
Abstract
Objective
Post-lumbar puncture headache is a common complication following lumbar puncture. Although several risk factors have been established, the role of low body mass index remains controversial. This study aimed to evaluate the association between body mass index and post-lumbar puncture headache in Chinese adults undergoing lumbar puncture.
Methods
In total, 499 patients who underwent lumbar puncture at the Department of Neurology between January 2022 and March 2024 were enrolled. Data on demographic characteristics, blood pressure, lumbar puncture history, and cerebrospinal fluid parameters were collected. Univariate and multivariate logistic regression models were employed to assess the relationship between body mass index and post-lumbar puncture headache. Subgroup analyses were conducted to evaluate the consistency of this association across sex, age, blood pressure, cerebrospinal fluid volume, and cerebrospinal fluid protein levels.
Results
Post-lumbar puncture headache occurred in 13% (65/499) of patients; among these, 63.1% were female. Compared with those without post-lumbar puncture headache, those with a headache were younger (p < 0.001), had lower body mass index (p = 0.003), lower systolic and diastolic blood pressures (p = 0.001 and p = 0.001), lower cerebrospinal fluid protein level (p < 0.001), and greater cerebrospinal fluid collection volume (p < 0.001). No significant association was found between primary disease classification and post-lumbar puncture headache (p = 0.164). In univariate logistic regression analysis, the risk of post-lumbar puncture headache significantly decreased with increasing body mass index values (odds ratio = 0.9, 95% confidence interval: 0.84–0.97, p = 0.003). After multivariable adjustment for sex, age, blood pressure, cerebrospinal fluid protein level, and cerebrospinal fluid volume, the association remained significant (odds ratio = 0.92, 95% confidence interval: 0.85–0.99, p = 0.033). Further analysis, in which patients were grouped by body mass index levels and assessed using two multivariate regression models, revealed that individuals with a low body mass index had a significantly higher risk of post-lumbar puncture headache. In Model I, adjusted for sex and age, the odds ratio was 3.2 (95% confidence interval: 1.41–7.23, p = 0.005); in Model II, further adjusted for systolic pressure, diastolic pressure, cerebrospinal fluid protein level, and cerebrospinal fluid collection volume, the odds ratio was 3.14 (95% confidence interval: 1.36–7.25, p = 0.007). The findings were robust across both models. The findings were consistent in the subgroup analyses.
Conclusion
Lower body mass index is significantly associated with an increased risk of post-lumbar puncture headache. These findings underscore the importance of considering body mass index in preoperative risk assessment and postoperative management for patients undergoing lumbar puncture. However, due to the cross-sectional study design, causal inference cannot be established.
Introduction
Post-lumbar puncture headache (PLPH) represents one of the most frequent complications following lumbar puncture, arising primarily due to cerebrospinal fluid (CSF) leakage and subsequent low CSF pressure.1,2 According to the International Classification of Headache Disorders (ICHD-3), 3 PLPH is defined as a headache that develops within 5 days of the procedure, persists for several hours to days, and typically resolves spontaneously within 2 weeks. The headache must be clearly attributable to the lumbar puncture and not better accounted for by other disorders. Clinical reports have indicated that PLPH affects between 3.5% and 33% of individuals undergoing lumbar puncture, 4 with characteristic exacerbation upon sitting or standing and relief in the supine position. In addition to pain, PLPH is associated with several morbidities, including nausea, vomiting, vertigo, hearing loss, visual disturbances, and even cranial nerve palsies,5–8 significantly impairing patients’ quality of life. Consequently, early identification of at-risk individuals and timely intervention are critical to mitigate its impact.
The precise pathophysiology of PLPH has not been completely elucidated; however, it is widely attributed to intracranial hypotension resulting from CSF leakage, which causes traction on pain-sensitive intracranial structures and compensatory venous dilation.9,10 Several independent risk factors have been established, including female sex, age between 31 and 50 years, history of PLPH, and perpendicular orientation of the needle bevel relative to the spinal axis during puncture. 3 Additional factors such as low body mass index (BMI),11–13 chronic headache history, needle size, trajectory angle, and operator experience have also been implicated8,13–16 although the association between PLPH and low BMI remains inconsistent across studies.15,17,18 The present study aimed to evaluate the incidence of PLPH in a clinical patient undergoing lumbar puncture and further examine the role of BMI in PLPH development. Our findings sought to inform evidence-based strategies for risk assessment and proactive management of this common complication.
