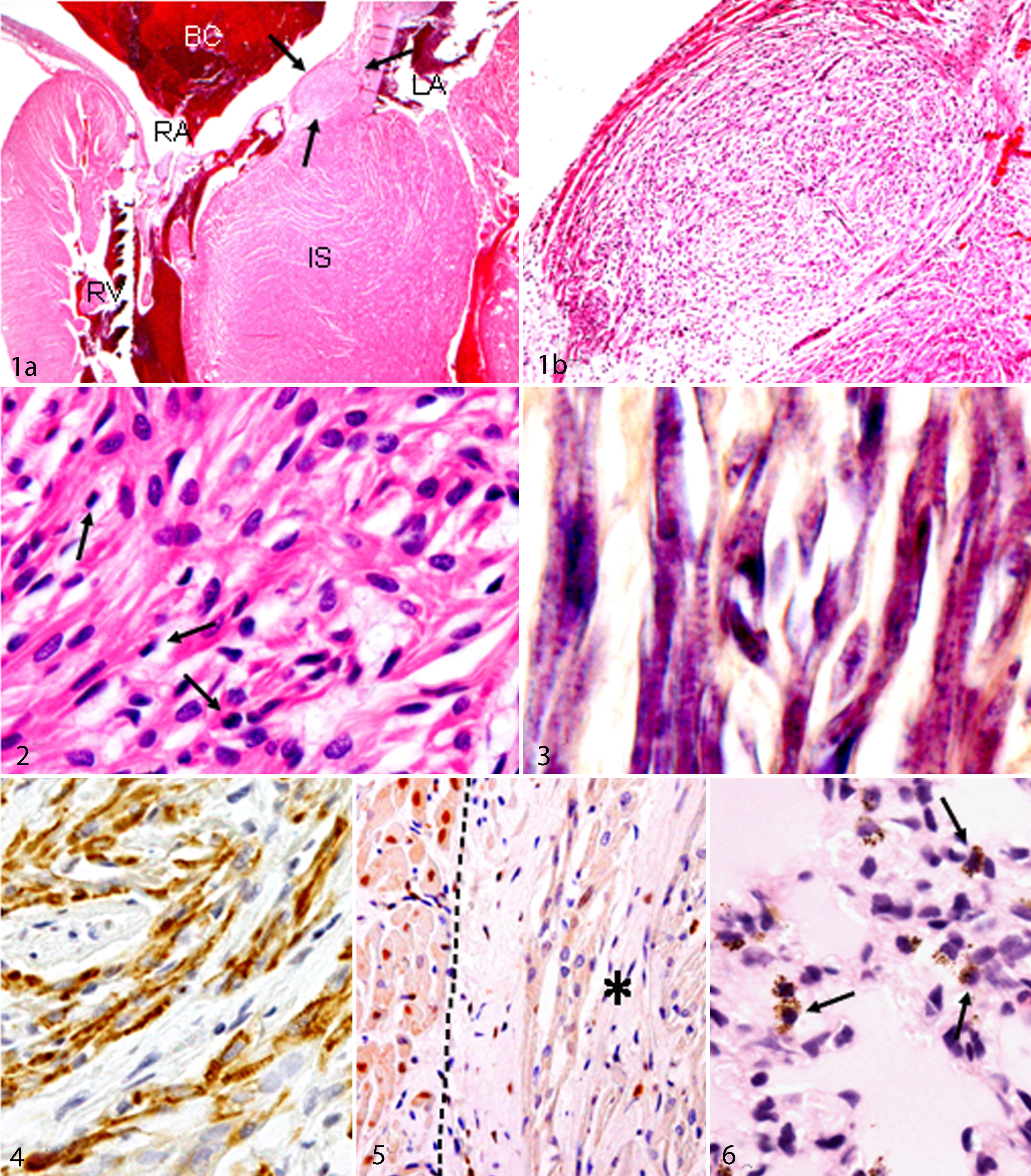
The heart, lungs, kidneys, liver, spleen, brain, stomach, and intestines were fixed in 10% neutral phosphate buffered formalin, which were routinely processed, embedded in paraffin, cut at 4 μm in thickness, and stained with hematoxylin and eosin. Immunohistochemical analyses were performed with mouse monoclonal antibodies against α-smooth muscle actin (α-SMA) (clone 1A4, 1:100), desmin (clone D33, 1:200), vimentin (clone V9, 1:400), Ki-67 (clone MIB-1, 1:100), and proliferating cell nuclear antigen (PCNA) (clone PC10, 1:400), as well as rabbit polyclonal antibody to S-100 (1:500)—all of which were purchased from Dakocytomation (Glostrup, Denmark). After deparaffinization, for antigen retrieval, sections for α-SMA immunohistochemistry were incubated with 10 μg/ml proteinase K for 10 minutes, and those for desmin, vimentin, PCNA, and Ki-67 immunohistochemistry were pretreated by microwave for 10 minutes in citrate buffer (pH, 6.0). These sections were incubated with 3% H2O2 in phosphate buffered saline for 10 minutes to quench endogenous peroxidase and then with 5% skimmed milk in phosphate buffered saline for 30 minutes to inhibit nonspecific reactions. The sections were reacted with each primary antibody for 14 hours at 4°C, followed by horseradish peroxidase–conjugated secondary antibody (Histofine Simple Stain MAX PO, Nichirei, Tokyo, Japan) for 30 minutes. Positive reactions were visualized with 3,3′-diaminobenzidine (DAB Substrate Kit, Vector Laboratories, Burlingame, CA). Sections were lightly counterstained with hematoxylin. As negative controls, tissue sections were treated with mouse or rabbit nonimmune serum instead of the primary antibody. Microscopically, a small nodular lesion (0.6 × 1.1 mm) was incidentally found at the right atrial wall, close to the junction between interatrial and interventricular septum (Fig. 1, arrows). The lesion consisted of irregularly shaped, slender myocytes arranged haphazardly, and it was encapsulated by a thin fibrous tissue; some myocytes had a hyperchromatic nucleus suggestive of the immature type of the cells (Fig. 2, arrows). Tissue sections stained with phosphotungstic acid hematoxylin clearly revealed the presence of stratified striations in the cytoplasm of constituting cells of the lesion; this finding