
Abstract
Multiple diverticula of the right and left cardiac ventricular walls were incidental findings at necropsy in a juvenile, male, mixed-breed dog with no clinical history of heart disease. Each saccular diverticulum had a narrow communication into the corresponding ventricular chamber. Histologically, the diverticular walls consisted mainly of collagen without elastin fibers and atrophic cardiomyocytes. No inflammation or other lesions were associated with the diverticula or the rest of the myocardium. Based on the history and pathologic findings, a diagnosis of congenital biventricular fibrous diverticula was made.
Congenital cardiac aneurysms and diverticula are rare cardiac outpouchings first described in humans in 1816. The diagnosis is made after exclusion of possible underlying causal conditions, such as arterial disease, local or systemic inflammation, trauma, or cardiomyopathy. Although some cases are suspected to result from in utero viral infection or coronary vascular abnormalities, most are attributed to an intrinsic, mural defect in embryogenesis. Some cases are associated with other cardiac, vascular, or thoracoabdominal abnormalities. 4,12,25
Congenital cardiac ventricular aneurysms and diverticula are classified into 1 of 3 categories. 9,24 True congenital aneurysms are muscular defects associated with an anomalous origin of the pulmonary artery. Muscular diverticula are cardiac outpouchings, usually apical, that are associated with midline abnormalities and congenital heart defects. Fibrous diverticula usually are subvalvular and basal and are associated with mitral and aortic valvular insufficiencies. 9
In humans, the clinical diagnosis of ventricular aneurysms or diverticula is established by echocardiography, magnetic resonance imaging, or ventricular angiography. Criteria to distinguish between congenital aneurysms and diverticula include the location and number of the lesions, the presence of other congenital or acquired cardiac malformations, contractility of the free wall of the outpouching, and the nature of the communication between the defect and the ventricular chamber. 13,18,27 Most aneurysms arise in the left ventricle. Biventricular, atrial, or right ventricular outpouchings of either type are uncommon and usually associated with other congenital cardiac anomalies. 10,14 In this report, we describe multiple, biventricular, fibrous cardiac diverticula in a dog with no other cardiac or extracardiac malformations.
History and Gross Findings
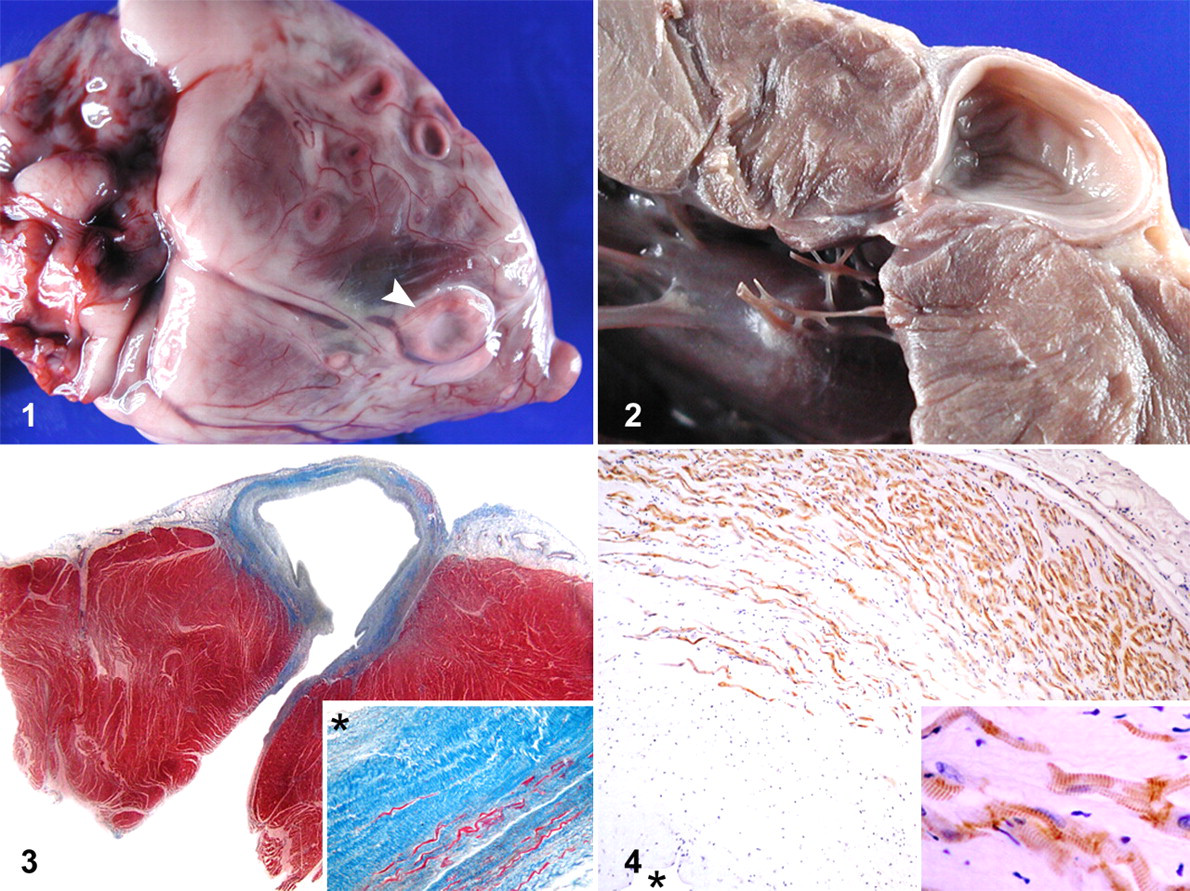
