
Abstract
Objective
Sodium-glucose cotransporter 2 inhibitors are widely used in the management of diabetes mellitus and have demonstrated substantial cardiovascular and renal protective effects, particularly in patients with heart failure. However, their impact on cardiovascular outcomes in patients with chronic obstructive pulmonary disease remains insufficiently characterized.
Methods
We conducted a systematic review and meta-analysis of randomized controlled trials to evaluate the efficacy and safety of sodium-glucose cotransporter 2 inhibitors in patients with chronic obstructive pulmonary disease. The primary outcome was the composite cardiovascular outcome (defined as cardiovascular mortality and total hospitalization for heart failure). Secondary outcomes included all-cause mortality, cardiovascular death, hospitalization for heart failure, and adverse events.
Results
Three randomized controlled trials involving 1986 patients with chronic obstructive pulmonary disease were included; in total, 1113 patients received sodium-glucose cotransporter 2 inhibitors treatment and 873 received placebo. Compared with the placebo, sodium-glucose cotransporter 2 inhibitors significantly reduced the risk of the composite cardiovascular outcome (risk ratio, 0.76; 95% confidence interval: 0.65–0.87; p < 0.001) and hospitalization for heart failure (risk ratio, 0.69; 95% confidence interval: 0.58–0.83; p < 0.001). Although not statistically significant, trends toward reduced all-cause mortality (risk ratio, 0.89; 95% confidence interval: 0.73–1.08; p = 0.23) and cardiovascular death (risk ratio, 0.96; 95% confidence interval: 0.74–1.24; p = 0.73) were observed. The incidence of adverse events was comparable between the two groups.
Conclusions
The use of sodium-glucose cotransporter 2 inhibitors is associated with a reduced risk of composite cardiovascular outcomes and hospitalization for heart failure in patients with chronic obstructive pulmonary disease, without an increased risk of adverse events. However, given the limited number of available trials, these findings should be interpreted with caution, and further large-scale studies are warranted.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a treatable chronic airway disease characterized by persistent airflow limitation accompanied by inflammation. 1 Despite advances in management, COPD remains a major global health burden, affecting millions of individuals worldwide and contributing substantially to morbidity and mortality rates. 2 In addition to causing respiratory impairment, COPD is increasingly recognized as a complex multisystem disorder frequently accompanied by comorbidities such as heart failure (HF) and diabetes mellitus (DM), both of which considerably worsen clinical outcomes. 3
Emerging evidence suggests that COPD represents a distinct high-risk cardiometabolic phenotype. Patients with COPD have a substantially increased risk of incident cardiovascular disease (CVD), including HF, compared with those without COPD. 4 This excess risk is driven by shared risk factors such as smoking as well as overlapping pathophysiological mechanisms, including chronic systemic inflammation, oxidative stress, and accelerated biological aging. 5 In addition, persistent hypoxia and inflammatory activation in COPD may further exacerbate endothelial dysfunction and increase susceptibility to acute cardiovascular (CV) events and mortality. 6 The coexistence of DM further amplifies this risk, as hyperglycemia and metabolic dysregulation contribute to adverse pulmonary and CV outcomes, including a higher risk of acute exacerbations.7,8 Therefore, effective management of multimorbidity is critical to improving the overall prognosis and quality of life in patients with COPD.
However, the management of COPD with multiple comorbidities is often complicated by polypharmacy, which increases the risk of medication nonadherence, drug–drug interactions, and adverse drug reactions. 9 In clinical practice, the use of certain CV therapies, such as beta-blockers, remains challenging due to concerns regarding respiratory effects.10–12 Consequently, there is a growing need to identify therapeutic strategies that can simultaneously address both pulmonary and CV disease processes to reduce the treatment burden and improve clinical outcomes.
Sodium-glucose cotransporter 2 inhibitors (SGLT2is) are well established as first-line therapies for DM and have demonstrated robust CV and renal protective effects, particularly in patients with HF.13–16 Notably, their benefits extend beyond glycemic control, suggesting pleiotropic effects involving anti-inflammatory, metabolic, and hemodynamic pathways. Given these properties, SGLT2is may represent a promising therapeutic option for patients with COPD and cardiometabolic comorbidities. However, whether these benefits translate into improved CV outcomes, particularly in the COPD population, remains insufficiently characterized.
