
Abstract
Objective
Neodymium:yttrium aluminum garnet laser capsulotomy is the gold standard treatment for posterior capsule opacification. Herein, we described a novel technique that has the potential to enhance the efficacy and safety of this procedure.
Methods
The technique utilizes multiple continuous ascending linear pattern laser shots, beginning at the bottom and forming successive horizontal rows upward. This approach results in a circular capsulotomy with minimal residual cloudiness along the edge of the intraocular lens optic.
Results
A total of 26 eyes from 23 patients with posterior capsule opacification were treated. The mean age of the participants was 73 ± 9.8 years. The average total energy used was 118.3 mJ. The average pretreatment best-corrected visual acuity was 0.45 ± 0.47 logMAR scale, which improved to 0.40 ± 0.53 following treatment. In 84% of cases, the optical axis was clear at the end of the intervention. Three patients reported subjective floaters, and two eyes required revision procedures. We did not observe any complications after the treatment.
Conclusions
The continuous ascending linear pattern posterior capsulotomy technique offers several potential advantages, including increased efficiency with lower energy usage, a larger optical opening, fewer capsule remnants, and reduced subjective complaints. Further studies involving a larger number of cases are required to evaluate this technique thoroughly.
Keywords
Introduction
Posterior capsule opacification (PCO) is the most common delayed complication following cataract surgery. 1 Over time, the lens capsule, which holds the intraocular lens (IOL) in place, may become cloudy due to the proliferation and migration of residual lens epithelial cells. This process leads to a decrease in visual acuity and contrast sensitivity, which patients often perceive as a recurrence of their original cataract symptoms. This condition is commonly referred to as a “secondary cataract.”2,3 The incidence of PCO 5 years after cataract surgery has been estimated to range between 28.5% and 50%.4,5
Neodymium:yttrium aluminum garnet (Nd:YAG) laser posterior capsulotomy (NYPC) remains the gold standard treatment for PCO. 5 This procedure involves the application of a Nd:YAG laser, following the placement of a contact lens on anesthetized cornea, to create an opening in the opacified posterior capsule, thereby allowing transmission of unobstructed light and restoration of clear vision. This minimally invasive procedure is typically performed in an outpatient setting and is associated with rapid visual recovery.5,6 Several posterior capsulotomy techniques have been described, including the crucial pattern, circular pattern, Christmas tree pattern, and hexagonal capsulotomy technique. 7 The general guideline for all techniques is to create an opening with a diameter of 4–5 mm in the posterior lens capsule using the least energy and the fewest number of laser shots. Despite the effectiveness of NYPC, some patients continue to experience subjective complaints such as floaters, glare, or mild visual disturbances. These symptoms may be influenced by several factors, including the technique used during the procedure and laser-specific settings. 7 The size of the Nd:YAG laser capsulotomy can significantly influence visual function. 8 Smaller capsulotomy openings have been associated with increased intraocular light scattering, which can degrade image quality and contrast sensitivity. 9 These findings suggest that achieving an optimal capsulotomy size and shape is important not only for clearing the visual axis but also for minimizing optical side effects.8–10 However, further studies are required to determine the ideal capsulotomy dimensions that balance efficacy with visual quality.
This study aimed to evaluate the anatomical and functional outcomes of a modified Nd:YAG (mNd:YAG) posterior capsulotomy technique for the treatment of fibrous and pearl forms of PCO, with particular emphasis on its efficacy and safety. The proposed method was designed to achieve wider removal of the posterior lens capsule with subtotal cleaning of the IOL optic, improving the visual acuity and minimizing the risk of residual capsule remnants, which may contribute to postoperative optical side effects and the occurrence of floaters. By optimizing the capsulotomy pattern, this approach aimed to enhance the visual quality and overall patient experience following treatment.
Methods
Study design
This study outlines the fundamental principles and clinical application of the mNd:YAG laser posterior capsulotomy technique, which utilizes multiple continuous ascending linear pattern (CALP) laser shots. The study design incorporates theoretical considerations and practical aspects of clinical implementation.
In this retrospective, nonrandomized, large case series study, medical records of patients with PCO who underwent NYPC from January 2022 to December 2023 were evaluated. The indication for treatment was visually significant PCO, defined as a reduction in visual acuity by one or more lines on Snellen optotypes. The study included patients with PCO following uncomplicated cataract surgery who were treated with mNd:YAG laser posterior capsulotomy using the CALP technique and had a recorded follow-up of a minimum of 3 months and up to 1 year. The exclusion criteria were as follows: (a) patients with any degree of corneal haze due to corneal dystrophies, corneal degenerations, or corneal scars after ocular trauma; (b) those with glaucoma, uveitis, and any retinal pathology; and (c) patients with incomplete follow-up.
