
Abstract
Primary thyroid hemangioma is a rare entity whose radiologic and intraoperative features may resemble those of a malignant disease, increasing the risk of misdiagnosis. Herein, we report a case of papillary thyroid carcinoma coexisting with a venous hemangioma that mimicked locally invasive cancer, which complicated surgical planning. A 48-year-old man presented with a thyroid nodule confirmed as papillary thyroid carcinoma. Preoperative imaging suggested extrathyroidal extension toward the esophagus and trachea, raising concern for locally invasive disease. Because vascular features were also suspected, total thyroidectomy was planned with an intraoperative reassessment of the surgical extent. Intraoperatively, the lesion was identified as a dilated vascular structure rather than an infiltrative tumor, allowing the procedure to be limited to thyroidectomy. Final histopathology confirmed papillary thyroid carcinoma with a coexisting venous hemangioma without true capsular invasion. This case highlights an important diagnostic pitfall: vascular lesions may mimic aggressive thyroid carcinoma and lead to overtreatment. A careful integration of imaging, intraoperative assessment, and pathology is essential for the appropriate management of primary thyroid hemangioma.
Background
Hemangiomas are benign vascular neoplasms that may be classified as synovial, cavernous, capillary, venous, racemose, or arteriovenous hemangiomas. 1 Venous hemangioma is a benign lesion of vascular differentiation; however, it is still controversial whether venous hemangiomas are true tumors or malformations because they generally lack definitive endothelial proliferation, which is a hallmark of true hemangiomas.2,3
Venous vascular anomalies are typically congenital and asymptomatic. 4 Owing to nonspecific radiological features, such lesions may be mistaken for malignancy if presented as a rapidly enlarging or firm mass. 5 On ultrasonography, several features including heterogeneous echogenicity, internal calcifications, or increased vascularity may further contribute to diagnostic ambiguity. Additionally, calcifications observed on imaging can be misleading, as they are commonly observed in papillary thyroid carcinoma (PTC).6,7 Such overlapping characteristics can complicate the preoperative assessment and make it difficult to determine whether surgical intervention is warranted.
Although PTC is a common malignancy, its coexistence with a venous hemangioma is rare, with only one case reported previously. 8 Herein, we describe the case of a 48-year-old man diagnosed with PTC coexisting with a venous hemangioma postoperatively. The lesion resembled extrathyroidal invasion, leading to challenges in determining an optimal surgical approach.
Case presentation