Recent studies have explored the potential role of SGLT2is in COPD. Population-based analyses have suggested that SGLT2is may reduce the risk of severe exacerbations compared with other glucose-lowering agents in patients with coexisting COPD and DM.17,18 In addition, post hoc and pre-specified analyses of major HF trials, including DAPA-HF and DELIVER, have demonstrated consistent CV benefits of dapagliflozin regardless of the COPD status.19,20 However, findings have not been entirely consistent across all agents as subgroup analyses from the EMPA-REG OUTCOME trial did not demonstrate similar benefits in patients with COPD, except for renal outcomes. 21
Given the current absence of dedicated RCTs specifically designed for COPD populations, a rigorous meta-analysis framework provides an important alternative approach for evidence generation. Such methodology enables a refined synthesis of comparative evidence and offers a systematic means to address clinically relevant questions and allows for cautious interpretation of pooled effects without overestimating therapeutic superiority. 22 Importantly, pooled analyses of COPD subgroups derived from large CV outcome trials may provide incremental insights beyond general meta-analyses that do not account for disease-specific risk profiles. Therefore, we conducted a systematic review and meta-analysis of randomized controlled trials (RCTs), incorporating trial sequential analysis (TSA), to comprehensively evaluate the CV effects of SGLT2is in patients with COPD.
Materials and methods
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines 23 and was registered with International Prospective Register of Systematic Reviews (PROSPERO) (Registration Number: CRD42024545310).
Literature search
We conducted a comprehensive search of electronic databases, including PubMed, Embase, Cochrane Library, and ClinicalTrials.gov, from their inception through 17 August 2024. The search strategy incorporated terms related to SGLT2is (including empagliflozin, dapagliflozin, canagliflozin, and ertugliflozin) and COPD. The complete search strategy has been detailed in Supplemental Table S1. Additionally, we manually screened reference lists of relevant articles to identify any missed studies.
Study selection criteria
We included eligible studies that met the following criteria: (a) enrolled patients with COPD; (b) evaluated SGLT2is use as the primary intervention; (c) compared SGLT2is to placebo or standard care; (d) reported clinical efficacy and safety outcomes; and (e) RCT or observational study. Exclusion criteria encompassed conference abstracts, case reports, single-arm studies, pharmacokinetic studies, and non-English language publications.
Screening and data extraction process
Two team members independently screened titles and abstracts and subsequently performed full-text review of potentially eligible studies. Any disagreements were resolved through discussion with a third reviewer. We extracted data on study characteristics, participant demographics, intervention details, and predefined outcomes using a standardized form.
Outcomes of interest
The primary outcome was the composite of CV outcome (defined as CV mortality and total hospitalization for heart failure (HHF)). Secondary outcomes included all-cause mortality, CV death, total HHF, and adverse events (AEs).
Quality assessment
We assessed the risk of bias in the included RCTs using the updated Cochrane RoB 2 tool. 24 Two reviewers independently evaluated each study, with discrepancies resolved via group consensus.
Statistical analyses
Meta-analyses were performed using STATA software (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC.). We calculated the risk ratio (RR) with 95% confidence interval (CI) for dichotomous outcomes using a random-effects model. Heterogeneity was assessed using Cochran’s Q test and I2 statistic, with I2 >50% or p <0.10 indicating substantial heterogeneity. We conducted leave-one-out sensitivity analyses for the primary outcome and performed subgroup analyses based on specific SGLT2is.
We employed TSA to evaluate the robustness of our findings. 25 This approach helps determine whether sufficient evidence has been accumulated to draw reliable conclusions. We set parameters for TSA, including a 5% type I error, 80% power, and a 20% relative risk reduction. The relationship between the cumulative Z-curve and TSA boundary or required information size (RIS) was examined to determine the strength of evidence.
Results
Study selection
First, we identified 412 records from PubMed (n = 31), Embase (n = 361), Cochrane Library (n = 19), and ClinicalTrials.gov (n = 1). After removing 37 duplicate records and 361 irrelevant articles based on the titles and abstracts, 14 reports were screened for eligibility. After excluding 11 studies that did not meet the selection criteria, three RCTs were included.19–21 Although some potential observational studies were retrieved, none qualified for inclusion in the final analysis. The process for selecting the studies is outlined in Supplemental Figure S1.