The study was conducted at the Department of Ophthalmology, Justus Liebig University, University Hospital Giessen and Marburg GmbH, Campus Giessen, Germany. The study was conducted in accordance with the guidelines of the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Medical Faculty of Justus Liebig University of Giessen, Germany (Protocol Number: N2025/01). All patients provided their written informed consent. Prior to surgery, all patients underwent a complete ophthalmological examination, including best-corrected visual acuity (BCVA), intraocular pressure (IOP) measurement, slit-lamp anterior segment examination, and dilated funduscopic examination. In all cases, IOP was measured using a Goldmann applanation tonometer (Haag-Streit; Bern, Switzerland). For pretreatment and posttreatment comparison, BCVA and IOP were measured at 1 week, 1 month, and 3 months after the procedure. In order to exclude possible complications, patients were followed up for a minimum of 3 months and up to 1 year. The primary outcomes were improvement in BCVA and procedural safety. Secondary outcomes included changes in IOP after treatment, IOL damage during the treatment, and possible posttreatment complications, such as floaters, retinal tears, retinal detachment, uveitis, and macular edema.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 11
Procedure description
All patients were screened for ocular surface pathology before undergoing treatment. Pupil dilatation, allowing the visualization of the optic margin of the IOL, was achieved by instilling topical 1% tropicamide approximately 30 min prior to the procedure. Immediately before the procedure, two to three drops of 0.5% proparacaine hydrochloride were instilled into the conjunctival sac. A capsulotomy contact lens (Ocular Abraham Capsulotomy Lens, Ocular Instruments; WA, USA) was used in all the cases, with 2% hypromellose gel applied to the contact lens as coupling medium. All patients were treated using the VISULAS YAG III laser system (Carl Zeiss Meditech; Oberkochen, Germany) with energy settings for mNd:YAG ranging between 0.9 and 3.0 millijoules (mJ). The mNd:YAG technique uses CALP laser shots (Figure 1). Laser shots were delivered when the four aiming beams converged into a single point at the plane of opacified posterior capsule, using a positive offset (+150 µm) to shift the laser’s photodisruption point posteriorly. After the procedure, patients were prescribed topical prednisolone therapy three times daily for 1 week. No prophylactic IOP-lowering drops were administered immediately after the procedure.

Schematic depiction of the modified NYPC with CALP. (a) Visualization of the IOL optic margin is crucial; black line shows a continuous ascending linear shot pattern. (b) Initiation of the ascending NYPC and (c, d) accomplishing of the procedure. CALP: continuous ascending linear pattern; IOL: intraocular lens; NYPC: neodymium:yttrium aluminum garnet laser posterior capsulotomy.
The zone of treatment includes a subtotal area of the IOL optic, sparing approximately 0.5–1 mm on each side, depending on the type of IOL (Figure 2).

Images of PCO during different stages of continuous ascending linear shot pattern NYPC. (a) The eye with PCO before NYPC; (b) initial stage of the procedure using the described technique from inferior (1/3 done); (c) progression of the procedure with remaining less than one-third superior of PCO and (d) end of procedure, with no pits, and no opacities left behind the IOL optic. IOL: intraocular lens; NYPC: neodymium:yttrium aluminum garnet laser posterior capsulotomy; PCO: posterior capsule opacification.
The shots at the posterior capsule begin at the bottom edge of the IOL optic and create ascending horizontal rows (Figure 1(a)). The laser spots are placed adjacent to one another, forming a row at the bottom (Figure 1(b)). The second row begins immediately upon the last laser spot and continues horizontally until the other side of the IOL optic (Figure 1(c)). Several rows will be needed to treat a PCO completely without letting any capsular rest behind the IOL optic (Figure 1(d)).
Statistical analysis
This study primarily utilized descriptive statistical methods. Mean values and SDs were calculated for key variables, including patient age, laser energy used, visual acuity before and after the procedure, and IOP changes. Group means were compared using paired t-tests, and 95% confidence intervals were calculated for each mean. To reduce the risk of type I errors, statistical significance was defined as p <0.05. The decimal values of BCVA were converted to logMAR for statistical analysis. Categorical data, including the presence of subjective floaters and the clarity of the optical axis, were reported in percentages. Future studies with control groups and larger sample sizes should include inferential analyses to determine statistical significance and effect sizes. The statistical software used is IBM Statistical Package for Social Sciences (SPSS) statistics, version 31.0.1.0.
