
Abstract
A 13-year-old spayed Labrador Retriever cross dog presented for polyuria and polydipsia. Serum total calcium, free calcium, and intact parathyroid hormone concentrations were elevated. Surgical exploration of the ventral neck revealed a grossly enlarged right external parathyroid gland. The histopathological diagnosis for the excised right parathyroid gland was an incompletely resected parathyroid carcinoma. Parathyroid carcinoma in the dog is an infrequent cause of hypercalcemia and primary hyperparathyroidism.
A 13-year-old spayed Labrador Retriever cross dog (26 kg) was referred with a 6-week history of polyuria and polydipsia.
A complete blood cell count (CBC), serum biochemistry panel, and urinalysis (cystocentesis sample) were evaluated. The CBC revealed a mild lymphopenia (0.966 × 109/liter; reference interval, 1.2–5.0 × 109/liter), which was attributed to stress. Abnormalities in the serum biochemistry panel included a mildly elevated serum cholesterol concentration (7.28 mM; reference interval, 2.70–5.94 mM), increased serum alkaline phosphatase (ALP) activity (176 U/L; reference interval, 9–90 U/L), and mildly increased total calcium concentration (3.84mM; reference interval, 1.91–3.03mM). The free calcium concentration was elevated (1.87mM; reference interval, 1.25–1.45mM). Further testing revealed an increased intact parathyroid hormone (iPTH) concentration (38.6pM; reference interval, 3–17pM). The high cholesterol was most likely a postprandial elevation because a nonfasted sample was collected. An increase in the steroid-induced and/or hepatic isoforms of ALP could explain the elevated serum ALP activity. The urine was isosthenuric (urine-specific gravity, 1.008). Ancillary diagnostics included plain film thoracic and abdominal radiographs, which were unremarkable. Based on the presence of elevated free calcium and iPTH and the lack of detection of another neoplasm, primary hyperparathyroidism was considered to be the most likely diagnosis. The dog was taken for surgical excision of the external parathyroid glands, which were submitted for histopathological examination.
Differential Diagnosis
Hypercalcemia in the dog can have many etiologies, including malignancy (eg, primary hyperparathyroidism, humoral hypercalcemia of malignancy, multiple myeloma, and neoplasia in bone), renal failure, hypoadrenocorticism, and increased vitamin D activity (eg, rodenticides containing cholecalciferol, compounds containing calcipotriene or calcipotriol, plants containing calcitriol glycosides, excess dietary supplementation, and granulomatous inflammation). 15 Hypercalcemia of malignancy is the most common cause of hypercalcemia in the dog 3,15 and is most often due to lymphosarcoma or apocrine gland adenocarcinoma of the anal sac. 15 It is less commonly present with other malignancies, including multiple myeloma and carcinomas. 15 In primary hyperparathyroidism, the most common tumors of the parathyroid glands are adenomas, 2 whereas hyperplasia and parathyroid carcinoma are more infrequently diagnosed. 2,15
Microscopic Findings
Histopathologic examination of the right parathyroid gland, which was 3 mm in diameter, revealed a multilobulated, partially demarcated and encapsulated, highly cellular, expansile mass. A thin rim of atrophied normal parathyroid gland was present at the periphery of the mass. The lobules comprised cords, trabeculae, and nests of round to polygonal cells that were supported by thin strands of a fibrovascular connective tissue. The cells had indistinct cell borders and a high nuclear:cytoplasmic ratio. There was moderate anisokaryosis and anisocytosis and occasional binucleated cells and megalocytes (see Figure 1 ). Mitoses were present (0 to 1 per 40× objective field). Tumor cells focally infiltrated the capsule and invaded the remaining atrophied parathyroid gland. The histopathologic diagnosis for the right parathyroid gland was a parathyroid carcinoma. The left parathyroid gland was 1 mm in diameter and comprised only fibrous connective tissue with a mild mononuclear cell infiltrate consistent with contralateral parathyroid atrophy.