Bias assessment
Supplemental Figure S2 shows the risk of bias assessment. All three included RCTs were associated with an overall low risk of bias evaluated according to the criteria of the risk of bias (ROB) 2 tool.19–21
Characteristics of the included studies
Overall, three RCTs involving 1986 patients were included (Table 1).19–21Among them, 1113 patients in the study group received SGLT2is (dapagliflozin (n = 651) and empagliflozin (n = 462)) and 873 in the control group received placebo. The mean participant age was 68.8 years, and male comprised 72.8% of all included patients. HF was the most common underlying disease (n = 1401, 70.5%), followed by DM (n = 1308, 65.9%). In addition, the prevalences of atrial fibrillation, myocardial infarction, and stroke were 55.7%, 40.5%, and 13.4%, respectively. Finally, 44.0% (n = 873) of the patients had an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2. The reported prevalence of New York Heart Association (NYHA) class III/IV was 42.6% and 34.5% in the studies by Dewan et al. 19 and Butt et al., 20 respectively. Furthermore, the left ventricular ejection fraction (LVEF) was 31.6% in Dewan et al.’s study 19 and 53.9% in Butt et al.’s study. 20
Characteristics of patients enrolled in each study.
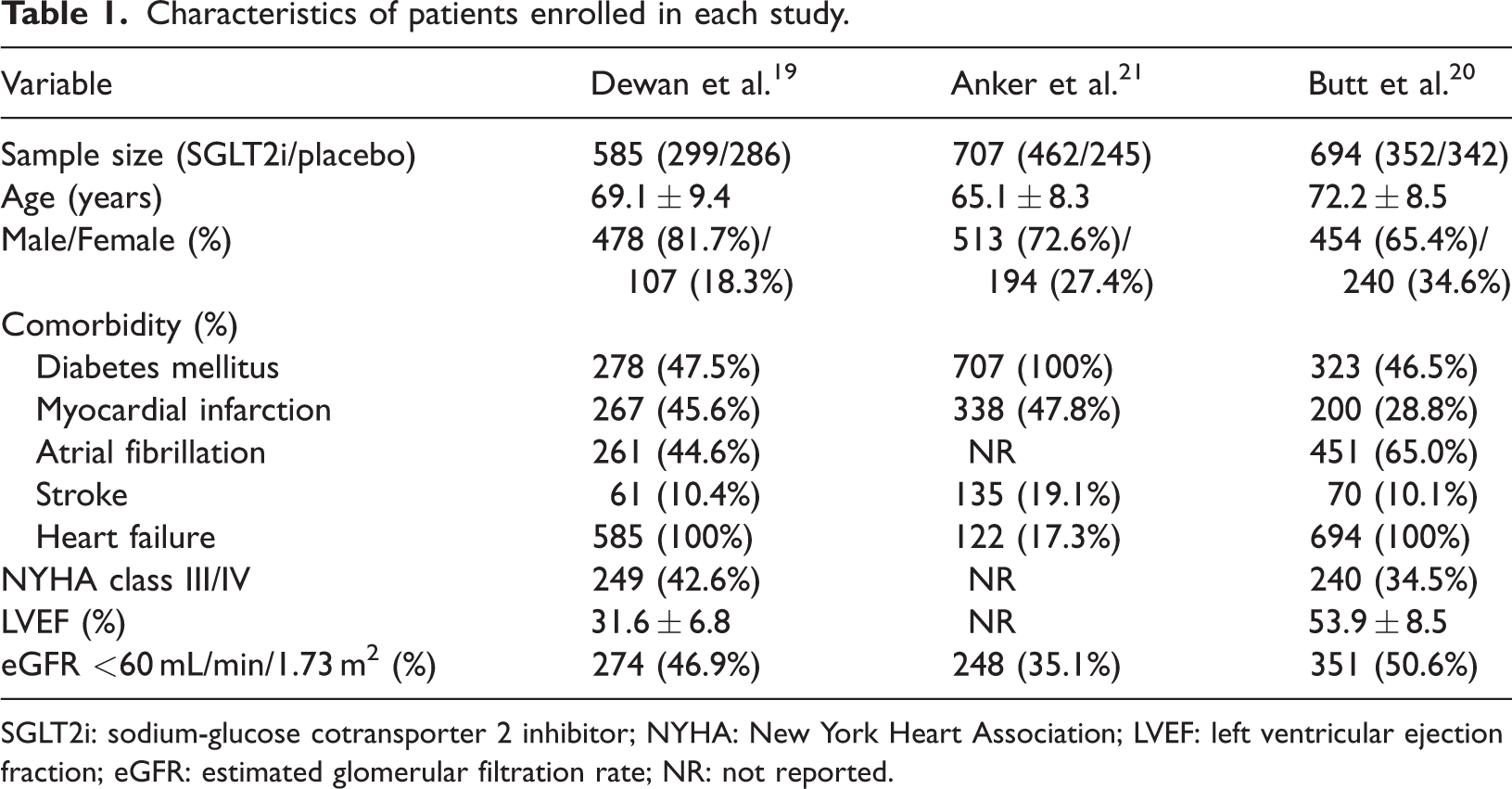
SGLT2i: sodium-glucose cotransporter 2 inhibitor; NYHA: New York Heart Association; LVEF: left ventricular ejection fraction; eGFR: estimated glomerular filtration rate; NR: not reported.
