
Abstract
This study reports two cases of Vogt–Koyanagi–Harada disease recurrence after laser treatment. Case 1 involved a woman in her late 70s with Vogt–Koyanagi–Harada disease that was controlled by adalimumab and steroid eye solution therapy. She presented with uveitis recurrence 4 weeks after undergoing neodymium:yttrium aluminum garnet laser posterior capsulotomy in both eyes. She was immediately treated with sub-Tenon triamcinolone acetonide injection in both eyes, which provided palliative relief. During the following year, she experienced further recurrences every 3–5 months. Case 2 involved a woman in her 40s with Vogt–Koyanagi–Harada disease and untreated type 2 diabetes. She had undergone pulse steroid therapy 3 months ago. She was prescribed insulin and oral diabetic medicine. The sudden glycemic control caused progression of her diabetic retinopathy, which was treated with retinal photocoagulation of the left eye. Three days later, there was recurrence of bilateral serous retinal detachment. She was immediately treated with sub-Tenon triamcinolone acetonide injection in both eyes, which improved serous detachment. Additional retinal photocoagulation was performed in both eyes 18 months later. These cases suggest that laser treatment triggers recurrence of Vogt–Koyanagi–Harada disease. Further investigation of this association is warranted.
Keywords
Introduction
Vogt–Koyanagi–Harada (VKH) disease is a bilateral, diffuse granulomatous uveitis. It presents with poliosis, vitiligo, alopecia, and central nervous system and auditory symptoms. The vision outcomes in VKH disease are generally favorable. In a previous study, we found that decimal corrected visual acuity 12 months after pulse steroid therapy was >1.0 in 139 eyes of 70 patients with VKH disease. 1
However, in cases that remain uncontrolled for long periods and those with recurrent inflammation, vision-threatening complications, including cataract, glaucoma, choroidal neovascularization, and subretinal fibrosis, can result in ocular morbidity. 2 Final visual acuity shows a strong, inverse correlation with the occurrence and number of complications (p = 0.001) as well as the number of recurrent inflammatory episodes (p < 0.001). 2 Thus, both inflammation control and recurrence prevention are crucial.
Both retinal photocoagulation for fundus disease and neodymium (Nd):yttrium aluminum garnet (YAG) laser posterior capsulotomy for post-cataract complications are widely performed procedures. However, we encountered two cases of VKH disease in which serous retinal detachment (SRD) recurred after retinal photocoagulation performed for rapidly progressing diabetic retinopathy and Nd:YAG laser posterior capsulotomy performed after cataract surgery. To the best of our knowledge, no case of VKH disease recurrence after laser treatment has been reported. Herein, we provide a detailed description of such recurrences.
Case report
Case #1
Case 1 involves a woman in her late 70s who had undergone pulse steroid therapy 52 months ago for naïve VKH disease during the coronavirus disease 2019 (COVID-19) pandemic at Dokkyo Medical University Saitama Medical Center. Pulse steroid therapy was initiated with intravenous methylprednisolone (Solu-Medrol; Pfizer, New York, New York) (1000 mg/day for 3 days) followed by oral prednisolone (Predonine; Shionogi, Osaka, Japan). Oral prednisolone was started at 40 mg/day and tapered by 5 mg/day every 3–4 weeks. Her eye condition progressed to chronic iritis; therefore, treatment with adalimumab injection and steroid eye solution was continued. She later exhibited progression of her posterior subcapsular cataracts. Therefore, 18 months after presentation, she underwent phacoemulsification cataract surgery in both eyes. Postoperatively, subretinal fibrosis was detected in her left eye. However, her chronic iritis was well controlled. Therefore, after 7 months, further follow-up was conducted at her previous eye clinic. Six months after this, she underwent Nd:YAG laser posterior capsulotomy in both eyes at this eye clinic. At that time, more than 1 year had passed since her last COVID-19 vaccine. Four weeks later, she presented at Dokkyo Medical University Saitama Medical Center again due to a decrease in visual acuity. Bilateral and symmetrical SRD recurrence, iritis, and thickened choroids in both eyes were detected (Figure 1). Her decimal visual acuity was 0.08 in the right eye and 0.01 in the left eye. We immediately administered sub-Tenon triamcinolone acetonide (STTA) injections in both eyes. Although her decimal visual acuity had improved to 0.6 in the right eye and 0.03 in the left eye 3 weeks after the STTA injections, she suffered SRD and iritis recurrence every 3–5 months in the following year. During this time, we administered STTA injections in both eyes on two more occasions. We also observed that the required interval between subsequent adalimumab therapy doses had shortened.