An 8- to 12-month-old, 12.5-kg, male, mixed-breed dog was donated by an animal shelter to the Veterinary College. The dog was reportedly healthy and without clinical disease before euthanasia. At necropsy, 16 variably sized, well-demarcated outpouchings were noted in the walls of both cardiac ventricles (Fig. 1 ): 9 in the left ventricle, and 7 in the right. The thin-walled pouches collapsed when blood was removed from the ventricles. The chamber of the pouches communicated with the corresponding ventricular chamber through a narrow channel whose lining was continuous with a thickened ventricular endocardium (Fig. 2 ). The pouches had a 1- to 2-mm-thick, gray-white, fibrous wall with no grossly apparent myocardial tissue. The chambers of the pouches ranged from 3 × 3 × 2 mm to 10 × 10 × 7 mm. The left and right ventricular myocardia adjacent to the pouches were 13- and 4-mm thick, respectively. No other cardiac or extracardiac abnormalities were identified, and the dog had no lesions of congestive heart failure.
Histologic Findings
Samples of liver, lung, heart, and kidney were fixed in 10% neutral buffered formalin and paraffin-embedded for light microscopy using hematoxylin and eosin, periodic acid–Schiff (PAS), Masson’s trichrome, and Verhoeff–Van Gieson histochemistry. Immunohistochemistry of cardiac sections was performed by the avidin–biotin–peroxidase method (ABC; Vector Laboratories, Burlingame, CA). Primary antibodies included anti-desmin (Eurodiagnostica, Arnehem, Netherlands), anti-actin (Enzolife Sciences, Farmingdale, NY), and anti-vimentin (Dako, Glostrup, Denmark). Diaminobenzidine was used as the chromogen; slides were counterstained with Harris' hematoxylin.
Histologically, the wall of the ventricular outpouchings consisted of mature connective tissue with parallel collagen fibers and fibroblasts and with a collagenous endocardium lacking elastin or Purkinje fibers (Fig. 3 ). No PAS-positive matrix was noted. No continuous myocardial layer was seen with Masson’s trichrome stain, but individual cardiomyocytes, which expressed desmin and actin but not vimentin, were noted mainly in the abluminal portion of the pouch walls. The antibody to actin delineated cross-striations in cardiomyocytes (Fig. 4 ).
No infarction, inflammation, granulation tissue, or coronary vascular abnormalities were identified in the diverticula, the diverticular–myocardial interface, or ventricular myocardium. No significant histologic lesions were detected in other organs. Based on the number and location of the defects, their fibrous nature, the presence of cardiomyocytes in the fibrous walls, and the absence of evidence of primary myocardial disease, the diagnosis was congenital biventricular fibrous diverticula.