Primary outcomes
Overall, the study group had a lower risk of primary composite CV outcome than the control group (RR, 0.76; 95% CI, 0.65–0.87; p < 0.001; three studies, 1986 patients (Figure 1)) with low heterogeneity (I2 = 0%, p = 0.86). The significant difference in the risk of primary outcomes between the study and control groups remained unchanged in the leave-one-out sensitivity test in which individual studies were randomly excluded.
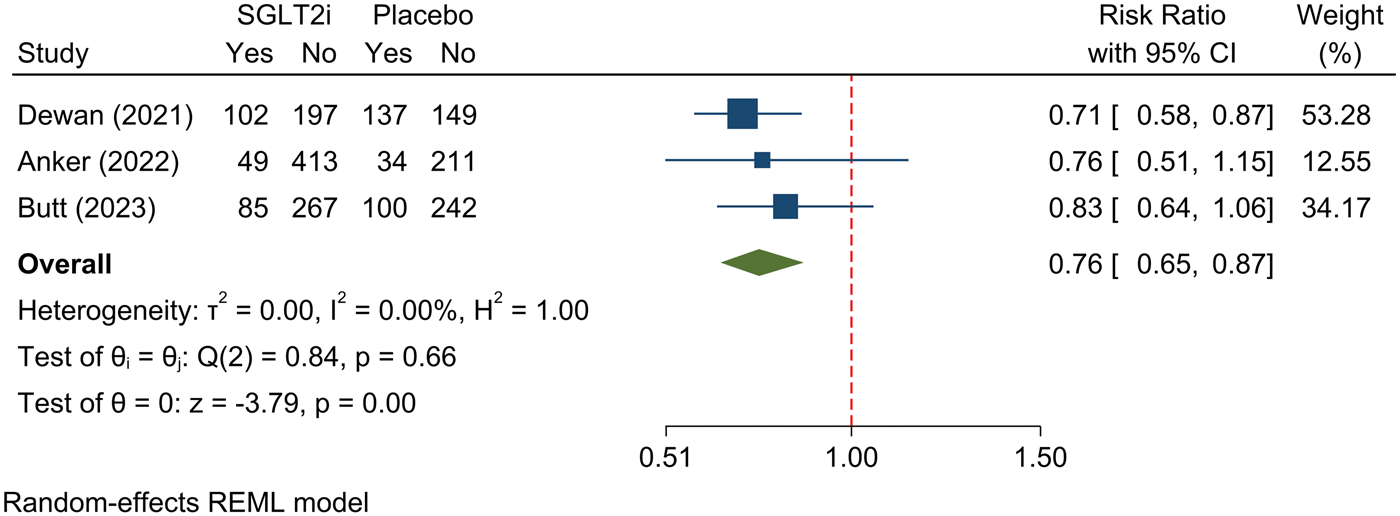
Composite cardiovascular outcome (cardiovascular mortality or hospitalization for heart failure) in patients with chronic obstructive pulmonary disease with or without sodium-glucose cotransporter-2 inhibitors (SGLT2i) use.
Further subgroup analyses revealed a similar trend; the study group had a significantly lower risk of primary outcome than the control group in the pooled analysis of patients receiving dapagliflozin and empagliflozin; however, a statistically significant difference was observed in the comparison between dapagliflozin and placebo groups with low heterogeneity (Table 2).
Subgroup analysis of the efficacy outcomes in COPD population according to different SGLT2is.