A 48-year-old man presented to our hospital for further evaluation of a thyroid nodule. Ultrasonography performed 4 years ago revealed an enlarged left thyroid lobe with a concomitant K-TIRADS category 3 lesion (1.5 cm axial, 1.8 cm sagittal). 9 Follow-up ultrasonography after 4 years demonstrated a slight increase in size (1.88 × 1.55 ×2.15 cm). Core-needle biopsy confirmed the diagnosis of PTC. The left thyroid lobe was diffusely enlarged with heterogeneous echogenicity and dilated vessels, suggesting diffuse thyroid disease (Figure 1(a) to (d)).
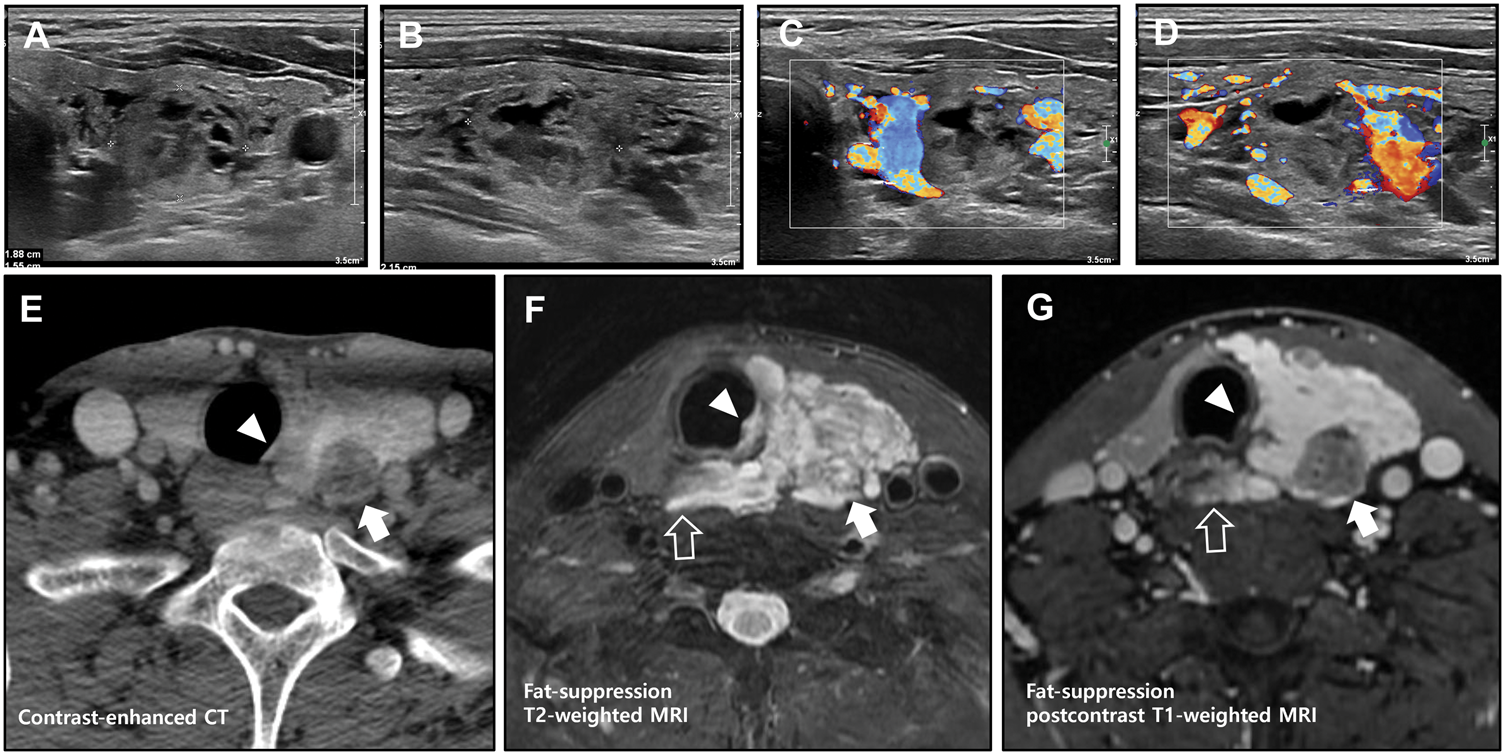
Radiologic evaluation of the thyroid gland. Ultrasonography of the left thyroid lobe shows a K-TIRADS category 3 nodule on axial (a) and sagittal (b) views. Doppler ultrasonography demonstrates heterogeneous echotexture with increased vascularity in the surrounding parenchyma (c, d). Contrast-enhanced CT (e), fat-suppressed T2-weighted MRI (f), and fat-suppressed post-contrast T1-weighted MRI (g) reveal a less-enhancing presumed PTC nodule in the left thyroid gland (arrow). The surrounding tissue abuts the trachea (arrowhead) and esophagus (open arrow), raising concern for possible direct invasion or synchronous disease.
Atypical ultrasonographic features raised concerns for the extrathyroidal extension of PTC. During neck rotation, the thyroid tissue protruded posteriorly toward the esophagus, indistinct from the adjacent structures, and could not be clearly separated from the esophagus. Multiple tubular low-echoic areas within the left lobe were suggestive of vascularity or vascular proliferative lesions. Meanwhile, no suspicious level VI metastatic lesions were detected.
Contrast-enhanced computed tomography (CECT) and magnetic resonance imaging (MRI) were performed to better delineate the extent of the disease and its relationship with the adjacent organs (Figure 1(e) to (g)). CECT and MRI revealed presumed PTC nodule with less enhancement compared with the surrounding thyroid area, which showed diffuse enlargement and heterogeneous enhancement on CECT. On CECT and MRI, the enlarged, heterogeneously enhancing portion of the left thyroid lobe appeared to involve the adjacent trachea and esophagus, raising concern for synchronous esophageal and/or tracheal carcinoma versus direct thyroid carcinoma invasion. Meanwhile, MRI showed that the surrounding region had high T2 signal and strong enhancement on post-contrast T1-weighted images, features that are clearly distinct from the presumed PTC and contralateral normal thyroid.
Therefore, given the marked vascularity on ultrasonography and relatively high T2 signal intensity on MRI, the possibility of an adjacent vascular lesion coexisting with the presumed PTC was included in the differential diagnosis.
As tracheal involvement was suspected, a bronchoscopy was performed, which revealed a focal area with prominent vascularity; however, no evidence of PTC was observed (Figure 2(a)). Biopsy revealed only inflammatory changes. Positron emission tomography showed mildly increased uptake at the thyroid nodule (maximum SUV, 2.9), whereas the adjacent infiltrative region exhibited no significant uptake; nevertheless, the possibility of malignant infiltration could not be completely ruled out.