Methods
Patients
In total, 499 patients who underwent lumbar puncture at the Department of Neurology at the Affiliated Hospital of Jining Medical University between January 2022 and March 2024 were retrospectively included in this study (Figure 1). Written informed consent was obtained from all participants. The study protocol was approved by the Ethics Committee of the Affiliated Hospital of Jining Medical University (reference 2023-03-C033). The study was conducted in accordance with the Declaration of Helsinki (2024 revision). All patient details were deidentified to ensure privacy. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. 19

Patient selection and inclusion.
Data collection
Data were retrospectively collected from the Electronic Medical Record System using a standardized form. Extracted variables included demographic characteristics (sex and age), BMI, pre-puncture blood pressure, volume of CSF collected, and CSF laboratory parameters (cell count, protein, glucose, lactate dehydrogenase, and opening pressure). Blood test results, including complete blood count, glucose level, liver and renal function test results, and final clinical diagnoses were also recorded. Histories of headache, back pain, and prior lumbar puncture were recorded. BMI was calculated as weight in kilograms divided by height in meters squared and categorized per the World Health Organization (WHO) criteria as follows: (a) underweight (<18.5 kg/m2); (b) normal (18.5–23.9 kg/m2); (c) overweight (24–27.9 kg/m2); and (d) obese (≥28 kg/m2).
Lumbar puncture
A neurologist guided the patient into the left lateral decubitus position, with the head flexed toward the chest, knees drawn up toward the abdomen, and the back positioned flush with the edge of the bed, maintaining perpendicular alignment to the surface, thereby maximizing the intervertebral space opening. The puncture site (L3–L4 or L4–L5) was identified. After sterilization and local anesthesia induction using 2% lidocaine, a paraspinal approach was employed, using a 0.9 × 100-mm (Quincke-type) cutting needle. Once loss of resistance was felt, the stylet was withdrawn. Following confirmation of free CSF flow, the opening pressure was measured, and CSF was collected slowly. All lumbar punctures were performed electively by neurology physicians.
Evaluation criteria for PLPH
According to the International Classification of Headache Disorders, third edition (ICHD-3), 3 a diagnosis of PLPH was established using the following diagnostic criteria: (a) headache occurs within 5 days after the lumbar puncture; (b) orthostatic headache; (c) headache is accompanied with at least one of the following symptoms, including stiff neck, tinnitus, hyperacusis, photophobia, and nausea; and (d) the headache resolved on its own within a week or 48 h after effective treatment of the CSF leak (normally with the use of an epidural blood patch). Patients were routinely followed up during hospitalization; those discharged before 5 days were contacted by telephone to assess for headache symptoms.
Statistical analyses
Categorical variables are presented as numbers (percentages) and were compared using the chi-square test. Continuous variables are expressed as mean ± SD or median (interquartile range) based on distribution normality and compared using analysis of variance (ANOVA) or Kruskal–Wallis test. Univariate logistic regression analysis was performed to evaluate associations between candidate predictors, including sex, age, blood pressure, CSF protein level, and CSF volume, and PLPH. Multivariable logistic regression models were constructed to adjust for potential confounders. Model I was adjusted for sex and age, and Model II was adjusted for sex, age, systolic pressure, diastolic pressure, CSF protein level, and CSF volume. We estimated 95% confidence intervals (CIs) and odds ratios (ORs) for all the models. BMI was analyzed as both a continuous and categorical variable. Stratified analyses and interaction tests were performed based on sex, age, blood pressure, CSF volume, and CSF protein level. Statistical analyses were performed using R software (http://www.Rproject.org, The R Foundation) and Free Statistics software version 2.4.0. A two-sided p-value <0.05 was considered statistically significant.