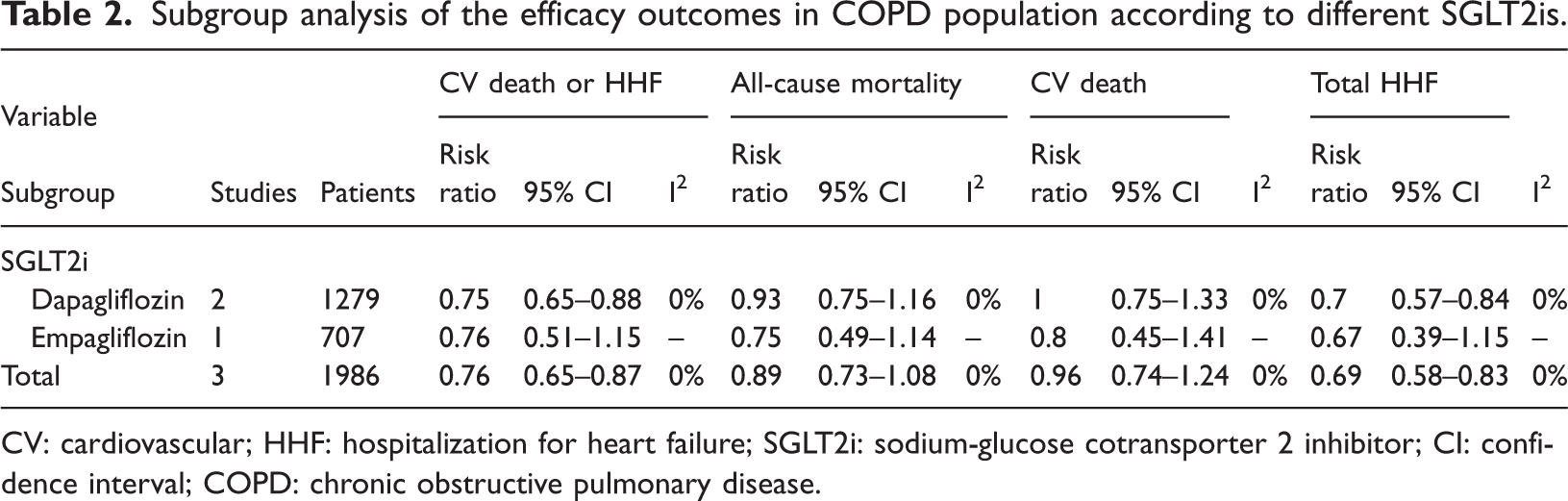
CV: cardiovascular; HHF: hospitalization for heart failure; SGLT2i: sodium-glucose cotransporter 2 inhibitor; CI: confidence interval; COPD: chronic obstructive pulmonary disease.
Secondary outcomes
Compared with the control group, the study group had a lower rate of HHF (RR, 0.69; 95% CI, 0.58–0.83; p < 0.001). Despite this, the study group was associated with a lower rate of all-cause mortality (RR, 0.89; 95% CI, 0.73–1.08; p = 0.23) and CV death (RR, 0.96; 95% CI, 0.74–1.24; p = 0.73); however, these differences did not reach statistical significance (Figure 2). A similar trend was observed in the subgroup analysis according to the types of SGLT2is (dapagliflozin and empagliflozin) (Table 2).
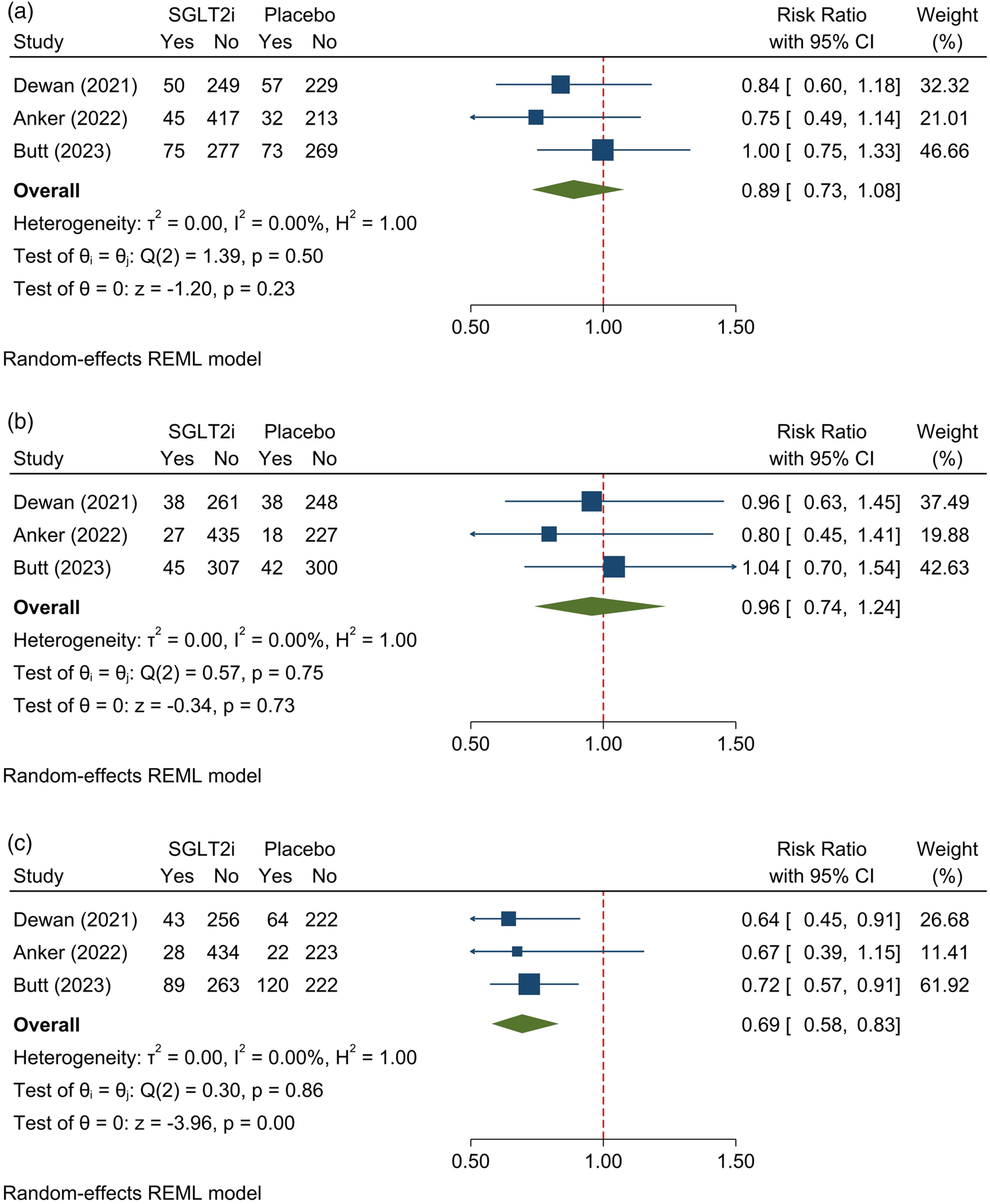
