
Abstract
Here, two cases involving the oldest reported patients with sympathetic ophthalmia (SO) after non-complicated cataract surgery, are reported. The first case was an 85-year-old female with bilateral decreased vision and headache. The best-corrected visual acuity (BCVA) was 0.8 in the right eye and 1.0 in the left eye at the initial visit. Pseudophakia and choroidal detachments were observed in both eyes, and retinal pigment epithelium undulation was observed by optical coherence tomography. The second case was a 90-year-old male with bilateral optic disc oedema. The BCVA was 0.09 in the right eye and 0.3 in the left eye with pseudophakic eyes. Optic disc oedema and choroidal thickening were observed in both eyes. Both patients were diagnosed with SO, and corticosteroid pulse treatments were started. The BCVA of the first case improved to 0.9 in the right eye and 1.2 in the left eye, while that of the second case reached 0.3 in the right eye and 0.6 in the left eye. No recurrence was observed in either case at 12 months after the initial visit. Both elderly patients with SO were successfully treated.
Keywords
Introduction
Sympathetic ophthalmia (SO) is defined as bilateral granulomatous uveitis that occurs after a penetrating ocular trauma or intraocular surgery in one eye. SO resembles Vogt–Koyanagi–Harada (VKH) disease, with autoimmune responses to melanocytes commonly playing a role in the occurrence of both diseases. SO is a rare disease, with an incidence of 0.2–0.5% after injury and 0.01% after intraocular surgery. 1
