
Abstract
Introduction
Quality of life in childhood cancer survivors is largely affected by survivorship care and transition from treatment to long-term follow-up (LTFU). Referring to evidence-based recommendations, we wanted to evaluate LTFU care for survivors through a survey among the Italian Association for Pediatric Hematology-Oncology (AIEOP) centers. The project aimed to evaluate the availability of services in Italy, investigate strengths and weaknesses, analyze improvements of awareness in the field, and identify the gaps that need to be addressed by different centers.
Methods
Together with the family representatives, on behalf of AIEOP’s Late Effects Working Group, we developed a questionnaire on assisting childhood cancer survivors. All AIEOP centers received one questionnaire including information on local health system organizations; LTFU for childhood cancer survivors; services for adult survivors of childhood cancer; information provided to survivors/caregivers and care plan delivery.
Results
Forty-eight AIEOP centers were contacted and 42 replied, with a response rate of 87.5%. The majority of respondents confirmed their interest in assisting patients with a survivorship care plan (95.2%), regardless of a clinic or dedicated staff.
Discussion
This is the first overview of LTFU in Italy, which provides detailed results at national levels, prompting consideration of improvements in the last decade. Although there is a high level of interest in survivorship care, many centers lack resources to implement such programs. The identification of these challenges is useful for planning future strategies.
Introduction
Childhood cancer survivors (CCS) represent a significant challenge for healthcare systems, both for continuity and transition of care. Indeed, each year approximately 35,000 children and adolescents are diagnosed with cancer in Europe, and five-year survival rates have improved, reaching 81% for all cancers combined through all of Europe. 1 As new technologies and innovative drug therapies are increasing, so is the number of CCS, which is currently over 500,000 in Europe.1 -3
In Italy, there are more than 50,000 young adults who survive several years after a cancer diagnosis, 4 with many health problems arising even decades following the diagnosis; these individuals carry a risk of premature morbidity and mortality. In fact, approximately 60% of CCS develop at least one chronic health condition during their lifetime and nearly one in three will have severe/life-threatening long-term effects (LEs).5,6
Long-term follow-up (LTFU) programs, as well as healthcare education for survivors, parents, and professionals, is recommended by several guidelines.7,8 Therefore, CCS have been the focus of new research, which has aimed to highlight possible sequelae of the disease and treatments not only at a physical level but also at a psychosocial level. 7 The Erice statement, 9 a consensus of a panel of experts, underlines the need to continue with follow-ups for surveillance of potential LEs of cancer or its treatments. This statement recommends the establishment of a well-structured LTFU clinic with a multidisciplinary team to reduce the medical and psychosocial LEs burden. However, information to allocate resources to implement staff and spaces dedicated to this purpose is still scarce. 10
Resource allocation and the burden of CCS are of high interest in a country like Italy where healthcare is considered a fundamental right for all, with a national level administration ensuring that the fundamental principles of the national healthcare system are met throughout all the territory, but the system is regional based. Each region has a significant independence and flexibility in determining its own priorities and goals.
In 2012 a survey investigating LTFU programs in 20 European countries including Italy 11 underlined the lack of a well-organized LTFU for CCS: availability varied widely across European regions, with pediatric and adult LTFU being usually located in pediatric hospitals and run by pediatric oncologists.
The Italian Association for Paediatric Hematology-Oncology (AIEOP), 12 is a scientific society and a national cooperative group that has been working for children and adolescents with cancer in Italy since 1975. Based on recommendations from the International Guidelines Harmonization Group (IGHG) 13 and on expert opinions of the AIEOP, this study was designed to investigate the Italian situation, by comparing the management of LTFU for CSS among all pediatric hematology/oncology AIEOP centers with that reported in the previous study, ten years ago. 11 More specifically, we investigated the availability of pediatric hematology-oncology networks on a national basis with a long-term care for CCS and the improvement of the level of awareness in the field by health care professionals.
Methods
This study was conducted in Italy where the healthcare system provides universal care for every citizen at no charge, including all CCS. This is a cross-sectional study performed through the administration of a standard questionnaire. The study included all the 48 currently active AIEOP centers providing care to children with cancer in Italy.
Each center received an invitation to participate in the survey and a link to complete the questionnaire, which was electronically administered using SurveyMonkey online survey platform (https://www.surveymonkey.com). Only one questionnaire per center was allowed. The head of the department or the professional responsible for LTFU oversaw providing information for their center.