was similar to that of normal cardiac muscles (Fig. 3), although the arrangement was more irregular in the lesion. A small amount of collagen fibers, demonstrable by the azan–Mallory method, was present throughout the lesion, accompanied with a few fibroblastic cells. Malignant features, such as nuclear atypia and necrosis or inflammatory cell infiltrate, were not observed. The majority of constituting cells reacted strongly for desmin (Fig. 4), and vimentin-positive cells were sporadically seen in the lesion. There were no cells positive for α-SMA or S-100. Interestingly, although there were a number of PCNA-positive and Ki-67-positive myocytes in the surrounding myocardium (indicative of maturing myocytes), cells positive for PCNA (Fig. 5) and Ki-67 in the lesion were much smaller in number. Other histopathologic findings included myocardial hypertrophy of the interventricular septum, severe edema, congestion, and appearance of hemosiderin-laden macrophages in the alveoli in the lungs (Fig. 6), lymphocyte depletion in the spleen, and submucosal edema in the stomach.
Discussion
Clinically, the presence of cardiac hamartoma could not be determined, and microscopically, the lesion was found incidentally. Therefore, heart function tests such as electrocardiogram and heart rate were not conducted. Human cardiac hamartomas have been a well-described association with arrhythmias—particularly, ventricular tachycardias. 25 Histopathologically, cardiac hamartomas in humans and a dog consisted of solitary and/or multifocal lesions of disorganized cardiac muscle cells interspersed by collagens and fatty tissues.1,3,16,18,26 By the desmin immunohistochemistry and phosphotungstic acid hematoxylin staining, the constituting cells in the present case were regarded as a myocyte origin. Although the constituting cells in the present case were more slender in shape and appeared to be immature, the irregular arrangement was similar to that reported in human and canine cases. Hamartoma is considered a lesion having the linkage between malformation and benign neoplasm. 23 The present case did not show any cellular atypia indicative of high malignancy. Rather, the number of proliferating cells, demonstrable by the PCNA and Ki-67 immunohistochemistry, was much smaller than that of surrounding normal myocytes.