Presently, more than 1.5 million cataract surgeries are performed every year in Japan, 2 and about 150 patients are diagnosed with SO annually according to a previous report. 1 To the best of our knowledge, only two cases of SO have been previously reported in the over 80-year-old worldwide population, according to a search of the PubMed (keywords, ‘cataract’, ‘SO’; search years, 2000–2022) and CiNii Research (keywords, ‘VKH’, ‘SO’; search years, 2000–2022) databases.3,4 Chan et al. 3 reported an 80-year-old female with SO after eye trauma, while Kobayashi et al. 4 reported an 84-year-old female with SO after a non-complicated cataract surgery, but this case was reported as VKH disease. 4 To diagnose VKH disease, a history of penetrating ocular trauma or ocular surgery preceding the onset of uveitis must be excluded, according to international diagnostic criteria. 5 Therefore, the case described by Kobayshi et al. 4 should have been diagnosed as SO, and is the oldest previously reported case.
Herein, the cases of an 85-year-old female and 90-year-old male with SO following non-complicated cataract surgery are described, with the detailed clinical picture provided for each case.
Case reports
Case 1
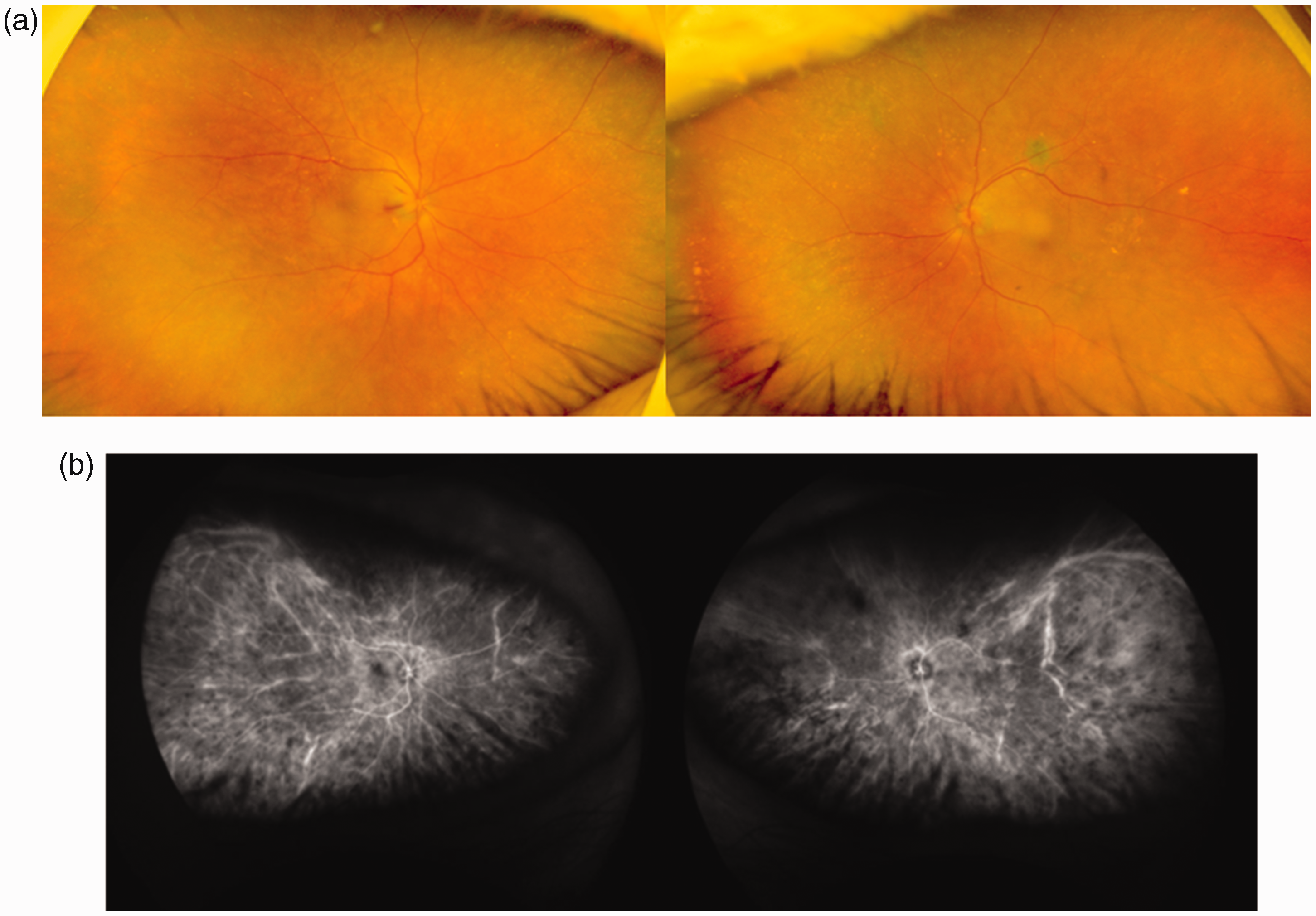
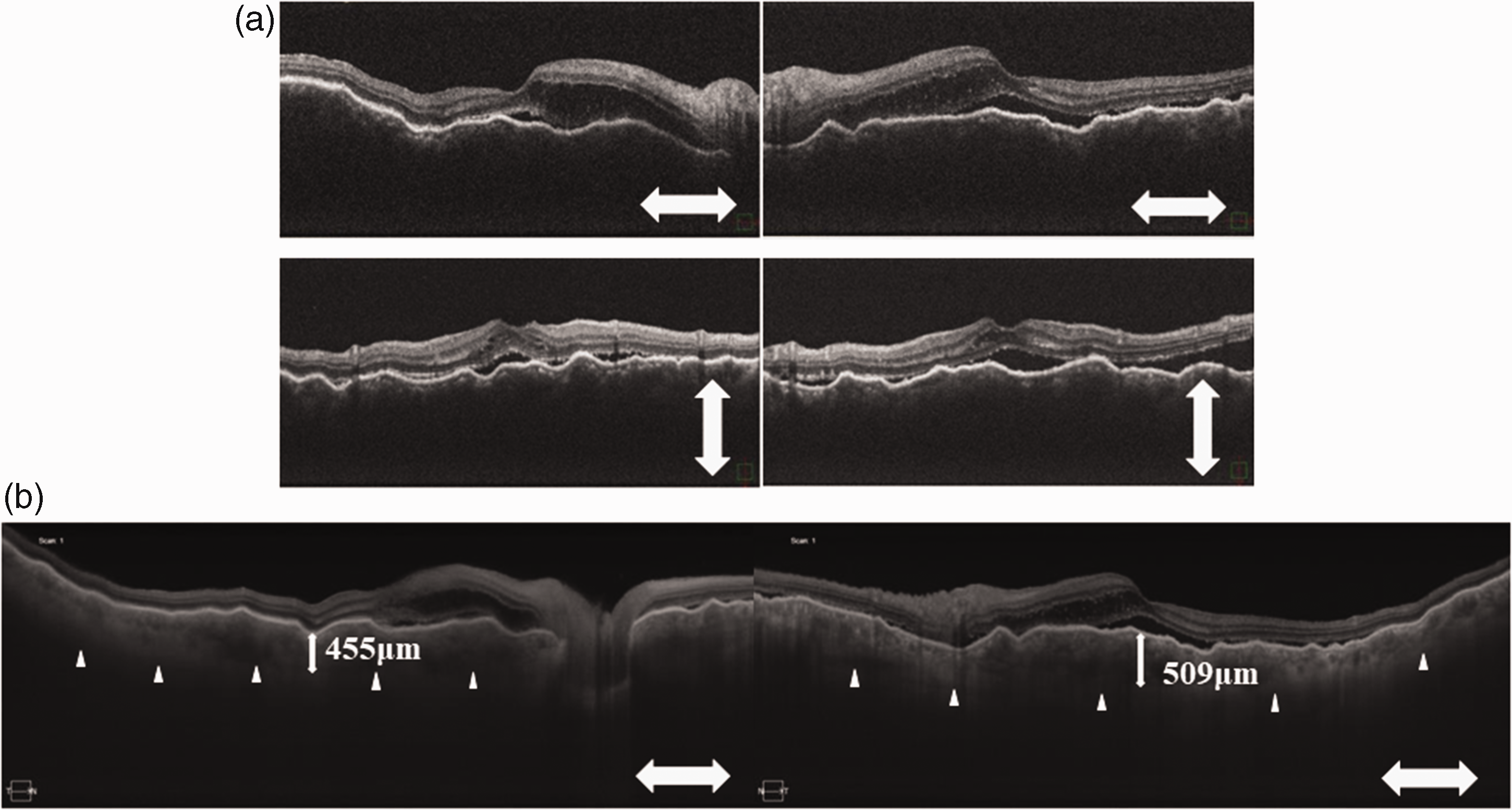
An 85-year-old female patient presented at Dokkyo Medical University Saitama Medical Centre, Koshigaya, Japan in April 2020, with decreased vision in both eyes after a non-complicated bilateral cataract surgery 13 years previously. She also had headache, and she had been diagnosed with VKH disease