The questionnaire was developed by the AIEOP working group for LEs and parent representatives and included 91 items organized in four sections regarding: 1) the organization of care for CSS at regional level; 2) the availability of LTFU for CCS; 3) the availability of LTFU care for CCS > 18-year-old; 4) the delivery of information and education activities to CCS on LEs and LTFU ( Online Supplementary Material 1).
We considered for observation individuals surviving >5 years who could experience LEs of cancer treatments. 8
The questionnaire was administered from February to April 2022. The centers that did not respond within 20 days of the invitation were sent a maximum of three reminders. Quality control of collected data was done upon receipt of each questionnaire, and inconsistent or missing data were verified together with the responder.
A database was consolidated in Excel and used for the analysis, which consisted of descriptive statistics using the STATA v14.1E.
Since the study did not involve the collection of information from patients, we did not ask for approval from an ethical committee.
Results
A total of 48 AIEOP centers (Figure 1A) received the survey and 42 completed it (Response Rate -RR- 87.5%), representing all Italian regions with a center for CCS. Among the 42 respondent centers, one center reported that they do not provide supportive care for CCS because they are not a treating center for pediatric malignancies. Therefore, the final analysis was led on 41 respondent centers.
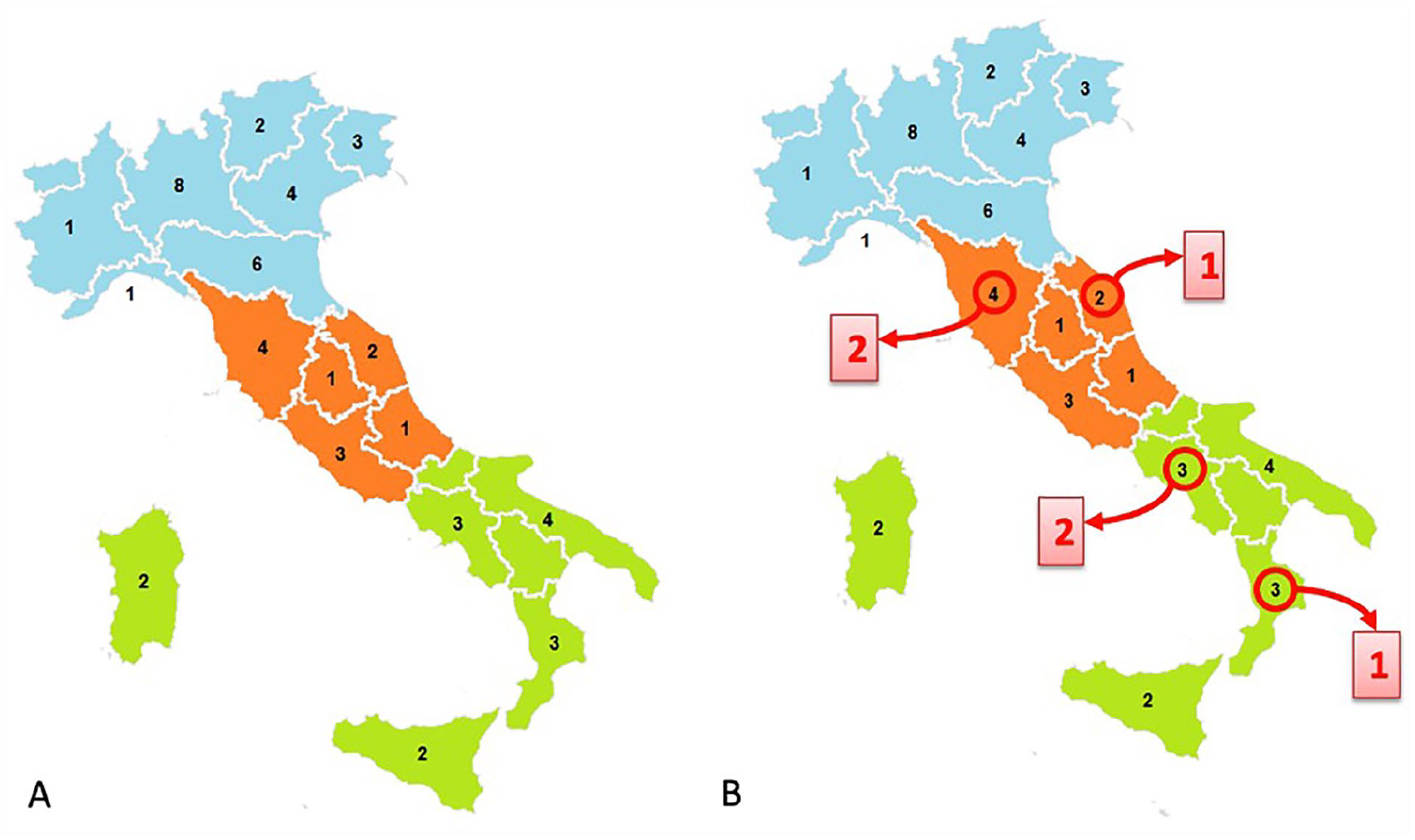
The geographical distribution of the 48 AIEOP centers in the different regions of Italy (A). In red the non-respondent centers (B). The number of patients followed up by each center varied between 10 and 1150.