Optical coherence tomography images of a woman in her late 70s, taken 4 weeks after neodymium. YAG laser posterior capsulotomy was performed in both eyes previously at an eye clinic. Recurrence of serous retinal detachment (SRD) was observed in both eyes. YAG: yttrium aluminum garnet.
Case #2
A woman in her late 40s received pulse steroid therapy for naïve VKH disease before the COVID-19 pandemic at Dokkyo Medical University Saitama Medical Center. Her initial corrected decimal visual acuity was 0.3 in the right eye and 0.08 in the left eye. Pulse steroid therapy was initiated with intravenous methylprednisolone (1000 mg/day for 3 days) followed by oral prednisolone. Oral prednisolone was started at 40 mg/day and was tapered by 5 mg/day every 3–4 weeks. Blood test revealed naïve severe diabetes and dyslipidemia. The patient’s glycated hemoglobin (HbA1c) level was 10.8%. Physicians at our hospital prescribed internal medication and administered insulin injections. The patient’s HbA1c level decreased to 6.7% over the subsequent 3 months. This caused rapid progression of her diabetic retinopathy. Specifically, although simple diabetic retinopathy was observed in both eyes at the initial visit, preproliferative retinopathy developed 3 months later. Retinal photocoagulation was performed for her left eye. The photocoagulation parameters were as follows: PASCAL SLIM LINE (OptiMedica Inc., Santa Clara, CA, USA), 407 shots, 575 mW, 0.02 s. The patient returned to our hospital 3 days after the procedure complaining of decreased vision in both eyes. Her corrected decimal visual acuity was 0.08 in the right eye and 0.1 in the left eye. Bilateral recurrence of SRD (Figure 2(a)) and mild iritis were observed. We immediately administered bilateral STTA injections. Her corrected decimal visual acuity improved to 0.7 in both eyes, and the severe SRD had almost resolved 2 weeks later (Figure 2(b)).
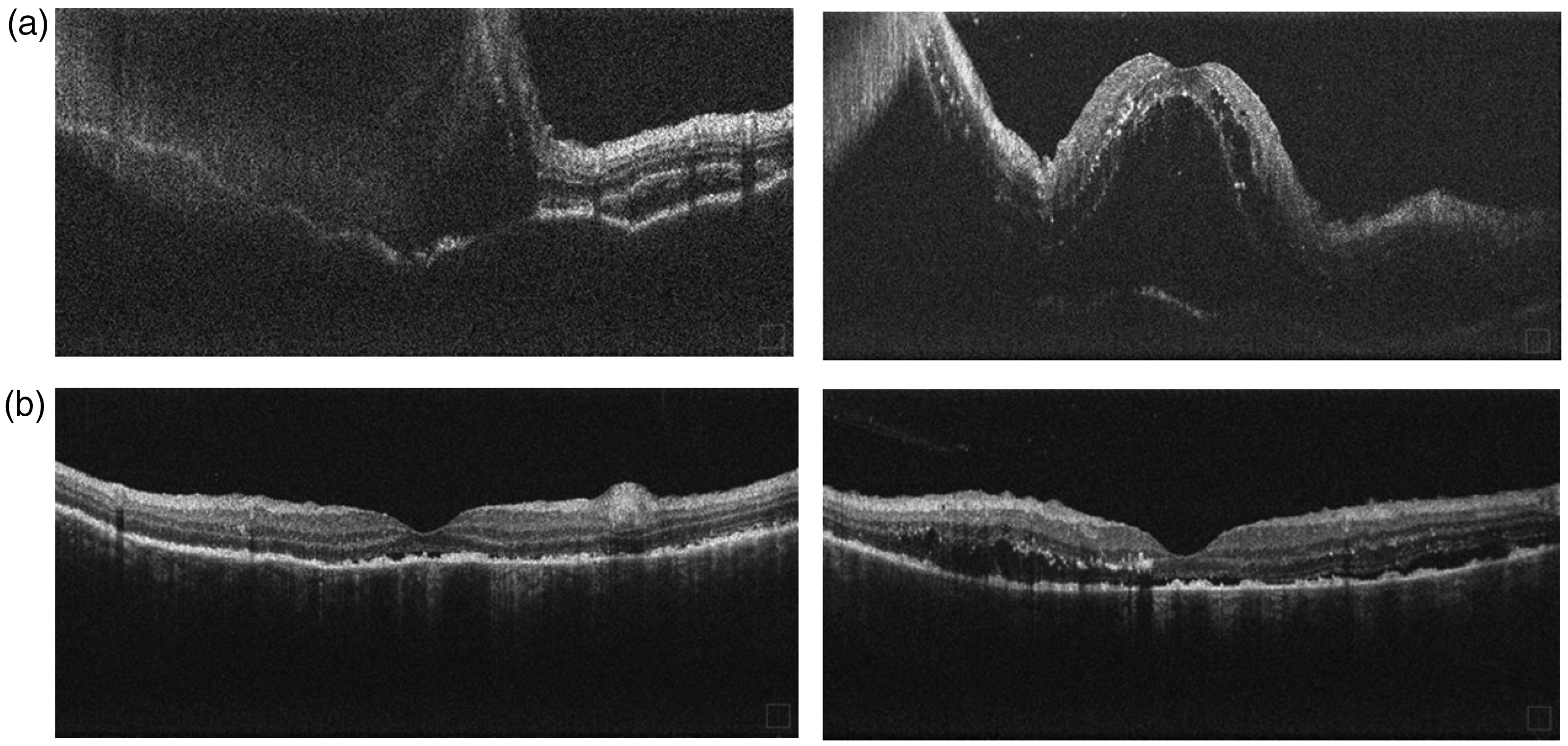
(a) Optical coherence tomography images of a woman in her late 40s taken 3 days after retinal photocoagulation for rapidly progressing diabetic retinopathy. (b) Absence of serous retinal detachment at 2 weeks after sub-Tenon triamcinolone acetonide injections in the female patient in her late 40 s.