at a previous eye clinic. On her initial visit, the best-corrected visual acuity (BCVA) was 0.8 in the right and 1.0 in the left eye, and intraocular pressure was normal in both eyes. Slit-lamp biomicroscopy showed that the iris had pseudoexfoliation deposits, pseudophakia with posterior capsulotomy, and cells in the vitreous cavity in both eyes. Fundus examination revealed choroidal detachments in both eyes (Figure 1a). During indocyanine green angiography (ICGA), choroidal veins were found to be obscured at the posterior pole (Figure 1b). Optical coherence tomography (OCT) demonstrated retinal pigment epithelium undulations (Figure 2a) and choroidal thickening (Figure 2b) in both eyes. The axial length was 22.85 mm in both eyes. Blood test results were within normal limits, except triglyceride and leucocyte levels (148 mg/dl and 8.8 × 109 cells/l, respectively). The glycosylated haemoglobin (HbA1c) level was 5.7%.

Eye examination images from an 85-year-old female patient with decreased vision in both eyes following non-complicated bilateral cataract surgery 13 years previously: (a) fundoscopy images showing choroidal detachments in both eyes; and (b) indocyanine green angiography images showing vague choroidal veins in the posterior pole of the fundi of both eyes.

Optical coherence tomography images from an 85-year-old female patient with decreased vision in both eyes following non-complicated bilateral cataract surgery 13 years previously, showing: (a) retinal pigment epithelium undulations in both eyes; and (b) choroidal thickenings in both eyes.