Availability and characteristics of regional hematology-oncology networks
Out of the 41 valid responses, only 12 centers (29.3%) reported providing support for management of pediatric LTFU of CCS, which is already included in the national healthcare plan and in the Regional Oncology Network, while five (12.2%) reported the existence of health facilities dedicated to this population, and two (4.9%) reported a transition program for patients older than 18 or having more than five years off therapy. The general organization of LTFU clinics was investigated through specific items illustrated in Figure 2.
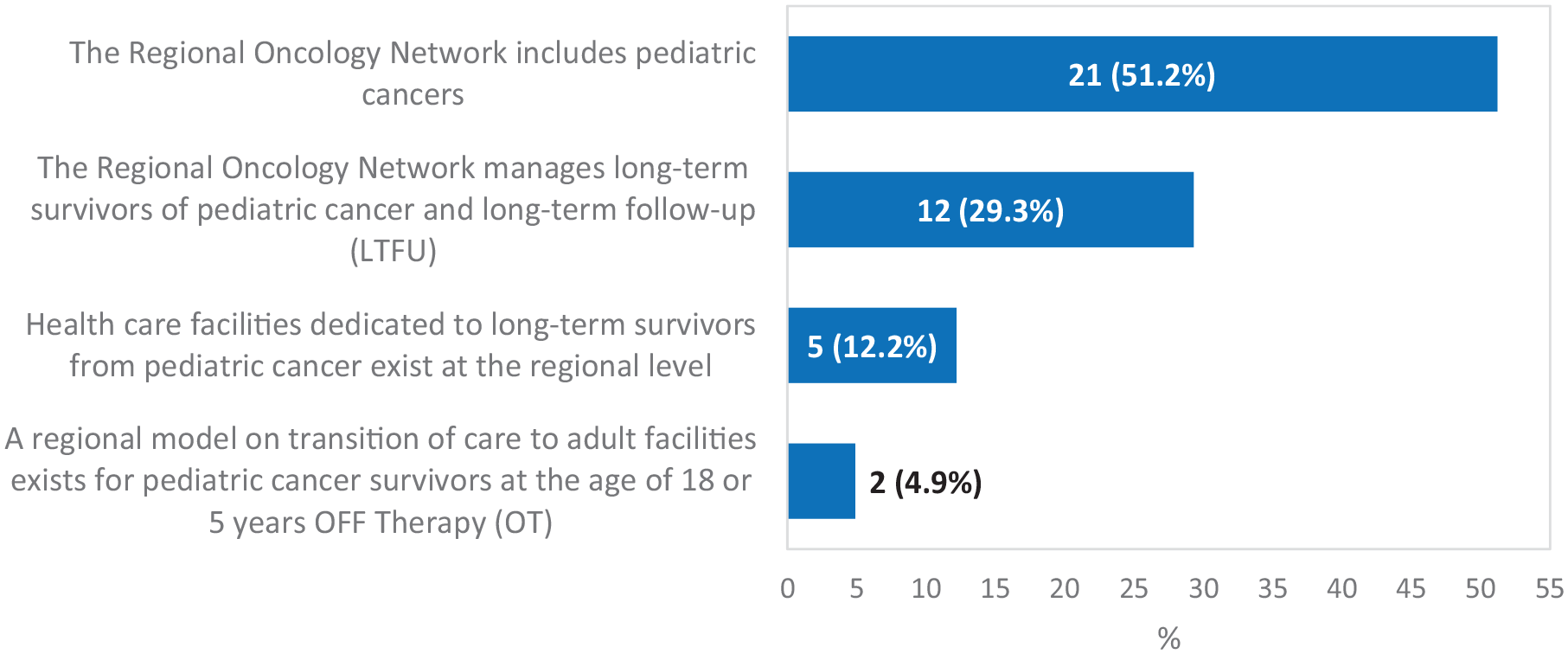
Features of hematology-oncology networks, the answers displayed represent positive responses.