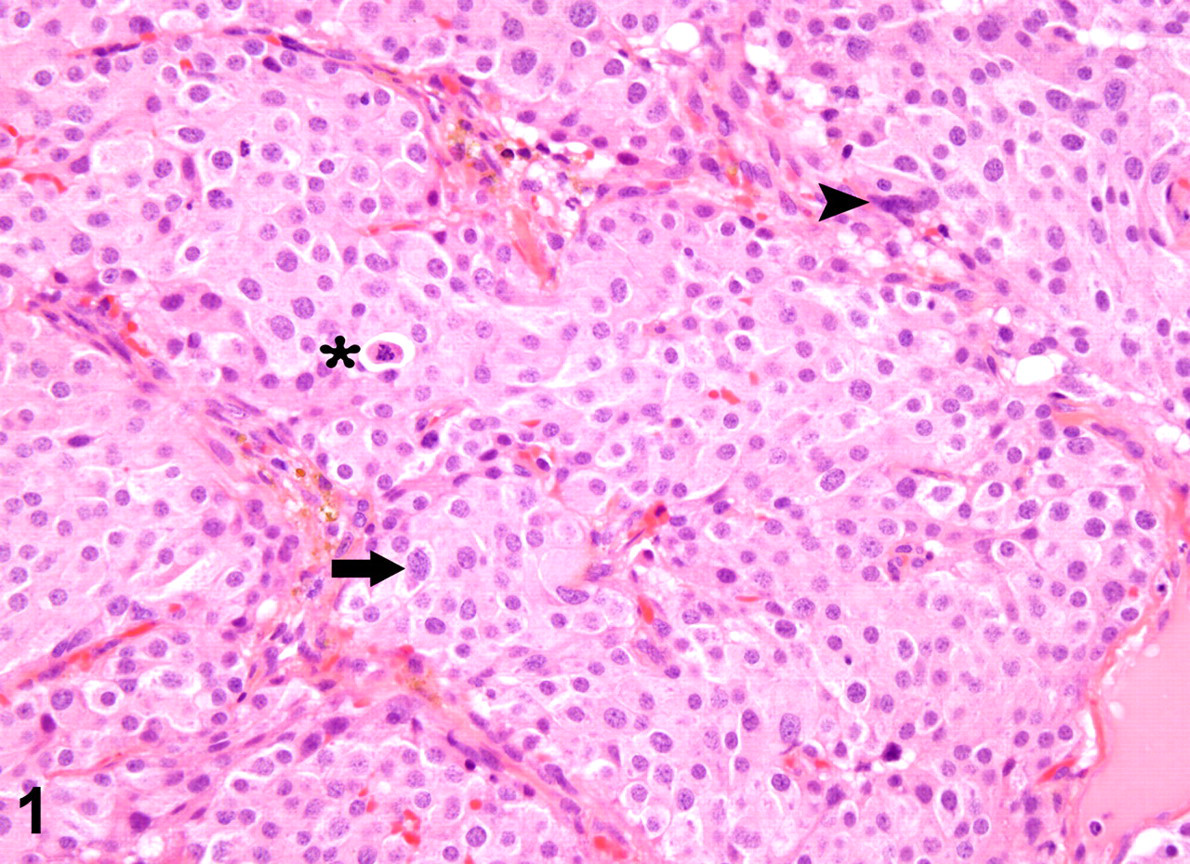
Parathyroid mass. Marked anisokaryosis and anisocytosis; karyomegaly (arrow); abnormal nuclear morphology (arrowhead) and mitotic figures (asterisk). HE.
Histologically, differentiating a parathyroid carcinoma from a parathyroid adenoma can be difficult. A parathyroid adenoma has well-differentiated cells and no invasion of adjacent tissue or the capsule. Parathyroid carcinomas tend to incorporate the entire gland, are invasive, and have a higher mitotic index and more cellular pleomorphism. 4 In this case, the degree of cellular pleomorphism, the number of mitotic figures, and the presence of capsular invasion were consistent with a parathyroid carcinoma.
Diagnosis
The diagnosis was hypercalcemia and primary hyperparathyroidism attributed to a parathyroid carcinoma.