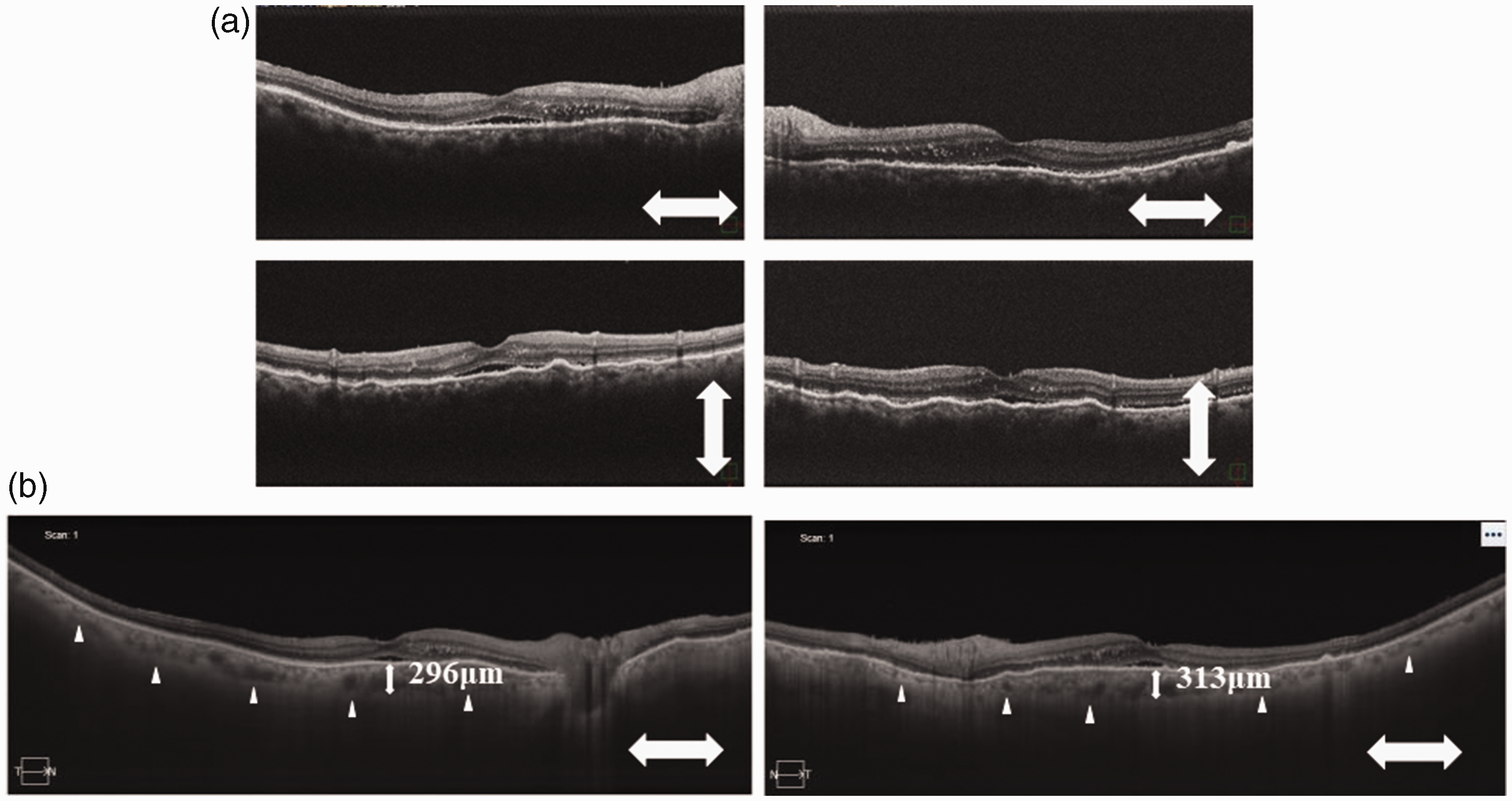
The clinical diagnosis was SO following a non-complicated cataract surgery. The patient was immediately treated by 1000 mg methylprednisolone (Solu-Medrol; Pfizer, New York, NY, USA) infusion, daily, for 3 days, followed by oral administration of 40 mg prednisolone (Predonine; Shionogi, Osaka, Japan), daily, which was gradually tapered off over the subsequent 6 months. During steroid therapy, the choroidal detachments disappeared after 1 week in the right eye and 2 months in the left eye. The HbA1c level had increased to 7.8% 3 months later (considered to be steroid-associated diabetes mellitus), and hypoglycaemic drugs were started. Although retinal pigment epithelium undulations improved (Figure 3a), the choroid remained thick at 6 months after therapy (Figure 3b). The BCVA improved to 0.9 in the right and 1.2 in the left eye. Sunset glow fundus was not observed until 12 months after the initial visit.