Availability and characteristics of LTFU care for childhood cancer survivors
Approximately half of the respondent centers reported having dedicated staff and/or clinics for CCS (of these 47.4% have at least two professionals involved and one dedicated room); these are most frequently led by a medical doctor – pediatric oncologist or pediatric hematologist – (78.9%), an expert on LEs (13.2%), or a nurse (7.9%). Table 1 reports the affirmative responses to questions describing the characteristics of LTFU care for CCS aged < 18 years.
Features and organization of LTFU.
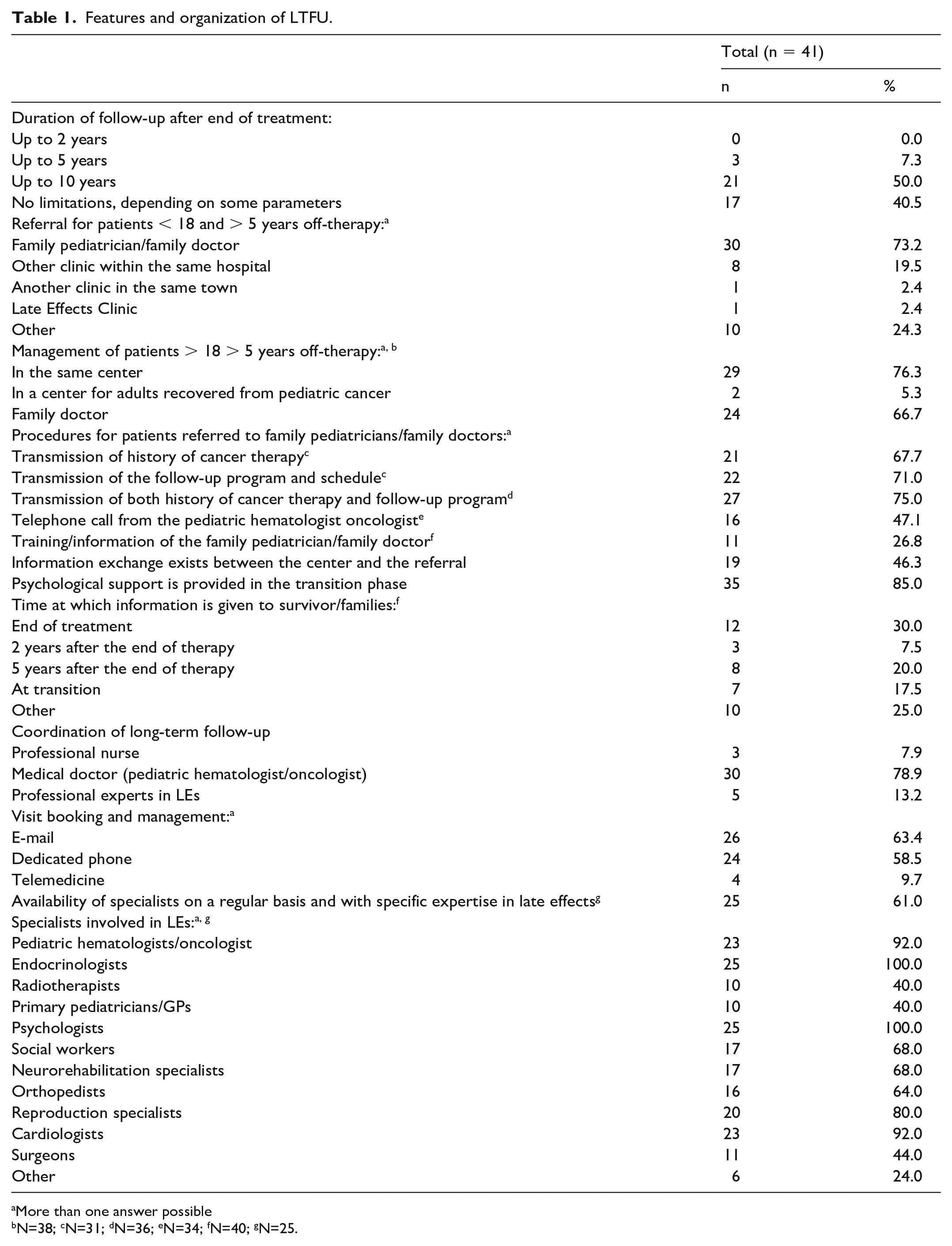
More than one answer possible
N=38; cN=31; dN=36; eN=34; fN=40; gN=25.
