
Abstract
Purpose:
Hospital admission is frequently required in the cancer trajectory. In a context of bed shortage, pressure on Emergency Departments and increasing healthcare costs, promoting actions that contain hospital stay is a priority. We studied the variables able to predict longer hospital stays.
Methods:
We retrospectively retrieved data on consecutive admissions in our cancer inpatient unit in a 6-month period and assessed individual and clinical variables potentially related with duration of hospital stay through univariate and multivariate analysis.
Results:
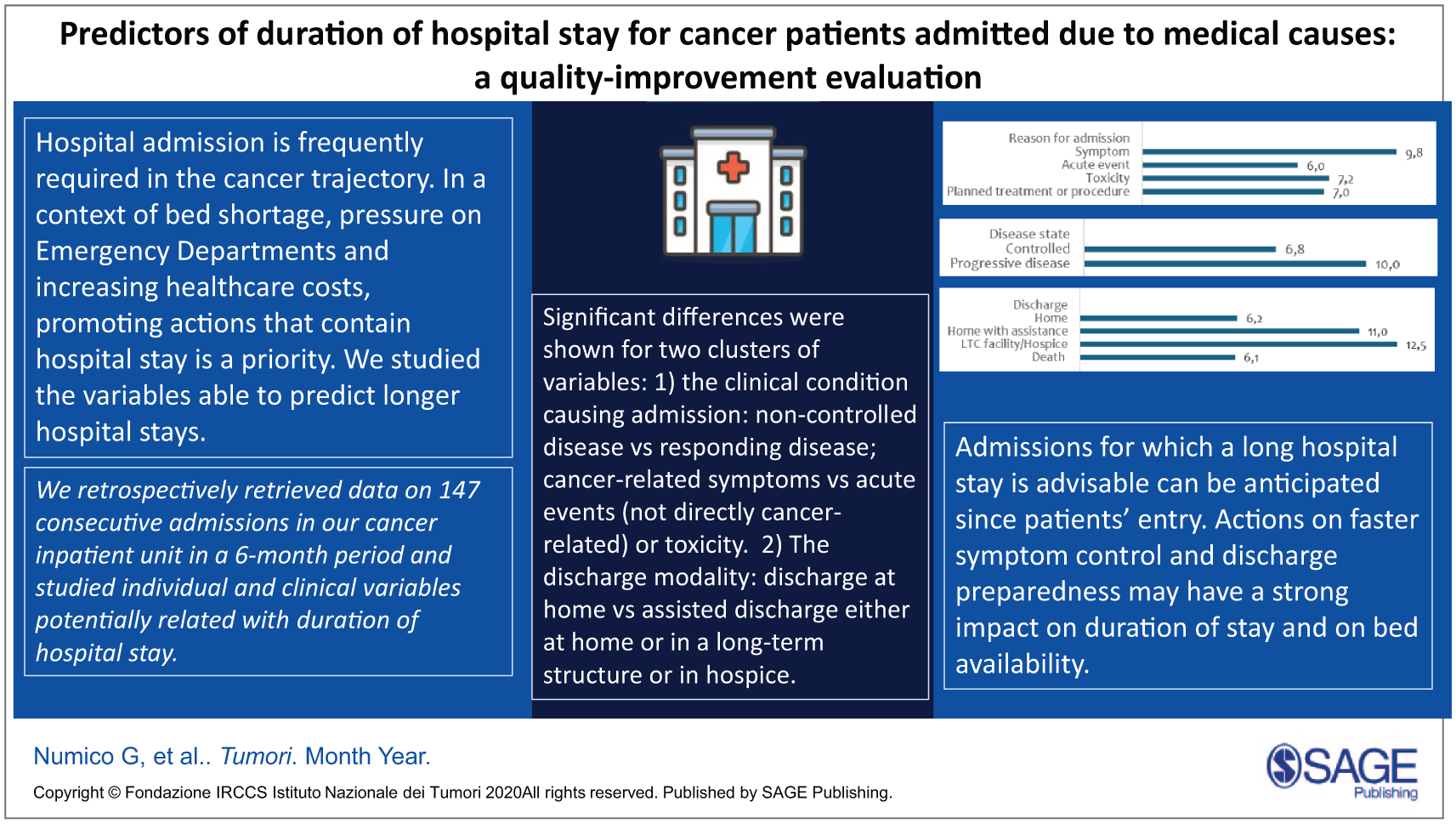
Among the 147 included admissions, mean overall duration of hospital stay was 8.46 days (95% I.C. 8.36 to 8.55). Significant differences were shown for two clusters of variables: 1) the clinical condition causing admission: non-controlled disease vs responding disease (10.0 vs 6.8 days, p: 0.006); cancer-related symptoms vs acute events (not directly cancer-related) or toxicity (9.8 – 6.0 – 7.2 days, respectively; p: 0.05). 2) The discharge modality: discharge at home (6.2 days) vs assisted discharge either at home or in a long-term structure or in hospice (11.0 and 12.5 days, respectively; p: 0.0001). Disease control and discharge modality retained statistical significance also in the multivariate analysis.
Conclusions:
Admissions for which a long hospital stay is advisable can be anticipated from patients’ entry. Actions on faster symptom control and discharge preparedness may have a strong impact on duration of stay and on bed availability.
Get full access to this article
View all access options for this article.