Optical coherence tomography images, obtained at 6 months after steroid therapy, from an 85-year-old female patient who presented with decreased vision in both eyes following non-complicated bilateral cataract surgery 13 years previously, showing: (a) almost flat retinal pigment epithelium in both eyes; and (b) reduced choroidal thickenings in both eyes.
Case 2
A 90-year-old male patient attended a local ophthalmologist clinic due to a 1-week history of decreased vision in both eyes. Ophthalmoscopy at that time revealed optic disc swelling. The patient had a history of cataract surgeries in both eyes 15 years previously. At 13 days following symptom onset, he was referred to Dokkyo Medical University Saitama Medical Centre for further examination. On the initial visit, the BCVA was 0.09 in the right eye and 0.3 in the left eye. Slit-lamp biomicroscopy examination revealed pseudophakia, and vitreous cells in both eyes. Fundus examination showed bilateral swollen discs and shallow serous retinal detachments (Figure 4a), and in ICGA, choroidal veins were obscured at the posterior pole (Figure 4b). The OCT images of both eyes revealed serous retinal detachments and retinal pigment epithelium undulations (Figure 5a), and choroidal thickening (Figure 5b). The axial length was 24.68 mm in the right eye and 24.35 mm in the left eye. Although his blood test results were almost normal, his red blood cell count, and haemoglobin and haematocrit levels, were slightly decreased, at 3.30 × 1012/l, 10.9 g/dl and 33.8%, respectively. His HbA1c level was 5.4%.
Eye examination images from a 90-year-old male patient with decreased vision in both eyes, and a history of bilateral cataract surgery 15 years previously: (a) fundoscopy images showing swollen discs in both eyes; and (b) indocyanine green angiography images showing unclear appearance of choroidal veins in the posterior poles of the fundi of both eyes.
Optical coherence tomography images from a 90-year-old male patient with decreased vision in both eyes, and a history of bilateral cataract surgery 15 years previously, showing: (a) retinal pigment epithelium undulations and slight serous retinal detachments in both eyes; and (b) choroidal thickenings in both eyes.
The patient was diagnosed with SO, and treatment was initiated with 1000 mg methylprednisolone, intravenously, daily, for 3 days, followed by 40 mg oral prednisolone, daily, which was gradually tapered off over the subsequent 6 months. The retinal pigment epithelium undulations improved (Figure 6a) and choroidal thickness reduced dramatically 1 week after initiation of therapy (Figure 6b). The BCVA improved to 0.1 in the right eye and 0.5 in the left eye at 1 month after therapy initiation. The shallow serous retinal detachments and retinal pigment epithelium undulations also disappeared. His HbA1c level changed slightly to 5.7% at 1 month, 6.1% at 2 months, and 5.9% at 4 months after therapy initiation. At 1 year following treatment, fundus examination revealed no apparent sunset glow fundus in either eye, and the BCVA had further improved to 0.3 in the right eye and 0.6 in the left eye. Ocular inflammation relapse and treatment side-effects were not observed.
Optical coherence tomography images, obtained after 1 week of steroid therapy, from a 90-year-old male patient who presented with decreased vision in both eyes, and a history of bilateral cataract surgery 15 years previously, showing: (a) reduced retinal pigment epithelium undulations and reduction in slight serous retinal detachments in both eyes; and (b) dramatically reduced choroidal thickenings in both eyes.