Discussion
Clinical signs of hypercalcemia include polyuria, polydipsia, anorexia, listlessness, weakness, and signs related to urinary tract stones or infection. 8,17 Nephrogenic diabetes insipidus develops as elevated serum calcium levels interfere with proper functioning of the renal tubule cells that normally respond to antidiuretic hormone. 17 Anorexia may be due to direct effects of calcium on the central nervous system (CNS) or to decreased excitability of smooth muscle cells in the gastrointestinal tract. 5,6,17 Weakness can occur as increased calcium decreases excitability of skeletal muscle; listlessness and depression occurs from the direct effects of hypercalcemia on the CNS. 6,17 Hypercalcemia increases the likelihood of calcium uroliths and urinary tract infection. 4,8 In primary hyperparathyroidism, elevated parathyroid hormone levels increase calcium resorption from bone and the renal tubules and absorption from the intestines. 7
Serum calcium exists in 3 forms: In the normal dog, free calcium makes up 56% of total serum calcium; protein bound calcium constitutes 34%; and the remaining 10% is complexed calcium. 16 Free calcium (fCa2+) is the portion of total serum calcium that is biologically active; therefore, it is the portion that should be measured when assessing pathology. 16
Diagnosing the source of hypercalcemia begins with a complete history that will indicate the likelihood of vitamin D toxicosis owing to supplementation, rodenticide, certain plants, or antipsoriasis creams. 15 A complete physical examination will reveal the presence or absence of enlarged lymph nodes, rectal masses, or skeletal pain.
Diagnostic work-up for hypercalcemia should include a CBC, serum biochemistry profile, urinalysis and free calcium, iPTH, and parathyroid-related protein concentrations (PTH-rp). In this case, PTH-rp concentration was not measured, because the physical examination and plain film survey radiographs of the abdomen and thorax revealed no abnormalities, and primary hyperparathyroidism was considered to be the most likely diagnosis. If neoplasia is suspected, thoracic radiographs should be evaluated for evidence of metastatic disease relating to lymphoma or other malignancies and for systemic mycoses. 9 Ultrasonography of the neck region may be used to detect enlarged parathyroid glands, generally those that are 2 mm or larger. 11,19 Nuclear scintigraphy with technetium-labeled sestamibi has been used to attempt identification of hyperfunctioning parathyroid glands, but accuracy was found to be poor. 12 For definitive diagnosis of an enlarged parathyroid gland, histopathological examination of an excised gland is required.
Free calcium concentration helps differentiate primary from secondary hyperparathyroidism because dogs in chronic renal failure generally have normal to low free calcium. Serum iPTH concentration in dogs with malignancy-associated hypercalcemia is usually low, indicating an appropriate response of the parathyroid glands to elevated serum calcium, whereas a dog with primary hyperparathyroidism will have elevated PTH. PTH-rp produced by some tumors can activate PTH receptors, thereby inducing hypercalcemia. 18
Removal of abnormal parathyroid tissue is the treatment of choice for parathyroid neoplasms. Surgical intervention provides the most definitive diagnosis while delivering the most effective treatment. Alternative therapies that have been reported include chemical ablation of the affected glands 10,14 and percutaneous ultrasound-guided radiofrequency thermoablation. 13,14 Postsurgical management must include monitoring for hypocalcemia, which commonly develops 1 to 6 days after surgery. 11 Treatment with calcitriol and vitamin D supplements can be instituted to help avoid postoperative hypocalcemia. The long-term prognosis after removal of a parathyroid tumor is excellent provided that renal failure has not developed as a complication of hypercalcemia. 1 In a recently published study comparing parathyroidectomy, ultrasound-guided ethanol ablation, and ultrasound-guided heat ablation, 45 of the 48 parathyroidectomies in the study provided control of hypercalcemia for a median of 561 days. 14
Hypercalcemia has many etiologies, and a thorough diagnostic work-up is required to accurately ascertain the cause. If the cause is determined to be primary hyperparathyroidism, surgical excision provides both definitive diagnosis and therapy.
Footnotes
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.