Almost all respondents (95.2 %) indicated that follow-up for CCS is available, and 87.8% of them reported no age limits. Patients off-therapy are monitored for at least 10 years in 50% of centers and over the entire life in 40.5% of centers, depending on specific clinical parameters. The main reasons to keep the CCS in the centers/LTFU clinics were the type of malignancies and the type of treatment received (79.5%). Specifically, allogenic Bone Marrow Transplantation (BMT) and Central Nervous System (CNS) tumor survivors were persistently followed in dedicated clinics by 53.6% and 33.3%, respectively.
A multidisciplinary team or a collaboration with healthcare specialists were available in 25 respondent centers (61.0%). Out of them, 100% reported to have psychologists and endocrinologists, and 92% at least one pediatric oncologist and cardiologist.
Most respondent centers (90.2%) provided written documentation of the previous clinical history (31.3%) or a combination of previous history plus recommendations according to the treatment received in 63.4% of cases. A survivorship passport has been available for all AIEOP centers since the end of 2021 and was routinely provided in seven of the largest AIEOP RCs at the time of this survey. A transition of care to the family pediatrician or the family doctor was reported by 73.2% to 66.7% of respondent centers, respectively, while transition to a LTFU clinic was reported in 23.8%. In case of transition, written documentation including the clinical history and/or the care plan is transmitted by 67.7% to 75% of respondent centers, and many centers (30%-50%) reported exchanging information with GPs. Psychological support for CCS in case of transition is frequently provided (85.0%).
Only one center reported to have a LTFU clinic for adult (age >18 years) CCS, with selected staff and professionals.
Communication with patients and families
Information on LEs and LTFU to patients and families are standardized in 80.5% of respondent centers and are provided mainly by pediatric hematologists oncologist (75.6%). Information is provided at diagnosis in 61% of centers, at the end of treatment in 56.1%, and at the beginning of LTFU in 34.1%. The majority of centers (73.2%) rely on oral communication only, although 26.8% are planning to provide written documentation in the future.
We also asked for the preferred definition of childhood cancer survivors. Nearly 60% of respondents reported they would define them as “cured from a childhood cancer”, 19.5% would define them as “long-term survivors of a childhood cancer”, 19.5% as “childhood cancer survivors”, and 2.4 % as “long living”.
Strengths and limitations
This is the first survey on this topic specifically used in our country and comprehensive of all AIEOP centers. This work gives a clear description of the improvement in several areas of CCS management in comparison with what was observed a decade ago in the study of Essig et al. 11 Although some of the smaller centers did not participate in the study, the response rate was high and all Italian regions with an AIEOP center were represented. Moreover, the exclusion of age limits in “at risk” conditions and the availability of a specific tool such as a passport are some positive aspects underlined by our results.
This survey also resulted in findings that may be translated into potential actions, such as the inclusion of survivorship at the national level as a model of care, with the support of dedicated nurses; a better definition of clinics for adult CCS; more attention to dissemination on LEs and healthy lifestyles through written/digital information for survivors, families, and GPs.
The main limitation of the study relies on the self-reported questionnaires and the potential associated bias as an increase in positive answers and hiding negative aspects.
Discussion
AIEOP as a scientific society is accredited by the Italian Ministry of Public Health and AIEOP centers are part of Italy’s national health system. Despite the fact centers have different volumes of activity and different specificities, 12 our survey showed an equally distributed high level of interest in survivorship issues. The response rate in this study was 87.5%, while in the previous survey on the availability and characteristics of LTFU programs published in 2012, among the 54 AIEOP centers contacted, only 25 replied, with a RR of 46%. 11 At that time, 48.0% of Italian responder centers reported having a LTFU for CSS and 48.0% having a program for adults.
At that time, the AIEOP guidelines/recommendations for CCS and the Survivorship Passport 14 were not yet available. The Survivorship Passport provides a summary of each survivor's clinical history, with detailed information about the original cancer diagnosis and the treatments received, together with personalized follow-up and screening recommendations based on guidelines published by the International Guidelines Harmonization Group and PanCareSurFup. The experience gained from the passport project and the increasing awareness of the importance of LTFU in Europe through the Pancare Network 15 positively impacted the AIEOP centers 13 and led to an improvement in CCS knowledge and care.