Written informed consent to treatment was obtained from each patient. The study protocol conformed to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Dokkyo Medical University Saitama Medical Centre (approval No. 21125). The need for informed consent for publishing was waived by the Ethics Committee of Dokkyo Medical University Saitama Medical Centre, due to the retrospective nature of this study. The reporting of this study confirms to CARE guidelines. 6
Discussion
To the best of our knowledge, the present study describes the oldest reported patients with SO from anywhere in the world. The present cases were not typical, particularly case 1; therefore, differential diagnoses were important. The differential diagnoses included VKH disease, SO, and uveal effusion syndrome. The absence of a history of ocular trauma and/or surgery indicates VKH disease. 5 Uveal effusion syndrome is common in nanophthalmic and hypermetropic eyes with thickened sclera, and because it is not normally associated with intraocular inflammation, the response to immunosuppressive therapy is poor. 7 Based on all our observations, the patients were diagnosed with SO.
Subfoveal choroidal thickness has been reported to decrease by 20 μm every 10 years in healthy Japanese subjects. 8 Furthermore, the same authors proposed the following equations to calculate choroidal thickness in healthy individuals: subfoveal choroidal thickness = −1.7 × age + 351.0 in males and −2.4 × age + 367.9 in females. 8 According to this equation, the expected choroidal thickness was calculated to be 163.9 μm for the 85-year-old patient in the present case 1, and 198 μm for the 90-year-old patient in case 2. Therefore, the choroidal thickness in the two present cases was greatly increased at the initial visit. Optic disc oedema and choroidal detachment are sometimes observed in elderly patients with VKH disease; however, these symptoms are atypical. 9 In this regard, SO appears the same as VKH disease.
Searches of the PubMed database (keyword, ‘SO’; search years, 2000–2022) and CiNii Research database (keywords, ‘VKH’ and ‘SO’; search years, 2000–2022) revealed that, to the best of our knowledge, only five reports on SO after cataract surgery have been published previously.4,10–13 One case occurred after non-complicated cataract surgery in a 74-year-old female patient, 4 while another case occurred after complicated cataract surgery that included vitrectomy with intraocular lens removal in a 50-year-old male. 10 Another case, involving a 74-year-old female, occurred after intracapsular cataract extraction with anterior chamber intraocular lens implantation. 11 In the case of a 4-year-old male patient who was diagnosed with SO after congenital cataract surgery, 12 the eye that was implanted with an intraocular lens ended up being blind. 12 A further published report described a case of SO after an extracapsular cataract extraction in a 59-year-old male patient, showing sunset-glow-fundi in spite of systemic steroid administration. 13
The present two cases represent the oldest patients with SO according to previously reported cases, while the youngest patients were 3-year-old children.11,12 After searching the PubMed and CiNii Research databases for cases of VKH disease (keyword, ‘VKH’; search years, 2000–2022), to the best of our knowledge, the oldest reported cases of VKH disease were aged 83 years,14,15 while the youngest reported cases were aged 3 years.16–18
Because elderly individuals tend to have systemic diseases, consideration should be paid to side-effects associated with high-dose systemic steroids. There are two reports about the side effects of steroid pulse therapy in elderly patients with VKH.14,15 Cervical fracture was reported to have occurred in an 83-year-old female patient after steroid pulse therapy, 14 while onset of diabetes was reported in an 83-year-old female patient during steroid pulse therapy. 15 Because steroid-associated diabetes was noted in the present case 1, the importance of managing eye and also systemic conditions in elderly patients was highlighted.
The present study describes the oldest reported patients with SO, according to previously published cases retrieved from the PubMed and CiNii Research databases. The two cases of elderly patients with SO were successfully treated by administrating steroid pulse therapy.
Since cataract surgery is increasingly performed, and as Japan is experiencing a population with super-longevity, elderly patients with SO may be encountered more frequently in Japan. Attention should be paid to possible side-effects of systemic steroid therapy in vulnerable elderly patients with SO.
Footnotes
Author contributions
Conceptualization, TM; writing–original draft presentation, SM; writing–review and editing, SI; review. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.