Secondary outcome in patients with chronic obstructive pulmonary disease with or without sodium-glucose cotransporter-2 inhibitors (SGLT2i) use. (a) All-cause mortality, (b) cardiovascular death, and (c) total hospitalization for heart failure.
Regarding the risk of AEs, no significant difference was observed between the study and control groups in terms of drug discontinuation due to AEs (RR, 1.04; 95% CI, 0.66–1.65), volume depletion (RR, 0.95; 95% CI, 0.67–1.36), renal-related AEs (RR, 0.79; 95% CI, 0.57–1.09), and hypoglycemia (RR, 0.91; 95% CI, 0.73–1.13) (Table 3).
Safety outcomes of SGLT2is use in the COPD population.
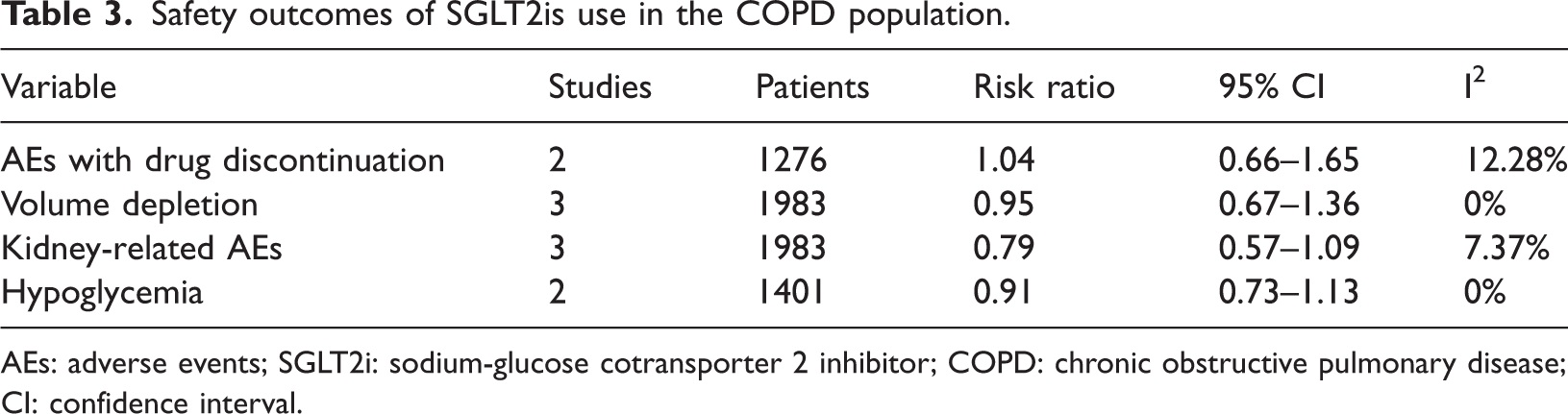
AEs: adverse events; SGLT2i: sodium-glucose cotransporter 2 inhibitor; COPD: chronic obstructive pulmonary disease; CI: confidence interval.