Results
Baseline characteristics
The demographic and clinical characteristics of the 499 patients who underwent lumbar puncture are shown in Table 1. The male/female ratio was 1.1 (266/233), and mean patient age was 46.1 ± 18.7 years. Furthermore, 42.8% (213/499) of the patients were finally diagnosed with immunologic diseases, 41% (204/499) with infectious diseases, 3.0% (15/499) with genetic diseases, 2.4% (12/499) with metabolic diseases, and 10.8% (54/499) with other diseases. With respect to lumbar punctures, 15% (75/499) were performed by discipline-trained physicians, 43.5% (217/499) by resident physicians, 23.4% (117/499) by attending physician, and 18% (90/499) by the associate chief physicians or above.
Baseline characteristics of patients with lumbar puncture.

The data are presented as mean ± SD, median (Q1, Q3), or n (%).
PLPH: post-lumbar puncture headache; BMI: body mass index; CSF: cerebrospinal fluid; Q1: quartile 1; Q3: quartile 3.
In total, 65 patients had PLPH; among these, 63.1% (41/65) were female. The mean age of the patients with PLPH was 35.3 ± 18.1 years; 52.3% (34/65) were diagnosed with infectious diseases, 30.8% (20/65) with immunologic diseases, 1.5% (1/65) with genetic diseases, 1.5% (1/65) with metabolic disease, and 13.8% (9/65) with other diseases. There was no significant association between the classification of the primary diseases and PLPH (p = 0.164).
Compared with those without PLPH, patients with PLPH were younger (p < 0.001) and had lower BMI (p = 0.003), lower systolic and diastolic blood pressures (p = 0.001 and p = 0.001), lower CSF protein levels (p < 0.001), and more volume of CSF collection during the lumbar puncture (p < 0.001). There were no statistically significant differences in the history of lumbar puncture, headache, professional experience of the operators, classification of primary diseases, CSF pressure, lactate dehydrogenase, CSF glucose levels, and hematological parameters between patients with and without PLPH. A detailed comparison of patients with and without PLPH is presented in Table 1.
There was a significant difference in the prevalence of PLPH based on BMI categories (p = 0.001); the prevalence rate was 35.1% (13/37) in the low-BMI group, 12.7% (29/228) in the normal group, 10.9% (18/164) in the overweight group, and 7.1% (5/70) in the obesity group.
Univariable and multivariable analyses
As shown in Table 2, univariate analysis revealed that PLPH occurrence was associated with younger age (OR = 0.96, 95% CI: 0.95–0.98), low BMI (OR = 0.9, 95% CI: 0.84–0.97), low systolic blood pressure (OR = 0.97, 95% CI: 0.96–0.99), low diastolic blood pressure (OR = 0.96, 95% CI: 0.94–0.98), and high volume of CSF collection during lumbar puncture (OR = 1.35, 95% CI: 1.21–1.51).
Univariate analysis for post-lumbar puncture headache.

BMI: body mass index; CSF: cerebrospinal fluid; OR: odds ratio; CI: confidence interval.
In univariate logistic regression analysis, the risk of PLPH significantly decreased with increasing BMI levels (OR = 0.9, 95% CI: 0.84–0.97, p = 0.003). This association remained consistent after adjusting for all confounding factors in multivariate logistic regression analysis (OR = 0.92, 95% CI: 0.85–0.99, p = 0.033).
Further analysis, in which patients were grouped by BMI levels and assessed using two multivariate regression models, revealed that individuals with low BMI had a significantly higher risk of PLPH. In Model I, adjusted for sex and age, the OR was 3.2 (95% CI: 1.41–7.23, p = 0.005); in Model II, further adjusted for systolic pressure, diastolic pressure, CSF protein level, and CSF collection volume, the OR was 3.14 (95% CI: 1.36–7.25, p = 0.007). The findings were robust in both models (Table 3).
Multivariate analyses of risk factors associated with post-lumbar puncture headache.

Model I was adjusted for sex and age; Model II was adjusted for sex, age, systolic blood pressure, diastolic blood pressure, CSF protein level, and volume of CSF collection.
