
Abstract
Objective
This study was conducted to evaluate the predictive value of endoscopic measurements of cardia opening diameter and sliding hernia length for diagnosing gastroesophageal reflux disease.
Methods
A total of 233 patients with typical gastroesophageal reflux disease symptoms who underwent endoscopy and esophageal pH-impedance monitoring between September 2017 and September 2023 were enrolled in this study. Cardia opening diameter and sliding hernia length were measured during endoscopy under adequate gastric insufflation. Using esophageal pH-impedance monitoring as the gold standard (with acid exposure time >4% as the diagnostic criterion for gastroesophageal reflux disease), the correlation between cardia opening diameter/sliding hernia length and gastroesophageal reflux disease-related parameters was analyzed. A nomogram prediction model was subsequently developed.
Results
The optimal cutoff values for predicting pathological acid reflux were cardia opening diameter >2 cm and sliding hernia length >1 cm (area under the receiver operating characteristic curve = 0.648 for both). Compared with patients with a cardia opening diameter ≤2 cm, those with a cardia opening diameter >2 cm had significantly higher acid exposure time (6.8% vs. 2.5%), DeMeester score (25.7 vs. 10.9), and number of reflux episodes (108 vs. 59) (all p < 0.001). Similarly, sliding hernia length >1 cm was associated with more severe reflux parameters (p < 0.05) and was more prevalent in males (72.4% vs. 43.6%). Univariate and multivariate logistic regression analyses demonstrated that a nomogram incorporating age, body mass index, and sliding hernia length exhibited good predictive performance (area under the curve = 0.739).
Conclusion
Endoscopically assessed cardia opening diameter and sliding hernia length are useful functional predictors of gastroesophageal reflux disease. The integrated prediction model may serve as a valuable diagnostic aid, especially in primary care or resource-limited settings.
Keywords
Introduction
Gastroesophageal reflux disease (GERD), a common chronic disorder of the digestive system, is characterized by the reflux of gastric and/or duodenal contents into the esophagus or oral cavity, resulting in discomforting symptoms and/or complications. The global prevalence of GERD varies widely, ranging from 2.5% to 51.2%, and affects approximately 20% of adults in high-income countries.1,2 In recent years, the incidence of GERD has been rising in China as well. 3 The pathophysiology of GERD is multifactorial, involving anatomical factors such as hiatal hernia (HH) as well as functional abnormalities, including incompetent lower esophageal sphincter (LES), impaired esophageal peristalsis, and defective esophageal clearance mechanisms.
Although esophageal manometry and pH-impedance monitoring remain the gold standards for GERD diagnosis, their use is often limited by their high cost, procedural complexity, low patient acceptance, and the need for specialized interpretation. In contrast, upper endoscopy is a fundamental tool in GERD evaluation. This procedure can detect varying degrees of reflux esophagitis (RE) and identify anatomical changes at the gastroesophageal junction (GEJ), such as sphincter laxity or HH, thereby providing valuable information for diagnosis and prognosis. However, conventional retroflexed endoscopic observation has inherent limitations, as it is susceptible to artifacts caused by factors such as gastric insufflation level, respiratory movement, retching, and belching. This underscores the clinical need for a more standardized and functional endoscopic approach to assess GEJ.
In recent years, increasing attention has been directed toward novel functional endoscopic techniques that facilitate GERD diagnosis during endoscopy and support treatment decisions.4–6 In 2019, Japanese scholars 4 proposed an endoscopic method involving measurement of the cardia opening diameter (CO) and sliding hernia length (SH) to functionally evaluate GEJ, demonstrating its potential predictive value for GERD. Based on these findings, we conducted a preliminary study using data from our own institution to further explore the clinical utility of this method.
Materials and methods
Study population
This single-center, diagnostic observational study was conducted at Peking University International Hospital, Beijing, China, between September 2017 and September 2023. The study protocol was approved by the hospital’s Institutional Review Board (Approval Number: 2021-KY-0027-03) and was conducted in accordance with the ethical principles of the Declaration of Helsinki 1975, as revised in 2024. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 7 To protect patient privacy, all data were deidentified prior to analysis.