According to the results of our study, 51.2% of AIEOP centers reported having a specific LTFU clinic and/or dedicated staff for this purpose, a figure that has almost doubled compared to that reported for Italy in 2012. 11 Knowledge and resources to implement staff and spaces for survivors are not the only current challenges for CSS care. Moreover, the increasing number of centers that confirmed interest to manage CCS (95.2%), regardless of dedicated space and personnel, should be appreciated. This improvement represents the recognition that managing the care of CCS is part of the process of recovering from cancer. This does not translate into a diminished role of an LTFU clinic and the dedicated staff: an organized clinic and staff implies funds and trained professionals with more time for patients and research. 11 However, this finding suggests that establishing a LTFU clinic in almost every AIEOP center is possible in the coming years or that the largest centers could serve as “hubs” for the others.
The increased interest in this topic also explains the significant number of respondent centers reporting no age limits in the follow-up of their CCS, depending on their clinical conditions. Although many patients were, are, and will be successfully treated without LEs and will live a healthy life, a significant number of CCS will experience chronic health conditions (60%), and 20-30% will have a severe/life threatening LEs.16,17 It is important to recognize that the risk of LEs increases with age, without reaching a plateau, 16 and some CCS need adequate lifelong medical, psychological, and social care. The availability of LTFU for adult CCS was infrequently reported in our survey. Available data suggest that several CCS are followed by a general practitioner with experience in LEs, but this observation is not confirmed for adult CCS both in Europe and North America.18 -20 In adult oncology, the survivorship is now recognized as a challenge, and there is evidence that a fragmentation of care and a lack of coordination between primary care physicians, oncologists, and survivors exist. 21 All these reasons might increase the CCS’s hesitancy to make a transition to other centers, leaving pediatric institutions with the burden of the adult CCS population. A well-organized transition of care is crucial to obtain a high quality of life for patients and families with a rational use of resources in the healthcare system, considering the universality of the Italian healthcare system.
Most respondent centers in our survey reported to support and manage information for survivors and families of LEs, as in the rest of Europe and North America.10,11,19,22 A clinical nurse specialist is usually available in many US pediatric centers, 17 while our report indicates that such a professional profile is rarely available in AIEOP centers. This result is similar to the study conducted in 2012 and suggests developing a focus strategy to address this gap.
A significant number of respondent centers provided a written summary of treatments and/or a follow-up care plan, or/and a combination of both, including a Survivorship Passport, which is available in all AIEOP centers since 2021. 14 This tool is intended to use standard information with evidence-based follow-up prescriptions and recommendations that can easily be implemented. Of note, a written document that provides further information on LEs for survivors and families is still rarely provided.
Efforts in improving the organization of care for CCS can reduce the morbidity and mortality as observed in some specific groups.23,24 A reduction in excess deaths among CCS with a healthy lifestyle and no cardiovascular risk factors as they age has been recently reported: supportive interventions for maintaining a healthy lifestyle should be the primary objective of all clinicians involved in pediatric oncology, and not only in LTFU clinics. 25
Finally, we explored the terminology and wording associated with CCS. Although our questionnaire was in Italian, and the recognition of “survivors and survivorship” as the scientific English wording, respondents indicated the term “cured from pediatric cancer” (60%) as the most appropriate term for CCS. In Italian, the word “cured” means a biological remission of the disease but also refers to a word with an important psychological impact on the daily life of CCS: it may reassure patients that cancer has been left behind. 26
Although the COVID pandemic had a negative impact on the healthcare system, we observed an improvement in survivorship care within our country thanks to international collaborations and the work done in the last decade. This study underlines the actions that remain to be implemented to improve programs for LEs.
Supplemental Material
sj-pdf-1-tmj-10.1177_03008916231185981 – Supplemental material for Current practices of follow-up programs for childhood cancer survivors in Italy
Supplemental material, sj-pdf-1-tmj-10.1177_03008916231185981 for Current practices of follow-up programs for childhood cancer survivors in Italy by Monica Terenziani, Alberto Eugenio Tozzi, Laura Diaco, Eleonora Biasin, Alessandro Cattoni, Ileana Croci, Donatella Fraschini, Giovanna Giorgiani, Riccardo Haupt, Monica Muraca, Marta Pillon, Giovanna Sironi, Maria Grazia Valsecchi and Angela Mastronuzzi in Tumori Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.