Discussion
Human congenital ventricular aneurysms and diverticula are rare, with a prevalence of 0.5/100,000 births. 20 The terms congenital ventricular aneurysm (CVA) and congenital ventricular diverticulum (CVD) have been used interchangeably in the literature, and although various criteria have been proposed to differentiate the 2 entities, there is no consensus on their distinguishing features. 12
A CVD is a saccular structure with a narrow communication with the ventricle; its wall has synchronous, systolic contractility. 25 This contractile property explains the term muscular ventricular diverticulum, which is also used for CVD. 1
In contrast, a CVA is a large akinetic or dyskinetic pouch with broad communication with the ventricle. 25 Histologically, a CVA tends to be fibrous with a minor, atrophic myocardial component when compared with the muscular wall of a CVD. 15,25 A second type of cardiac diverticulum, the fibrous diverticulum, has been described. It has a narrow connection with the ventricle, is not contractile, and usually is multiple. It originates from the base of the left ventricle and is not associated with other congenital malformations. 2,9,21,23,24 The present case had multiple, small, flask-shaped pouches with mainly fibrous walls that included atrophic cardiomyocytes and communicated with the ventricular lumen via a narrow channel. These findings are most consistent with fibrous CVD as defined in human medicine.
Ventricular aneurysms and diverticula represent either primary congenital defects or lesions that arise at points of weakness in the ventricular wall secondary to myocardial ischemia, trauma, or infections. 20,22 They are considered congenital when no causes for acquired defects are discovered. 12
Myocardial infarction secondary to coronary arteriosclerosis is documented in humans and dogs. 5,26 This process leads to focal scarring and myocardial atrophy after the initiating ischemic event 26 but in humans may progress to ventricular aneurysms. 19
Myocarditis due to trypanosomiasis and septic endomyocarditis are the most frequent infectious causes of ventricular aneurysms. 16 Such aneurysms usually are small, may be multiple, and usually affect young patients without risk factors for ischemic heart disease. 6 Coxsackievirus is reported to cause ventricular aneurysms without histologic evidence of myocarditis, 8 but most cases of human infection-related aneurysms are characterized by inflammation, focal necrosis, and interstitial fibrosis. 7
Types II and VI mucopolysaccharidoses have been associated with the development of left ventricular aneurysms in human beings. 11,17 The accumulation of proteoglycans in the myocardial interstitium presumably alters the extracellular matrix, which is a critical determinant of myocardial contractility and the myocardial response to increased wall stress.
In this report, the absence of underlying histologic lesions, such as coronary vascular disease, myocardial infarction, necrosis, or inflammation, and the absence of cytoplasmic or interstitial PAS-positive material (eg, glycogen deposits) further support the diagnosis of a congenital malformation as the most plausible origin of the ventricular diverticula.
In human medicine, most congenital ventricular outpouchings are classified as nonapical CVA or CVD or as apical CVD. Nonapical CVAs usually are solitary, large, and unassociated with other cardiac or extracardiac malformations. 12 Although 2 types of CVD have been described in humans, apical CVDs comprise more than 70% of reported cases and are characterized by solitary, large diverticula restricted to the apex of the left ventricle. They are associated with other cardiac and midline thoracoabdominal defects. 4 Nonapical CVDs are generally small, multiple, diverticula in the free wall of the left ventricle, unassociated with other congenital malformations. 2 Although this dog had 1 small apical outpouching, it had no other anatomic abnormalities, and overall, the lesions were most similar to those described for human nonapical CVD.
The prognosis of each form of human congenital ventricular outpouching varies, so accurate clinical diagnosis is important. 10 The prognosis is more guarded for apical CVD and depends upon the severity and the reparability of the associated malformations. However, both apical and nonapical CVDs generally are asymptomatic with a good prognosis after surgical repair. 24 Most patients with CVA are asymptomatic until the second decade of life, when CVAs often are associated with fatal cardiovascular complications including systemic embolization, heart failure, arrhythmias, valvular regurgitation, pericardial effusion, ventricular wall rupture, and/or sudden death. 12,18 No intralesional thrombi, which are reported in approximately one-third of CVA cases, 3 or lesions of myocardial disease were detected in the present case. Thus, the described canine defect may have behaved as in human cases and remained asymptomatic had the dog not been euthanatized.
To our knowledge, this is the first description of congenital biventricular cardiac diverticula in a domestic animal. Although human diagnostic criteria may not be applicable, this case resembles human cases of congenital diverticula. Characterizing the macroscopic and histologic features of veterinary cases will be key to establishing comparative clinicopathologic relationships and, ultimately, the prognosis.
Footnotes
Acknowledgments
In memoriam of Esmeralda Thomas, a great person, a woman of wisdom, and the best mother.
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
The authors declared that they received no financial support for their research and/or authorship of this article.