The study enrolled patients presenting with typical symptoms of GERD, including heartburn, acid reflux, chest pain, or belching, who underwent upper gastrointestinal endoscopy, esophageal high-resolution manometry (HRM), and esophageal multichannel intraluminal impedance-pH monitoring (pH-impedance monitoring, Given Imaging Inc.; Duluth, USA). A diagnosis of GERD was confirmed based on pH-impedance monitoring. Patients with a history of anti-reflux surgery (e.g. prior laparoscopic Nissen fundoplication, Toupet fundoplication, or anti-reflux mucosectomy (ARMS)), Barrett’s esophagus (BE), or major esophageal motility disorders (achalasia, absent contractility, and esophagogastric junction outflow obstruction as defined by the Chicago Classification v4.0) were excluded. All participants were instructed to discontinue proton pump inhibitors (PPIs) at least 4 weeks prior to endoscopic examination to allow accurate detection of erosive esophagitis. Similarly, PPIs were discontinued for at least 1 week prior to HRM and the pH-impedance study to ensure reliable measurement of acid exposure. Written informed consent was obtained from all prospective study participants prior to study enrollment.
Endoscopic assessment of GEJ
Endoscopic examinations were conducted using high-definition endoscopes, EG-590 and EG-600 (Fuji Photo Film Corp.; Tokyo, Japan), with outer diameters measuring 10.8 mm and 9.9 mm, respectively. All procedures were conducted under intravenous sedation with propofol and were performed by experienced endoscopists at Peking University International Hospital.
A functional endoscopic technique was employed to evaluate GEJ. This method involved retroflexed observation under maximal high-flow insufflation until the gastric folds on the greater curvature were flattened, and the GEJ fully opened. Parameters assessed using a previously described method
4
included the following:
CO. CO was defined as the maximal diameter of the cardia opening, measured in centimeters. SH. SH was defined as the vertical distance from the diaphragmatic crus to the squamocolumnar junction (SCJ), also measured in centimeters. The outer diameter of the endoscope (approximately 1 cm) was used as a reference for estimation.
Still images from the endoscopic videos were independently reviewed by three endoscopists to assess CO and SH. Any discrepancies in measurements were resolved by consensus to ensure consistency. Subsequently, the endoscopic CO and SH measurements were compared with the GERD parameters obtained from pH-impedance monitoring.
The primary outcome was acid exposure time (AET), defined as the percentage of the total monitoring time during which the esophageal pH remained below 4. Secondary outcomes included the DeMeester composite score, total number of reflux episodes (categorized liquid, gas, or mixed; acid or nonacid), and number of proximal reflux episodes. The pH-impedance probe was placed transnasally, guided by findings from the previous HRM study, to precisely position the probe 5 cm above the upper border of the LES. According to the 2024 Lyon Consensus, 8 an AET of >6% and total number of reflux episodes >80 were considered definitively abnormal. Additionally, the Chinese GERD guidelines 9 recommend an AET >4% as sufficient for diagnosing GERD in the Chinese population. Accordingly, this threshold was adopted as the diagnostic criterion in our study.
Statistical analysis
Data analysis was conducted using the Statistical Software for Social Sciences (SPSS) software (version 26.0, IBM Corp.; Armonk, USA). Continuous variables were represented as mean ± SD or median, as appropriate, whereas categorical variables were presented as frequencies and percentages. Intergroup comparisons for continuous variables were performed using unpaired t-tests, and categorical data were compared using the chi-square or Fisher’s exact test, as appropriate. Correlations between continuous and categorical variables were evaluated using the Spearman correlation coefficient. Receiver operating characteristic (ROC) curves were generated to determine the optimal cutoff values for CO and SH, with the Youden index used to identify thresholds that maximized sensitivity and specificity.
Factors associated with increased AET were analyzed using univariate and multivariate binary logistic regression. Significant variables identified in the multivariate analysis were subsequently incorporated into a nomogram prediction model using R software (version 4.3.0, R Foundation for Statistical Computing, Vienna, Austria). The model was internally validated within the training cohort. The predictive value and optimal cutoff points for GERD were evaluated using ROC curves, calibration plots, and decision curve analysis (DCA).
All analyses were two-tailed, and p-values <0.05 were considered statistically significant.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Peking University International Hospital (IRB Registration Number: 2021-KY-0027-03). Written informed consent was obtained from all participants before they underwent upper gastrointestinal endoscopy. In accordance with the IRB policy, individual written informed consent for participation in this study was not required. The study protocol was publicly disclosed on the hospital’s official website, and participants were given the opportunity to opt out of allowing the use of their medical data. Written informed consent was obtained from all participants for prospective data collection. For retrospective analysis of anonymized data, the IRB granted a waiver of additional consent.