Results
A total of 23 patients (26 eyes) were included in this study, with a mean age of 73 ± 9.8 years; 10 were female and 13 were male. In 20 cases, NYPC with CALP was performed unilaterally, and in 3 cases, it was performed bilaterally. The mean follow-up period after treatment was 6 months. Of the total number of treated eyes, 15 were right eyes and 11 were left eyes.
The energy levels of the laser shots ranged from 1.2 to 2.8 mJ. On average, the total energy used per procedure was 118.3 mJ (range: 48.6–394.8 mJ). The number of laser shots ranged from 26 to 141, with an average number of 60.9 shots (Figure 3).

Energy levels used during intervention. (a) Number of spots and energy used per patient and (b) total energy used per patient.
The mean BCVA before the procedure was 0.45 ± 0.47 logMAR for the entire study population. After capsulotomy, the mean BCVA improved to 0.40 ± 0.53 logMAR (Figure 4). A paired t-test revealed a statistically significant improvement in visual acuity following yttrium aluminum garnet (YAG) capsulotomy (t = −2.91, p = 0.0075). This finding indicates that the observed improvement in visual acuity is likely attributable to the intervention rather than random variation.
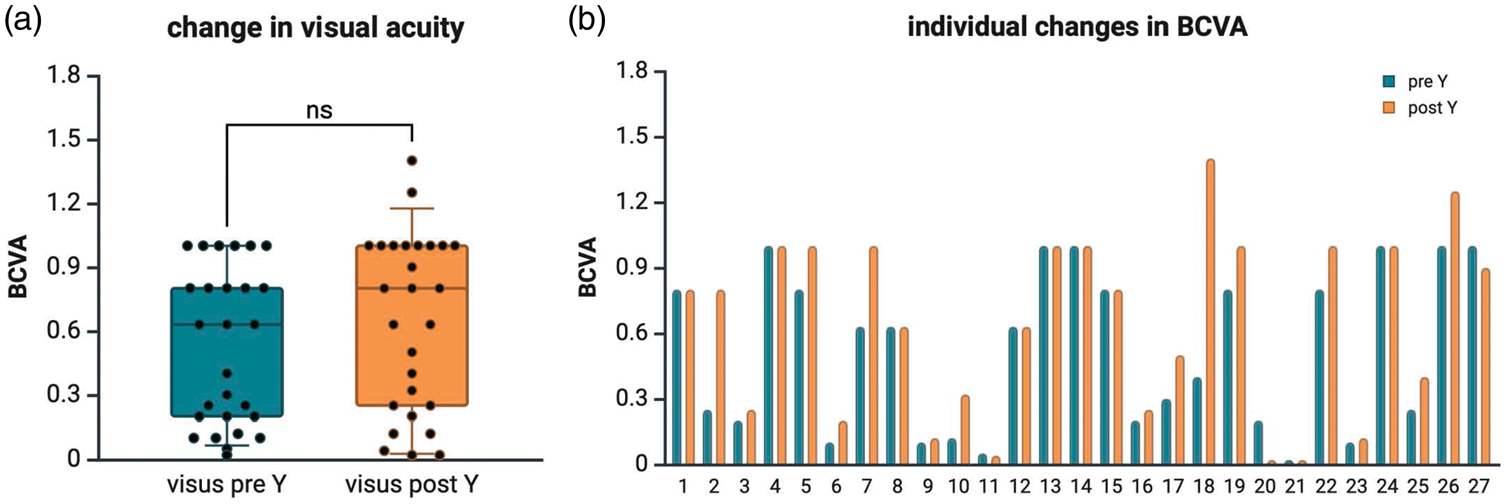
BCVA changes before and after the treatment. (a) Change in visual acuity for all patients during the intervention, p = 0.21 (Mann–Whitney U test) and (b) changes in visual acuity at the individual level. BCVA: best-corrected visual acuity.
The average pretreatment IOP value was 14.29 mmHg (range: 10–21). Postprocedure, IOP increased by an average of 0.86 mmHg (range: 9–33). Only one patient experienced an IOP spike to 33 mmHg, which was successfully treated solely with antihypertensive eyedrops (carbonic anhydrase inhibitors, twice daily for 2 weeks) (Table 1).
Comparison of BCVA and IOP before and after treatment.

BCVA: best-corrected visual acuity; IOP: intraocular pressure; mNd:YAG: modified neodymium:yttrium aluminum garnet posterior capsulotomy; min: minimum; max: maximum.
By the end of the intervention, the IOL optic and the optical axis were clear in 84% of cases, and patients reported satisfaction with the results of the treatment. However, three patients reported subjective visual disturbances, such as floaters, and two eyes required revision procedures. No significant complications, such as corneal, iris, or IOL damage; corneal edema; iris hemorrhage; IOL subluxation; cystoid macular edema; retinal tears; or retinal detachment, were noted.