OR: odds ratio; CI: confidence interval; BMI: body mass index.
Subgroup analysis
Stratified analysis of the associations between BMI and PLPH is presented in Figure 2. When subgroup analysis was performed according to the confounders, including age, sex, systolic blood pressure, diastolic blood pressure, CSF protein level, and volume of CSF collection during the lumbar puncture, no significant interaction was observed across all subgroups, suggesting that the effect of BMI on PLPH remained consistent across subgroups. The association between BMI and PLPH in the stratified analysis was consistent with that in the multivariate logistic regression analysis.
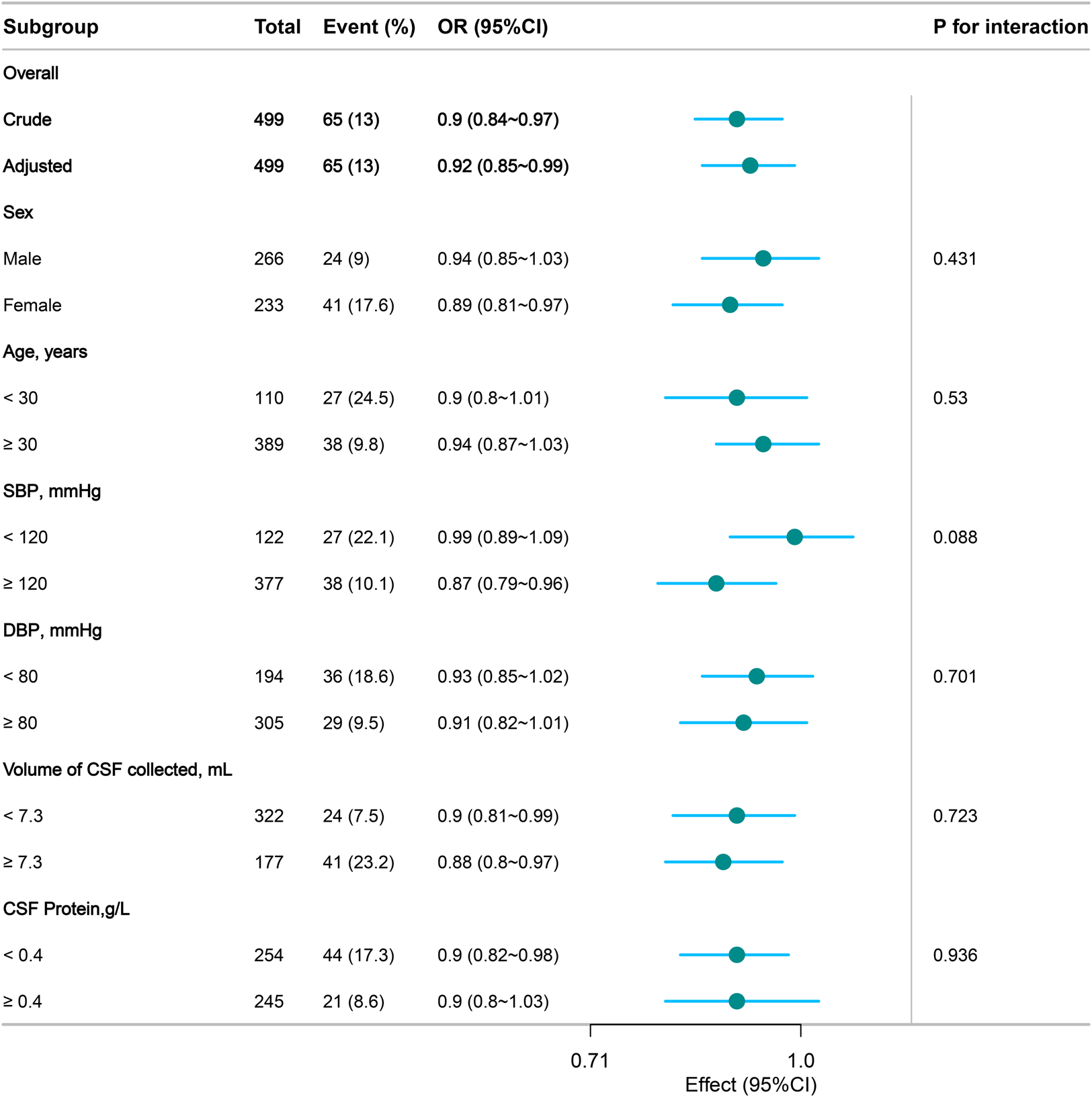
The relationship between BMI and risk of post-lumbar puncture headache risk. Except for the stratification component itself, each stratification factor was adjusted for all other variables (sex, age, SBP, DBP, CSF protein level, and CSF volume collected). As shown, no significant interaction was observed across all subgroups, suggesting that the effect of BMI on PLPH remained consistent across subgroups. BMI: body mass index; CSF: cerebrospinal fluid; SBP: systolic blood pressure; DBP: diastolic blood pressure; PLPH: post-lumbar puncture headache.