Results
A total of 248 patients were initially enrolled in the study. However, 13 patients were excluded from the study due to the following conditions: Nissen fundoplication (n = 5), BE (n = 5), and esophageal motility disorders (n = 3). Ultimately, 233 patients were included in the final analysis. The mean age (± SD) was 49.4 ± 12.6 years, and 110 participants were male (47.2%). Detailed characteristics of the study population are summarized in Table 1. No adverse events were observed during the procedures.
Patient characteristics (n = 233).

BMI: body mass index; IQR: interquartile range; GERD: gastroesophageal reflux disease.
CO
CO was significantly and positively correlated with multiple GERD-related parameters, including AET (r = 0.282, p < 0.001), DeMeester score (r = 0.286, p < 0.001), reflux frequency (r = 0.255, p < 0.001), and endoscopic evidence of RE (r = 0.286, p < 0.001). ROC curve analysis determined an optimal CO cutoff of 2 cm for predicting pathological acid exposure (AET > 4%), with a sensitivity of 73.3%, specificity of 52.0%, and an area under the ROC curve (AUROC) of 0.648.
When patients were stratified based on the 2-cm CO threshold, those with a CO >2 cm exhibited significantly worse GERD profiles compared to those with a CO ≤2 cm. Specifically, the CO >2 cm group had higher AET (6.8% vs. 2.5%, p < 0.001), elevated DeMeester scores (25.7 vs. 10.9, p < 0.001), and more frequent reflux episodes (108 vs. 59, p < 0.001), as summarized in Table 2. Demographic analysis further showed that the CO >2 cm group had a significantly higher proportion of males (66.7% vs. 43.3%, p = 0.009) and higher body mass index (BMI; 25.15 vs. 23.20 kg/m2, p = 0.003). No significant difference in age was observed between the two groups (p = 0.710), suggesting that CO dilation is more closely associated with sex and body weight than with age. Collectively, these findings indicated that a CO >2 cm serves as a clinically relevant marker of more severe GERD phenotypes, particularly among male patients with elevated BMI.
Statistical analysis stratified according to CO threshold.
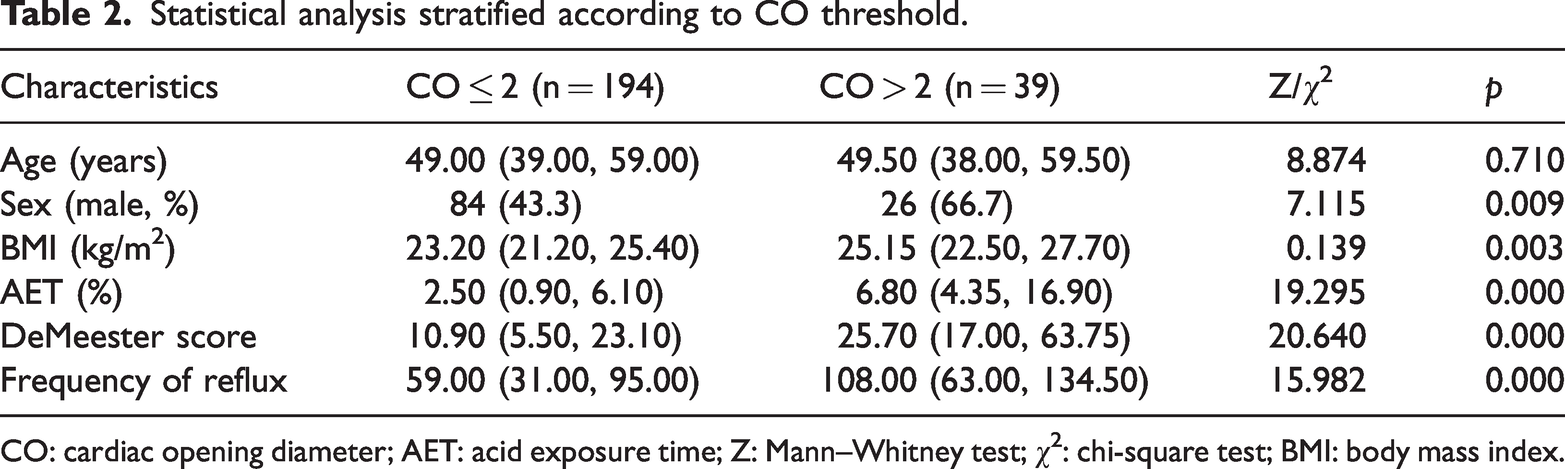
CO: cardiac opening diameter; AET: acid exposure time; Z: Mann–Whitney test; χ2: chi-square test; BMI: body mass index.