She underwent phacoemulsification cataract surgery in both eyes at another clinic 14 months later and additional pattern scanning laser (PASCAL) treatment in both eyes at our hospital 21 months after her initial visit. Her HbA1c level increased from 8% to 11%. Her decimal visual acuity changed from 0.7 to 1.0. It was unclear whether the chronic iritis was caused by her diabetes or VKH disease. As the chronic iritis was mild, we did not administer adalimumab injections. The reporting of this study confirms to the Case Report (CARE) guidelines. 3
We have deidentified all patient details.
The patients provided written informed consent for treatment. The study protocol adhered to the tenets of the Declaration of Helsinki (1975, as revised in 2024) and was approved by the Ethics Committee of Dokkyo Medical University Saitama Medical Center (approval number 25099). Owing to the retrospective nature of the study, the requirement for publication consent of this report was waived by the Ethics Committee of Dokkyo Medical University Saitama Medical Center.
Discussion
Retinal photocoagulation involves risk of retinal and choroidal inflammation. Steinert et al. have reported 11 cases (1.23%; 95% confidence interval (CI), 0.51%–1.95%) where the patient developed cystoid macular edema after Nd:YAG capsulotomy. 4 Herbort has reported the case of a 66-years-old woman who developed severe and recurrent scleritis and uveitis after undergoing Nd:YAG capsulotomy 18 months after cataract extraction. 5 Hollander et al. have reported a case of late-onset Corynebacterium endophthalmitis following laser posterior capsulotomy. 6 Taken together, Nd:YAG capsulotomy may induce inflammation in the retina and vitreous cavity. However, we performed a PubMed search covering the period between 1 January 1980 and 1 July 2025 and found no studies on the topics of retinal photocoagulation, Nd:YAG laser posterior capsulotomy, or VKH disease recurrence. Therefore, the relationship between these three factors is unclear. Nevertheless, it is possible that laser treatment triggers recurrence.