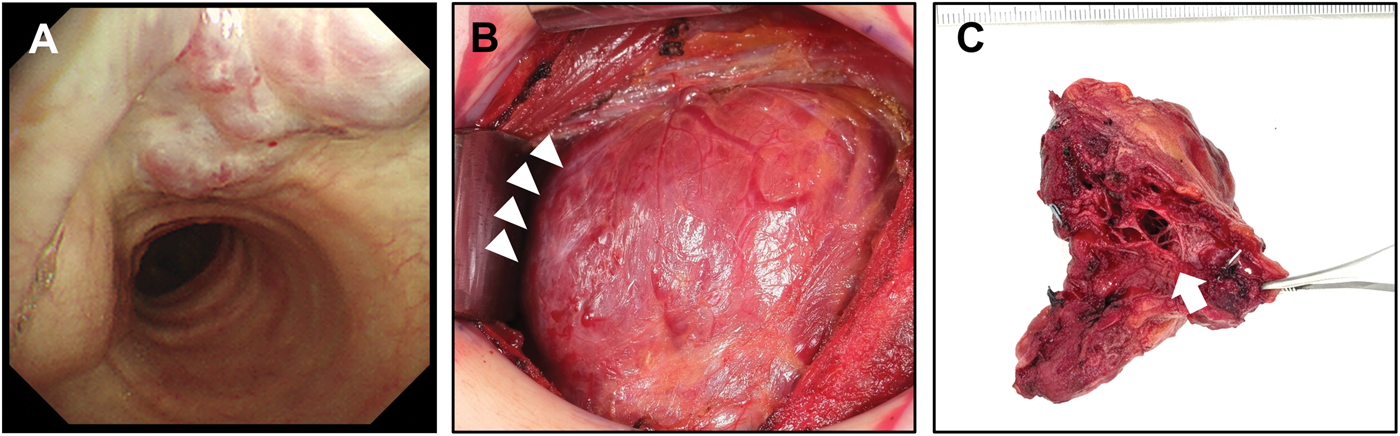
Bronchoscopic and intraoperative findings. Bronchoscopic examination shows a focal area with prominent vascularity within the tracheal lumen, with biopsy confirming the absence of papillary thyroid carcinoma (a). Intraoperative view shows a vascular lesion (arrowhead) coexisting on the surface of the left thyroid gland (b). The resected specimen viewed from the basal aspect demonstrates grossly dilated vascular structures (arrow) (c).
Taken together, the preoperative findings suggested the possibility of a vascular lesion coexisting with PTC; however, locally invasive PTC could not be ruled out. After a multidisciplinary discussion with the patient and data review, total thyroidectomy was planned, with the option to extend the procedure intraoperatively if locally invasive disease was confirmed. Total thyroidectomy was selected over lobectomy because of the potential need for postoperative radioactive iodine therapy, considering that an additional adjuvant treatment might be required depending on the final pathology, even if the disease did not appear extensive.
Intraoperatively, prominently dilated vessels were observed extending from the lateral aspect of the thyroid (Figure 2(b)). During the dissection of the posterior aspect of the thyroid, massive bleeding occurred at the lateral aspect of the cricoid cartilage and adjacent inferior region, corresponding to the vascular lesion observed on bronchoscopy. Hemostasis was achieved using 5-0 Prolene sutures and compression with hemostatic agents, after which the surgery was completed. The tissue was soft, suggesting a vascular lesion rather than PTC. The posterior portion of the thyroid, composed of markedly enlarged vascular structures, lacked a clearly definable boundary (Figure 2(c)). The patient’s hemoglobin level decreased from 15.8 g/dL preoperatively to 11.8 g/dL postoperatively but recovered to 14.4 g/dL at 3 months without transfusion.
Final pathology demonstrated two PTCs in the left lobe (1.8 × 1.6 × 1.2 cm and 0.9 × 0.6 × 0.3 cm), consistent with the infiltrative follicular subtype (2022 WHO classification). Both tumors showed minimal microscopic extrathyroidal extension, with no necrosis, lymphovascular invasion, and lymph node metastasis (pT1bN0a, AJCC on Cancer 8th edition). Additionally, a vascular lesion (6.2 × 3.2 × 1.2 cm), comprising large thick-walled muscular vessels, was identified, consistent with venous hemangioma (Figure 3). All surgical margins were tumor-free.

Histopathologic findings of papillary thyroid carcinoma (PTC) coexisting with venous hemangioma. Low-power views (25×; a–c) demonstrate the interface between PTC and venous hemangioma within the thyroid gland. High-power views (100×; d–f) correspond to the region indicated by the red square in panel A. Hematoxylin and eosin staining shows dilated vascular channels characteristic of venous hemangioma adjacent to infiltrative follicular-type PTC. Immunohistochemical staining further highlights the vascular components and tumor cells.
Based on the final pathology, the patient was classified as intermediate risk; therefore, adjuvant radioactive iodine therapy was omitted. On postoperative follow-up, the thyroglobulin level was 1.28 ng/mL at 1 month and decreased to <0.1 ng/mL at 6 months, with no recurrence.