SH
SH measurements revealed that 29 patients (12.4%) demonstrated SH >1 cm, whereas the majority (204 patients, 87.6%) exhibited SH ≤1 cm. Notably, 7 patients (4.7%) with SH ≤1 cm also exhibited CO >2 cm.
Statistical analysis demonstrated significant positive correlations between SH and key GERD parameters, including AET (r = 0.270, p < 0.001), DeMeester score (r = 0.283, p < 0.001), reflux episode frequency (r = 0.234, p < 0.001), and endoscopic evidence of RE (r = 0.264, p < 0.001). ROC curve analysis identified an optimal SH cutoff of 1 cm for predicting pathological acid exposure (AET > 4%), with a sensitivity of 77.1%, specificity of 51.0%, and an AUROC of 0.648. When patients were stratified based on the 1-cm threshold, those with SH >1 cm demonstrated significantly worse reflux profiles compared to those with SH ≤1 cm. Specifically, the SH >1 cm group exhibited higher AET values (6.25% vs. 2.60%, p = 0.003), elevated DeMeester scores (24.35 vs. 11.50, p = 0.002), and more frequent reflux episodes (92.5 vs. 61, p = 0.010).
Demographic comparisons showed that patients with SH >1 cm were more likely to be male (72.4% vs. 43.6%, p = 0.005) and had a slightly higher median age (50 vs. 43 years, p = 0.018). No statistically significant difference in BMI was observed between the two groups (p = 0.356).These findings are detailed in Table 3, which compares all relevant clinical and demographic parameters between the SH ≤1 cm (n = 204) and SH >1 cm (n = 29) groups, including age, sex distribution, BMI, AET, DeMeester score, and reflux frequency along with corresponding statistical test results and p-values.
Statistical analysis stratified according to SH threshold.

SH: sliding hernia length; BMI: body mass index; AET, acid exposure time; Z: Mann–Whitney test; χ2: chi-square test
The distributions of CO and SH measurements among the study participants are illustrated in Figure 1. Most patients (87.6%) demonstrated SH ≤1 cm, whereas 12.4% (n = 29) exhibited SH >1 cm corresponding to the optimal threshold for predicting pathological acid exposure (AET > 4%).

Distribution map of CO and SH in the study participants. CO: cardia opening diameter; SH: sliding hernia length.
Predictive diagnostic model of GERD
Univariate logistic regression was performed for all variables listed in Table 4 to predict pathological acid exposure (AET > 4%). Variables with p ≤0.05, including age, BMI, and SH, were subsequently included in a multivariate logistic regression analysis.
Univariate and multivariate logistic regression analyses for patients with GERD.

GERD: gastroesophageal reflux disease; BMI: body mass index; CO: cardiac opening diameter; SH: sliding hernia length; HP: Helicobacter pylori; OR: odds ratio; CI: confidence interval.
A nomogram was subsequently constructed based on the independent predictors identified in the multivariate analysis, including BMI and SH. The resulting prediction model is illustrated in Figure 2, where the total score corresponds to the estimated probability of GERD based on the combined contributions of each risk factor.

Nomogram model for predicting gastroesophageal reflux disease. Assessment of the nomogram model for predicting gastroesophageal reflux disease. (a) Comparison of ROC curves for the nomogram; (b) four calibration curves for the nomogram in the primary cohort; and (c) decision curve analysis for the nomogram. ROC: receiver operating characteristic.
To evaluate the predictive performance of the nomogram, ROC curve analysis was conducted (Figure 2(a)), yielding an AUROC of 0.739, which indicated good discriminative ability. The calibration curve (Figure 2(b)) demonstrated strong concordance between the predicted and observed outcomes. Furthermore, the nomogram curve (Figure 2(c)) remained consistently above the reference lines and displayed a characteristic upward convex shape within the 0.2–0.8 probability range, further supporting the model’s high performance.