Discussion
Nd:YAG laser capsulotomy remains the standard treatment for PCO following cataract surgery. However, the procedure has been associated with an increased risk of complications, including IOP elevation, retinal detachment, and potential IOL damage. 7 Importantly, recent studies have demonstrated that the shape and size of the capsulotomy significantly influence visual function, with smaller openings associated with increased intraocular light scattering and reduced image quality and contrast sensitivity.8–10 These findings underscore the importance of optimizing not only the procedural safety but also the optical outcomes. Consequently, novel approaches are needed to improve the precision and predictability of capsulotomy size and placement, aiming to enhance safety and visual performance.
The results of our study indicate that the mNd:YAG laser capsulotomy technique using CALP represents a promising alternative to traditional methods for treating PCO after standard cataract surgery. By employing multiple continuous linear laser shots that ascend in horizontal rows, we achieved a uniform removal of the opacified posterior capsule within the entire area of the IOL optic. This technique resulted in improved visual acuity for most patients and a reduction in subjective complaints, such as floaters. As the primary aim of the study was to describe the outcomes associated with the new technique, no additional inferential statistical tests (e.g. t-tests or analysis of variance) were performed.
The optimal size of the posterior capsulotomy remains a matter of debate. Guidelines for determining the diameter of the capsulotomy were established approximately half a century ago, based on optical and mechanical factors. Regarding mechanical factors, the posterior lens capsule is considered a barrier that should be maintained between the anterior and posterior segments of the eye. 9 In order to minimize glare and other undesirable optical aberrations following posterior capsulotomy, it was suggested that the diameter should be equal to the normal pupillary diameter in dark conditions. 9 From an optical point of view, we believe that the optical factors are in favor of a larger capsulotomy size. All surgeons who perform cataract surgery aim to maintain transparency of the posterior lens capsule. Therefore, leaving a large portion of the opacified lens capsule intact appears illogical. Moreover, in a study of 17,688 eyes after cataract surgery, Elbaz et al. 12 found no evidence that Nd:YAG capsulotomy increased the risk of pseudophakic retinal detachment over a 4-year follow-up period.
A technique with a larger diameter of Nd:YAG laser capsulotomy was described by Min et al. 13 Their technique consists of a circular en bloc pattern of laser shots placed 0.5 mm inside the optic margin or along the anterior continuous curvilinear capsulorhexis. Upon completion of the procedure, the circular fragment of the posterior capsule was completely separated from lens capsule and displaced into the intravitreal space. The total energy used for this procedure was between 40 and 167 mJ, with a mean total energy level of 74 ± 21 mJ. 13 Although Min et al. did not report the number of laser shots, Kim et al., 14 using the same technique, reported a mean total energy of 195.88 ± 120.06 mJ and a mean number of 97.5 ± 55.2 mJ laser shots. In our case, on average, a lower energy of 118.3 mJ (range: 48.6–394.8 mJ) and a lower mean number of shots (average number of shots: 60.9) were required. Moreover, with our mNd:YAG technique, the posterior lens capsule was completely removed, whereas in the alternative technique, a fragment of the posterior lens capsule is displaced into the vitreous body, potentially increasing the possibility of floaters. With an average energy usage of 118.3 mJ, we were able to perform an effective capsulotomy without increasing the risk of complications.
The reduced energy settings aimed to produce smaller laser spots, resulting in a more precise capsulotomy and a circular opening with minimal cloudiness at the edge of the optic. Although this method requires a greater number of laser shots than conventional circular YAG capsulotomy, the total energy used remains within standard safety limits.
Our findings are consistent with those of previous studies emphasizing the benefits of optimized laser parameters and novel techniques in YAG capsulotomy. Previous studies have demonstrated that minimizing laser energy can significantly reduce the risk of postoperative complications, including macular edema and retinal detachment. In contrast to the findings of Elbaz et al., 12 a recent study reported that the incidence of retinal detachment following Nd:YAG laser capsulotomy was 0.82% (2/244), with a mean time of 13.5 months between capsulotomy and retinal detachment. 15 In our cohort, there were no cases of retinal detachment after the surgery during the 1-year follow-up period.