The left ventricular wall is the predilection site for human cardiac hamartomas (Table 1). 1 However, some human cases have been reported to develop in the right ventricular wall, right atrium, or ventricular septum (Table 1). The present case and a canine 16 case reported earlier found hamartomas in the right atrium. Thus, cardiac hamartomas may occur at any place in the myocardium.
The present cardiac hamartoma was considered congenital because the affected monkey was young (2 months old). From the fetal period, the cardiac lesion might have developed in the right atrium; the location was close to the tricuspid and pulmonary valves. Mechanical hindrance of the tricuspid valves and stenosis of the pulmonary valves are associated with myocardial hypertrophy of the right ventricle, pulmonary hypertension, and hepatic congestion; 14 histologic findings suggestive of such abnormalities were absent in the present case. Intriguingly, interventricular septal thickening was observed, as well as edema and hemosiderin-laden macrophages in the lungs. These findings indicated left-sided heart failure. The present hamartoma, located in the right atrium, might have caused interference of the conduction system, which can lead to tachyarrhythmia and subsequently result in secondary heart failure. Such complicated functional failures of the heart might gradually progress, thereby resulting in the heart–lung circulation disturbance. A chain of these events were considered a cause of the sudden death of this monkey. Therefore, the hemosiderin-laden macrophages seen in the lungs might be regarded as “heart failure cells”; clinical pyrexia might be related to such pulmonary lesions. 17
Differential Diagnosis
For differential diagnoses, there are cardiac rhabdomyomas, fibromas, and myxomas. Cardiac rhabdomyoma is considered a congenital tumor of the heart. 2 Cardiac hamartoma and rhabdomyoma may have gross findings similar to each other. However, rhabdomyomas develop as solitary and/or multiple lesions in the heart, consisting mainly of neoplastic myocytes with clear cross-striated myofibrils: Occasional neoplastic cells have vacuolated cytoplasm containing abundant glycogen granules, giving an appearance of so-called spider cells; these neoplastic cells show mitotic activity. 27 Recently, the term purkinjeoma has been proposed for porcine rhabdomyoma of Purkinje cell origin. 13 Immunohistochemically, myogenic cardiac hamartoma and purkinjeoma exhibited similar characteristics; these neoplastic cells gave a strong reaction for desmin and a weak reactivity for vimentin. However, cardiac hamartoma and purkinjeoma differ in morphology in that purkinjeomas are made up of large cells with distinct cell borders and with an abundant, pale, eosinophilic, partly vacuolated granular cytoplasm, which resemble cellular characteristics of normal Purkinje cells.13,22 Additionally, Purkinje cells show positive reactions for neuronal heart conducting system markers, such as neuron-specific enolase and protein gene product 9.5.7,13 S-100 protein is also a neuronal marker that is simultaneously expressed in the protein gene product 9.5–positive conducting (Purkinje fiber) system in the heart. 28 The negative reaction for S-100 protein supports the myogenic origin of the present case. Cardiac fibromas are characterized by proliferation of neoplastic fibroblasts accompanied with various amounts of collagen fibers, and degenerating myocytes and focal calcification may be seen in cardiac fibromas. 18 Cardiac myxomas are composed of intervening satellite and spindle-shaped tumor cells supported by myxomatous matrix; the cells might arise from mesenchymal cardiomyocyte progenitor cells. 15 Histopathologic features reminiscent of cardiac fibromas and myxomas were not seen in the present case.
The pathogenesis of hamartoma is unknown, but congenital anomalous development of embryonic cells seems most likely. 19 In humans, some cases of cardiac hamartomas have been considered to be related to an autosomal dominant disorder due to defective TSC-1 gene on chromosome 9q34 that encodes a protein called hamartin. 20 Hamartin, with TSC-2-encoded protein tuberin, affects proliferation of cells, especially at the G1 phase of the cell cycle. 20 Hamartin acts as a negative regulator of cell proliferation; the functional loss of hamartin due to the mutation may induce uncontrolled cell proliferation. 20 The pedigree of the present case could not be inquired. To know the pathogenesis, cases of cardiac hamartomas in veterinary medicine should be accumulated in not only the squirrel monkey but also other animal species.
Footnotes
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
The authors declared that they received no financial support for their research and/or authorship of this article.