Collectively, these results indicated that the nomogram provides robust predictive accuracy for GERD. Its validity is supported by multiple metrics, including ROC curve, calibration (SHARP) plot, and DCA, all of which demonstrated close agreement between the predicted probabilities and actual clinical outcomes.
Discussion
GERD is a common motility-related disorder of the digestive tract, characterized by chronic symptoms and/or complications caused by the reflux of gastric and duodenal contents into the esophagus or oral cavity. Based on endoscopic findings, GERD can be classified into nonerosive reflux disease (NERD), RE, or BE. In recent years, the prevalence of GERD has been increasing, potentially attributable to factors such as heightened gastric acid secretion, decreasing Helicobacter pylori infection rates, and adoption of Westernized dietary and lifestyle habits.9–11
The diagnostic criteria for GERD remain a subject of debate between Eastern and Western medical communities. The gold standard for diagnosis is 24-h esophageal pH monitoring; however, significant ethnic variations exist in the diagnostic threshold for its primary parameter, AET. In China, an AET ≥4% is adopted as the diagnostic cutoff, 9 consistent with the Korean consensus. 11 In contrast, Japanese guidelines 10 do not specify a definitive threshold. This discrepancy aligns with the characteristics of Asian populations, which exhibit a higher prevalence of NERD and generally lower AET levels than those in Western populations. Studies have shown that in Chinese patients, an AET ≥4% is significantly associated with typical reflux symptoms, validating the appropriateness of this threshold for the Chinese population. In contrast, Western populations 8 more commonly present with RE and BE. Therefore, a higher threshold (e.g. AET ≥ 6%) used in Western settings enhances specificity, whereas the Chinese threshold (≥4%) improves sensitivity. These differences underscore the need for ethnicity- and population-specific diagnostic standards.
The findings demonstrate that an enlarged CO is a significant endoscopic marker associated with pathological reflux. Notably, dilatation of the diaphragmatic hiatus is the primary determinant of a widened CO, as highlighted in recent consensus literature. 12 This anatomical distortion compromises the integrity and function of the crural diaphragm (CD), a crucial extrinsic component of the anti-reflux barrier. As extensively discussed by Nguyen et al., 12 dilatation of hiatus results in separation of the CD from the LES, diminishing its sphincteric function and contributing to the overall incompetence of the anti-reflux barrier. Therefore, our endoscopic measurement of CO serves as a simple yet effective proxy for assessing this element of anatomical disruption at GEJ. This mechanistic link reinforces the clinical value of measuring CO during routine endoscopy.
This study used CO and SH measurements for performing endoscopic evaluation of LES to improve the diagnostic predictions for GERD. Consistent with previous research, we found that patients with CO >2 cm and/or SH >1 cm exhibited significantly higher AET and DeMeester scores. By adopting AET >4% as the diagnostic standard and analyzing a relatively large cohort (n = 233), we reaffirmed previous findings while proposing stricter CO and SH cutoffs that may accurately reflect local patient characteristics. In univariate analysis, both these readily obtainable endoscopic parameters were strongly associated with GERD, enhancing diagnostic sensitivity and facilitating early identification of high-risk GERD patients. For instance, a combination of CO >2 cm and SH >1 cm strongly suggests pathological reflux. Inoue et al. 4 were the first to propose that the CO–SH measurement method could predict GERD. Their retrospective analysis of 61 patients with GERD demonstrated a significant correlation between CO/SH and AET, proposing CO ≥3 cm (sensitivity, 72.4%; specificity, 46.9%) and SH ≥2 cm (sensitivity, 55.2%; specificity 75.0%) as optimal thresholds for AET >6%. Japanese researchers have further advanced the field of functional endoscopic diagnosis. Shimamura et al. 5 developed the Endoscopic Pressure Study Integrated System, which continuously measures intragastric pressure during gastric insufflation in endoscopy. This method demonstrates high diagnostic accuracy for pathological acid reflux, with pressure difference showing the strongest predictive value (AUC = 0.87).