Discussion
In this study, 13% (65/499) of the patients developed PLPH, in line with the widely reported range of 3.5% to 33%.4,12 The variation in PLPH incidence across studies, including ours, may be attributed to differences in patient populations. Notably, our study included a high proportion of patients with infectious (n = 204) and immunological diseases (n = 213). Although no significant difference in PLPH incidence was found across disease categories (p = 0.164), the occurrence of PLPH was highest in the infectious disease group (34/65), suggesting that specific pathophysiological states influence susceptibility. Importantly, we identified low BMI as an independent risk factor for PLPH, a finding that aligns with several previous studies and extends the existing literature by demonstrating this association in a mixed neurological cohort.11,13 Other significant factors associated with PLPH included younger age, lower blood pressure, lower CSF protein levels, and larger volume of CSF collected during the procedure.
The pathophysiology of PLPH is believed to originate from CSF hypovolemia leading to intracranial hypotension. In adults, the total CSF volume is approximately 150 mL, with a daily production rate of 500 mL.20,21 Loss of CSF following lumbar puncture reduces the buoyant support of the brain, resulting in caudal displacement and traction on pain-sensitive intracranial structures such as the cerebral vessels and dura mater.21–23 According to the Monro–Kellie doctrine, a reduction in the CSF volume may also trigger compensatory cerebral vasodilation, further contributing to headache. 22 CSF secretion and pressure are affected by many factors, including traumatic brain injury, obstruction of the CSF pathways, cerebral edema, tumor, and infections. 24 Although neuroinflammatory conditions can increase CSF production through blood–brain barrier disruption and tissue edema,25–27 we did not observe a significant association between primary disease etiology and PLPH in this study. Several factors may explain this negative finding. First, mechanical CSF leakage from the dural puncture site, a direct and dominant trigger of PLPH may overshadow the more subtle contributions of underlying inflammatory diseases. Second, the inflammatory drive for increased CSF production might be counterbalanced by concomitant disturbances in CSF reabsorption or changes in intracranial compliance, resulting in no net effect on PLPH risk. Furthermore, the sample size, though substantial overall, may still be insufficient to detect subgroup-specific differences, particularly given the clinical and pathophysiological heterogeneity within the infectious and immunological disease categories. Finally, the timing of lumbar puncture relative to disease activity and treatment initiation may modulate CSF dynamics, thereby blurring disease-specific associations. Therefore, although inflammatory mechanisms are theoretically relevant, their effect on PLPH risk in this mixed clinical cohort appears limited compared with that of stronger predictors such as BMI and CSF volume loss. This finding underscores the multifactorial nature of PLPH and highlights the need for larger, disease-stratified studies to clarify potential etiological interactions.