VKH disease is a systemic disorder of unknown origin and is considered a specific autoimmune disease targeting melanocytes. This disease most frequently occurs in individuals with darker skin color, including the Japanese population. The primary sites of inflammation are tissues rich in melanocytes, such as the eyes, meninges, ears, skin, and hair. During the acute stage, melanocytes and many lymphocytes infiltrate and cause inflammation in the target tissues. Most melanocytes are lost during the convalescence stage. These clinical and pathological findings suggest that VKH disease is an autoimmune disease for melanocytes. 7 Human leukocyte antigen-DR4 (HLA-DR4) positivity is commonly observed in patients with VKH disease. 7
We found several reports of patients with coexisting VKH disease and diabetes;8,9 therefore, there must have been cases of patients who required retinal photocoagulation during therapy for VKH disease. However, none of these studies have reported VKH disease recurrence after retinal photocoagulation.
In Case 2, the patient was treated with steroid pulse therapy at the Department of Ophthalmology and glycemic control therapy at the Department of Diabetic Tract Medicine at our hospital. Her HbA1c level decreased approximately 4% every 3 months, which led to diabetic retinopathy progression. Retinal hemorrhages and soft exudates increased markedly within only 3 months after the initiation of pulse steroid therapy. This may have been a consequence of both diabetic retinopathy and VKH disease being unstable.
In Case 2, the recurrence occurred only 3 days after photocoagulation, suggesting a plausible temporal association. In contrast, in Case 1, recurrence was observed 4 weeks post laser treatment. This difference is interesting from the research point of view. Papasavvas et al. reported that the COVID-19 vaccine might have triggered VKH disease recurrence. 10 However, because the recurrence in Case 2 occurred before the COVID-19 pandemic, we can conclude that the COVID-19 vaccine did not play a role in this case. In Case 1, more than 1 year had passed since the final COVID-19 vaccination, making it difficult to establish a clear correlation. We also considered potential confounding factors, including systemic inflammation, and changes in medication, which may have contributed to the observed differences. More than 3 years had passed since the completion of pulse steroid therapy in Case 1, and the patient was receiving regular adalimumab treatment. In Case 2, oral prednisolone (30 mg/day) was administered, and adalimumab was not used. These differences may have acted as additional confounding factors.
VKH disease, systemic steroid treatment, and STTA are known to cause cataract progression.1,11 Ganesh et al. have reported that among patients with VKH disease, posterior capsule opacification developed in 38 eyes (76.0%), of which 21 (42.0%) required Nd:YAG laser posterior capsulotomy. 11 Reactivation of the disease occurred in 28 eyes during the postoperative period. 11 These might have included instances of VKH disease recurrence that went unnoticed as Ganesh et al. did not consider the possibility of a relationship between VKH disease recurrence and Nd:YAG laser posterior capsulotomy. 11
The development of VKH disease is rare. 12 Moreover, cases complicated by post-cataract events or diabetic retinopathy are uncommon, which may explain the absence of previous reports on this topic. As indicated by our findings, ophthalmologists should consider that unprepared laser treatment may act as a trigger for disease recurrence.
This study has certain limitations. Laser treatment cannot be confirmed as the cause of recurrence; the association observed in these cases might be a coincidence. Furthermore, the sample size was limited to two, which reduced the reliability of our results. To further clarify the present results, we will continue to treat VKH disease and monitor similar cases in the future.
We have described two cases of VKH disease recurrence after Nd:YAG laser posterior capsulotomy and retinal photocoagulation. The relationship between the laser treatment and VKH disease recurrence is unclear. In the meantime, careful considerations should be given to the use of laser treatment in patients with VKH disease such as perioperative systemic steroid cover, interval extension of biologics, and strict adherence to imaging surveillance protocols.
Footnotes
Acknowledgments
The authors thank Enago for assistance with English editing.
Author contributions
Tetsuya Muto wrote the main manuscript text and prepared all figures. All authors reviewed the manuscript.
Data availability statement
The datasets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest regarding the publication of this article.
Funding
The authors received no funding support.