Earlier techniques often relied on spot shots or radially oriented ablation, which, in some cases, resulted in irregular openings and an increased likelihood of capsule remnants. The cross-like and circular Nd:YAG laser capsulotomy techniques have been shown to induce similar visual changes. The circular technique is associated with higher energy consumption, increased floater symptoms, and a pronounced effect on macular thickness 1 day after laser capsulotomy, as reported in a previous study. 16 The clinical significance of this study lies in the potential to improve the efficacy and safety of Nd:YAG laser posterior capsulotomy. Reducing the required laser energy and achieving a uniform capsule removal could lower the risk of postoperative floaters and increase patient satisfaction. This technique may be particularly beneficial for patients at higher risk of retinal complications, as it allows improved visualization of the fundus and the peripheral retina.
Findl et al. 17 demonstrated that a larger capsulotomy size may cause a hyperopic shift due to increased posterior movement of the IOL. However, Chua et al. 18 found that there was no significant difference in the refraction following Nd:YAG laser capsulotomy. Yilmaz et al. 19 also found that the size of posterior capsulotomy does not significantly affect either refraction or visual acuity. Reports in the literature regarding IOP change after Nd:YAG laser capsulotomy are controversial. Karahan et al. 20 reported IOP elevation in patients with capsulotomy sizes smaller than 3.4 mm as well as in those with larger capsulotomy sizes, although the average value of total energy used was statistically insignificant. Elevation of IOP after Nd:YAG laser capsulotomy in 1% of cases was reported by Stark et al. 21 In contrast, studies of Ge et al. 22 and Lin et al. 23 reported a higher risk of IOP elevation in patients with glaucoma. In our cohort of 26 eyes from 23 patients treated with the new approach, only one patient experienced a significant elevation in IOP after the procedure. Our findings suggest that the new technique has a minimal impact on IOP, which is a critical safety consideration. No complications were observed in any of the reviewed cases. Specifically, we found no instances of damage to the cornea, iris, or IOL pitting; no signs of corneal edema or iris hemorrhage; and no evidence of IOL subluxation. Similarly, no patient developed cystoid macular edema, and no retinal breaks or retinal detachments were observed throughout the 1-year follow-up period. Subjective visual disturbances, such as floaters, were reported by three patients, and revision procedures were required in two eyes. Only one patient experienced IOP elevation, which was managed with topical medications (carbonic anhydrase inhibitors, twice daily for 2 weeks).
To the best of our knowledge, this is the first study to demonstrate the effectiveness of this novel approach for mNd:YAG laser posterior capsulotomy. However, this study has several limitations. The main limitation of this study is its retrospective and noncomparative design. Another limitation is a relatively small sample size; the limited number of evaluated parameters, such as contrast sensitivity and pupillometry measurement; and the average follow-up of 6 months. Furthermore, correlations between the technique itself and different IOL types (one-piece, three-piece, hydrophobic vs. hydrophilic acrylic IOL, toric IOLs, among others) were not assessed.24,25 Nevertheless, the main aim of this study was to present the mNd:YAG laser posterior capsulotomy with CALP and to analyze its preliminary safety and efficacy. The technique does not present a challenge to learn and adapt for professionals with experience in NYPC procedures. We believe that the technique can be readily absorbed by beginners as well. Further studies involving a larger patient cohort are necessary to confirm the efficacy and safety of this approach. In addition, the potential impact on ocular biometric measurements warrants further evaluation. Comparative analyses with other established techniques would help clarify the relative benefits and limitations of this method. Investigating patient satisfaction and subjective visual symptoms following capsulotomy can provide valuable insights to support and refine clinical practice.
Conclusion
The mNd:YAG laser posterior capsulotomy with CALP offers several potential advantages. These advantages include higher efficiency due to the use of lower energy settings, resulting in a larger optical opening of the posterior capsule and fewer residual capsule remnants. This approach may also reduce the likelihood of subjective complaints after the procedure.
This technique can serve as an alternative method for performing Nd:YAG laser posterior capsulotomy, particularly in patients at higher risk of posterior segment complications or those with persistent subjective complaints following the standard procedure. Further research with larger sample sizes and longer follow-up periods is needed to confirm these results and refine the technique further.
Footnotes
Acknowledgments
The authors have nothing to report.
Author contributions
L.L. and M.A.O. designed and carried out the research. L.L. and M.A.O. collected and organized the data. L.L., M.A.O., X.L., and T.S.B. analyzed and performed the statistics. M.A.O., X.L., and T.S.B. drafted the paper. K.S. and S.S. performed critical revision of the manuscript.
Consent for publication
Not applicable.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors indicate no financial support or conflicts of interest. All authors attest that they meet the current ICMJE criteria for authorship.
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Medical Faculty of Justus Liebig University of Giessen, Germany (Protocol number: N2025/01). All patients involved provided their written informed consent.
Funding
No funding was received for conducting this study.
Informed consent
We have obtained informed written consent from the patient.