A robust body of evidence supports the association between younger age and an increased risk of PLPH,4,28,29 a finding corroborated by our results showing a mean age of 35.3 years among affected patients, consistent with the common threshold of 40 years used in previous studies.30,31 This age-related susceptibility may be attributable to greater pain sensitivity or decreased dural elasticity in younger individuals. Furthermore, larger volumes of CSF collected during lumbar puncture were significantly associated with PLPH, which is mechanistically plausible given the immediate reduction in CSF volume and consistent with previous reports.32–34 Similarly, the observed link between lower blood pressure and PLPH may reflect diminished cerebral perfusion and impaired CSF regeneration post-puncture, aligning with previous findings. 34 Finally, patients with PLPH exhibited significantly lower CSF protein levels, suggesting a role of nutritional status or altered CSF synthesis in PLPH pathogenesis. Although this contrasts with a previous report that found no significant difference, 35 it underscores the need for further investigation into CSF composition as a modulator of PLPH risk.
The relationship between BMI and PLPH has been investigated in various clinical settings; however, findings have not been consistent. Our study reinforces the association between low BMI and increased PLPH risk, a finding supported by several investigations. Peralta et al.
36
reported significantly lower PLPH incidence among patients with BMI ≥31.5 kg/m2 compared with that in those with lower BMI (39% vs. 56%; p = 0.0004), whereas a Japanese study documented a protective effect of elevated BMI in both obstetric and non-obstetric cohorts.
13
Similarly, a recent prospective study by Al-Hashel et al.
29
has identified low BMI as an independent risk factor for PLPH in a cohort of 285 consecutive procedures. However, conflicting evidence exists, including a study involving Huntington’s disease patients
37
and a retrospective analysis in pregnant women
11
that found no association between BMI and PLPH. These discrepancies may be attributable to differences in study populations, sample sizes, and the prevalence of other risk factors. Mechanistically, higher BMI may confer protection through several pathways:
Increased intra-abdominal pressure reduces the transdural pressure gradient, thereby attenuating CSF leakage.
36
Enhanced epidural fat content may achieve improved sealing of the dural defect. Gravitational effects in recumbent positions may further minimize CSF effusion.
Additionally, recent evidence has suggested that adipose tissue may influence dural healing processes by secreting anti-inflammatory cytokines; 38 however, this hypothesis requires further investigation. These factors collectively support the notion that elevated BMI reduces the PLPH risk, consistent with the pathophysiological model of CSF hypovolemia following lumbar puncture.
Taken together, our study identified low BMI as a significant predictor of PLPH. Certain study limitations should be considered when interpreting these results. The cross-sectional design precludes causal inference, and the sample size, though sufficient for primary analyses, may limit subgroup interpretations. Although sensitivity analyses indicated stable results across subgroups, unmeasured confounders may persist. Variability in operator technique and experience, despite standardized protocols, could also influence outcomes. Notably, the cutting needle used for lumbar punctures in this study is associated with a higher risk of PLPH compared with atraumatic needles; 39 this procedural factor may have influenced the overall incidence observed in our study. Furthermore, although additional variables were associated with PLPH in this study these findings require validation in larger, prospective studies. Future research involving a multicenter design and detailed mechanistic assessments is needed to confirm the generalizability and biological basis of these associations. Nonetheless, our results suggest that patients with low BMI undergoing lumbar puncture may benefit from enhanced preoperative counseling and vigilant postoperative monitoring.
Footnotes
Acknowledgments
We thank Prof. Yuzhong Wang from the Department of Neurology and Clinical Medical Research Center, Affiliated Hospital of Jining Medical University, Jining, Shandong Province, China, for his critical reading and revision. We thank Ranran Niu, Lingling Liu, Lei Wang, Mengmeng Zhong, Yuwen Yang, Ying Gao, Ying Zhuo, Xiaomei Wang, Yumeng Zhao, and Qin Wang for their assistance in data collection.
Author contributions
Study concept and design: Baojun Qiao; data acquisition: Ruonan Li, Xia Liu, and Ning Yang; statistical analysis: Baojun Qiao; data interpretation: all authors; drafting the manuscript: Ruonan Li; and critical reading and revision: Baojun Qiao and Zhaoying Wu.
Data availability statement
The data are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare no competing interests.
Funding
This work was supported by the Key Research and Development Program of Jining City (2022JNZC118), Jining City Traditional Chinese Medicine Science and Technology Development Plan Project (ZYY2015026), and the Natural Science Foundation of Shandong Province (ZR2020QH110).