Discussion
In this report, we used the term “venous hemangioma” to describe a lesion that is often referred to as a venous malformation. These terms are considered interchangeable, reflecting an ongoing debate regarding whether the lesion represents a true neoplasm or a developmental vascular anomaly.2,10,11
This case report describes PTC coexisting with a venous hemangioma mimicking a locally invasive disease, illustrating complex surgical decision-making. Thyroid hemangioma is a rare, benign vascular lesion presenting as a painless neck mass or remaining asymptomatic. Its radiological features are variable, often appearing as heterogeneous or hypervascular nodules,6,7 resembling malignant thyroid tumors, leading to diagnostic uncertainty. 12
A PTC arising within or with a thyroid hemangioma is exceptionally rare, with only one case reported previously; 8 however, the lesion was classified as a cavernous hemangioma. In addition, this report did not describe the preoperative findings suggesting hemangioma or features mimicking locally invasive PTC; the enlargement of the hemangiomatous component was presumed to have resulted from fine-needle aspiration performed preoperatively, leading to intraoperative bleeding without radiological diagnostic ambiguity observed in our case. Conversely, our case demonstrated preoperative imaging findings highly suggestive of extrathyroidal invasion, features typically associated with malignant neoplasms, such as angiosarcoma, thereby creating significant diagnostic and surgical challenges. 13
Despite multidisciplinary discussions and extensive diagnostic workup, malignancy could not be ruled out; however, a definitive diagnosis of locally invasive PTC had not been established. Preoperative ultrasonography and T2-weighted MRI indicated a vascular lesion, multiple tubular low-echoic areas within the thyroid parenchyma, and diffuse hypervascularity on Doppler imaging. Although not pathognomonic, these findings suggest a vascular component that may account for the atypical imaging. This highlights the importance of multidisciplinary assessment in guiding surgical planning in cases of indeterminate and confounding radiological features.
Unexpected intraoperative bleeding can occur because of the highly vascular nature of such lesions, emphasizing the importance of preoperative recognition and preparedness for meticulous hemostatic control. 14 The preoperative identification of these vascular lesions is important because they may represent arteriovenous malformations that can lead to massive intraoperative hemorrhage. In a previous case report, the blood loss during left hemithyroidectomy was approximately 2000 mL, necessitating whole blood transfusion. 14 Therefore, awareness of this potential risk reinforces the need for careful preoperative evaluation and surgical planning in patients presenting with hypervascular thyroid lesions.
Histopathologically, venous hemangiomas are characterized by irregular, variable-sized vascular channels with flat endothelial lining and smooth muscle walls. CD31 and CD34 serve as useful immunohistochemical markers for confirming the vascular origin of such lesions, while smooth muscle actin highlights the vascular smooth muscle walls. 15 Currently, these characteristic histopathological and immunohistochemical findings confirmed the diagnosis of a venous hemangioma coexisting with PTC. Subsequent management was guided by the staging and standard treatment protocols for PTC.
Conclusion
This case illustrates the rare coexistence of PTC and venous hemangioma of thyroid. The hemangioma showed radiological and intraoperative findings suggestive of extrathyroidal invasion, making it difficult to determine the appropriate extent of surgery. The recognition of vascular lesions as potential mimickers of invasive thyroid carcinoma is crucial for accurate clinical decision-making. Multidisciplinary evaluation and meticulous correlation of imaging, intraoperative findings, and histopathology are essential to avoid unnecessarily extensive surgery and achieve optimal patient outcomes in such diagnostically challenging cases.
Footnotes
Author contribution
Jong Woo Lim: Conceptualization, Validation, Writing–Original Draft
Hyun Seong Kim: Resources, Validation, Writing–Original Draft
Yoo Hyung Kim: Resources, Validation, Writing–Reviewing and Editing
Kyeong Cheon Jung: Resources, Validation, Writing–Original Draft
Ji-hoon Kim: Project administration, Supervision, Writing–Reviewing and Editing
Jungirl Seok: Conceptualization, Funding acquisition, Writing–Reviewing and Editing
Data availability
The patient data are not available as patient consent for the sharing of personal information was not obtained.
Declaration of conflicting interest
The authors have no financial conflicts of interest to disclose.
Ethics approval and consent to participate
The case was reported based on a prospective registry, using informed consent from patients approved by the IRB of Seoul National University Hospital (IRB No. 2109-043-1253).
Funding
This study was supported by the National Research Foundation of Korea Grant funded by the Korean Government (Grant No. NRF-RS-2023-00210922) and the Seoul National University Hospital (SNUH) Research Fund (Grant Nos. 0320230120 and 3020250190).