TSA
When applying a 20% relative risk reduction criterion, the Z-curve successfully crossed the predefined benefit boundary, indicating a statistically significant effect. Additionally, the analysis achieved the RIS of 1643 patients. TSA suggested sufficient accumulated evidence for the primary outcome (Supplemental Figure S3).
Discussion
Our study demonstrated that SGLT2is use is associated with improved CV outcomes in patients with COPD, including a 24% reduction in composite CV outcomes and a 31% reduction in HHF. Although the reduction in all-cause mortality did not reach statistical significance, the absence of heterogeneity (I2 = 0%) suggests a consistent neutral-to-favorable trend across studies. These findings indicate that SGLT2is do not confer additional mortality risk in this population and may provide survival benefit; these associations warrant further investigation. 26
In subgroup analyses, a statistically significant reduction in outcomes was observed in the dapagliflozin subgroup. However, this finding should be interpreted with caution. The comparison across agents was indirect and based on a limited number of studies with unequal sample sizes. Therefore, the observed significance likely reflects differences in the available data rather than true pharmacologic superiority. These results underscore the importance of distinguishing agent-specific findings from broader class effects in cardiometabolic disease contexts. 27
Our findings are consistent with robust evidence from large RCTs demonstrating that SGLT2is reduce the risk of HHF and CV death in patients with type 2 DM and HF, independent of glycemic control. 28 In addition, a previous meta-analysis examining CV outcomes in COPD populations has reported similar trends. 29 However, that analysis lacked key methodological components, including protocol registration, comprehensive bias assessment, and TSA. By incorporating these elements, our study provides a more rigorous and reliable synthesis of the available evidence.
COPD is increasingly recognized as an independent risk factor for adverse CV outcomes. Large-scale trials have demonstrated that COPD is associated with increased risks of both CV and non-CV hospitalizations in patients with HF. 30 Furthermore, emerging real-world evidence suggests that SGLT2is initiation may reduce overall and COPD-related hospitalizations. 31 Although our analysis demonstrated a significant reduction in HHF, we were unable to evaluate non-CV hospitalizations due to limited data availability in the included trials.
In addition to CV outcomes, SGLT2is may exert beneficial effects on pulmonary disease progression. Observational studies have suggested reductions in COPD exacerbations among SGLT2is users compared with that in patients using other glucose-lowering therapies.17,18 However, key respiratory outcomes, including exacerbation frequency, lung function (e.g. forced expiratory volume in 1 s (FEV1)), and patient-reported outcomes, were not consistently reported in the included trials and could not be analyzed in our study. Therefore, although our findings suggest potential benefits beyond CV protection, these effects require further validation in dedicated respiratory-focused studies.
From a clinical perspective, the use of SGLT2is in COPD populations is largely driven by established indications such as DM and HF.13,16 Therefore, data on COPD patients without DM remain limited. This precluded a direct assessment of whether the observed benefits are independent of glycemic status. However, available real-world evidence suggests that reductions in hospital stay associated with SGLT2is use may occur regardless of comorbid DM or HF, although these findings should be interpreted cautiously.32,33 In addition, our interaction analysis demonstrated no significant differences in treatment effects between COPD and non-COPD populations, suggesting that the relative efficacy and safety of SGLT2is are preserved, irrespective of COPD status. Importantly, these findings do not establish COPD-specific effects but support the generalizability of SGLT2is use benefits in patients with multimorbidity.
Mechanistically, the observed benefits of SGLT2is in COPD populations may be explained by overlapping cardiometabolic and inflammatory pathways. COPD and DM share a bidirectional pathophysiology characterized by systemic inflammation, oxidative stress, and metabolic dysregulation. 34 Activation of the (advanced glycation end products) AGE/receptor for advanced glycation end products (RAGE) axis and nuclear factor kappa-B (NF-κB) signaling contributes to endothelial dysfunction and impaired tissue repair, whereas suppression of phosphoinositide 3-kinase (PI3K)/protein kinase-B (PKB/Akt) signaling further exacerbates cellular injury.34,35 In COPD, chronic hypoxia, lung hyperinflation, and oxidative stress collectively promote arterial stiffness and atherosclerosis. 36 In turn, CV dysfunction, particularly left ventricular impairment, can worsen pulmonary function and exercise capacity, creating a vicious cycle of cardiopulmonary interaction. 36 Emerging experimental data also suggest that SGLT2is exert direct anti-inflammatory and antioxidative effects, including modulation of cytokine production,36–38 airway responsiveness,39,40 and inhibition of the NLRP3 inflammasome.41,42 Together, these mechanisms provide biological plausibility for the observed clinical benefits.
Several limitations should be acknowledged. First, only three RCTs were included, and no observational studies met the inclusion criteria, limiting the scope of subgroup analyses. Second, important COPD-specific outcomes, including exacerbation rates, lung function parameters, disease severity, and patient-reported outcomes, were not available. Third, detailed clinical variables such as HF subtype, LVEF, natriuretic peptide levels, glycemic control, and background therapies could not be fully assessed due to insufficient data. Finally, the included studies evaluated only dapagliflozin and empagliflozin; therefore, the generalizability of these findings to other SGLT2is requires further investigation.
Conclusions
This study provides evidence demonstrating that SGLT2is are associated with a reduction in composite CV outcomes and HHF in patients with COPD, regardless of the presence of DM or HF. Although a statistically significant reduction in mortality was not observed, the consistent neutral-to-favorable trend suggests survival benefit without increased risk.
Importantly, SGLT2is use was not associated with the occurrence of AEs affecting overall patient safety, supporting their clinical applicability in patients with COPD and multimorbidity. TSA further indicated that the evidence supporting the primary outcome is sufficient and robust. These findings position SGLT2is use as a potential cardiopulmonary-modifying therapy in patients with COPD, bridging CV and respiratory disease management.
However, given the limited availability of COPD-specific clinical indicators, including exacerbation rates and lung function parameters (e.g. FEV1), the impact of SGLT2is on respiratory outcomes remains unclear. Further large-scale, COPD-focused studies are warranted to clarify their role in this population.
Footnotes
Acknowledgments
Not applicable.
Author contributions
C.-C Lin and H.-L Sung were involved in the primary analysis. C.-C Lin, C.-C Lai, Y.-F Wei, and P.-K Fu wrote the main manuscript. C.-C Lin, P.-Y Huang, and H.-L Sung prepared the figures and tables. All authors reviewed the manuscript. All the authors discussed the results and contributed to the preparation of the final manuscript. All authors have read and approved the final manuscript.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
All datasets used and analyzed in the current study are available from the original sources of the included studies or the corresponding author on reasonable request.
Declaration of conflicts interest
All authors declare that they have no conflicts of interest.
Ethical considerations
This study did not involve human participants or animals and therefore did not require ethical approval.
Funding
This study was supported by Taichung Veterans General Hospital (TCVGH-1137308D) and the National Science and Technology Council (Taiwan) (NSTC 112-2314-B-075A-003-MY3-2).
Institutional review board statement
Not applicable.
Published materials
This article is a revised and expanded version of a poster entitled, “Impact of sodium-glucose cotransporter 2 inhibitors on cardiovascular outcome in chronic obstructive pulmonary disease: a systematic review with meta-analysis and trial sequential analysis of randomized control trial,” which was presented at 2024 Annual Congress of Taiwan Society of Pulmonary and Critical Care Medicine And Taiwan Society of Thoracic Surgeons, Taiwan Association of Thoracic & Cardiovascular Surgery Joint Conference, Tainan, Taiwan, 7–8 December 2024.
Use of artificial intelligence
None of authors used any artificial intelligence tools in this study.
Supplemental material
Supplemental material for this article is available online.