In the present study, CO >2 cm emerged as a sensitive endoscopic indicator of GERD (sensitivity, 73.3%; specificity, 52.0%; AUROC, 0.648). Similarly, SH >1 cm also showed strong predictive value (AUROC =0.648), although its specificity was modest. When analyzed in combination, CO and SH demonstrated significant correlation with standard GERD severity indicators such as AET, DeMeester score, and reflux frequency. The strong univariate associations support the use of CO/SH measurements as practical, noninvasive screening tools that can be easily incorporated into routine upper endoscopy, particularly valuable in healthcare settings where pH monitoring is unavailable.
In addition, we observed strong associations between CO and demographic variables, including sex and BMI, with significantly higher CO values in male and overweight patients. In the SH >1 cm subgroup, 72.4% of patients were male, suggesting that male sex and elevated BMI are independent risk factors for esophagogastric junction dilation and GERD. These findings are consistent with international guidelines 11 and consensus13–16 that identify obesity as a well-established risk factor for GERD. Proposed mechanisms include increased intra-abdominal pressure, delayed gastric emptying, altered esophagogastric pressure gradients, reduced LES pressure, and increased frequency of transient LES relaxations, all of which compromise the anti-reflux barrier. 17 Consequently, weight loss remains a cornerstone of GERD management. Furthermore, the significantly higher prevalence of GERD among male patients corroborates findings from multiple studies.16,18–21 Interestingly, patients with SH >1 cm were significantly younger than those with SH ≤1 cm (43 vs. 50 years, p < 0.01), contradicting the conventional belief that GERD incidence increases with age,18,19,22,23 but aligning with studies suggesting age-independent GERD development. 24 Given GERD’s multifactorial pathogenesis, including lifestyle and psychosocial factors such as smoking, alcohol consumption, depression, and physical inactivity, 21 this age discrepancy may reflect sample limitations or selection bias. Future multicenter prospective studies are needed to elucidate the true relationship between age and SH.
Based on CO and SH data, we proposed a distribution chart that offers novel evidence for individualized GERD diagnosis and treatment. Endoscopic anti-reflux procedures, such as ARMS, anti-reflux mucosal ablation (ARMA), and anti-reflux mucoplasty with valve formation (ARM-P/V), are increasingly offered to patients who are responsive to medication but prefer nonpharmacologic options. These procedures are indicated for patients with confirmed GERD diagnosis who respond to acid-suppressive medication but are unwilling to receive long-term medication or experience drug-related adverse effects. 9 By simultaneously evaluating CO and SH, we can screen suitable candidates for endoscopic treatment. For instance, CO >2 cm independently correlates with acid reflux, and these patients may benefit more significantly from endoscopic interventions, which aligns with the perspectives of Japanese scholars. 4 Patients with SH >2 cm and confirmed HH are considered candidates for surgical treatment, 25 such as Nissen and Toupet fundoplication. However, consensus guidelines on HH 26 emphasize that surgical repair is unnecessary for sliding hernias in the absence of GERD. Based on our findings, we recommend further investigation of the synergistic effects of CO and SH. For example, patients presenting with CO >2 cm and SH >1 cm may provide meaningful guidance for endoscopic and surgical management of sliding HH. Although incorporating HRM data on the CD value would enhance reliability, our center’s limited HRM volume suggests that future studies should include esophageal motility parameters to further strengthen the evidence chain.
We also developed a novel nomogram-based predictive model for GERD, including independent predictors of age, BMI, and SH. Notably, although CO showed strong univariate correlations with pathological reflux parameters, it was not retained as a statistically independent predictor in the multivariate model (p = 0.078). This suggests that its predictive value is shared with or explained by other factors in the model, such as SH, with which it was correlated. Nonetheless, the straightforward visual assessment of CO during endoscopy remains a readily available and clinically useful marker for prompting further investigation for GERD. The model demonstrated moderate diagnostic accuracy (AUC = 0.739) and good calibration. DCA confirmed its clinical utility in the 0.2–0.8 threshold range. This visual, user-friendly tool can help clinicians assess GERD risk and guide early intervention in high-risk populations, particularly in settings with limited availability of advanced diagnostics.
This study has several limitations. First, its mixed retrospective and prospective design may have introduced selection and information biases. Second, the absence of a healthy control group limited the comparative analysis. Third, data collection from a single institution may have reduced the generalizability of our findings. Fourth, the relatively small sample size in certain subgroups may have increased the risk of overfitting in multivariate modeling, potentially affecting model stability. Future research should involve larger, multicenter cohorts; incorporate objective image analysis (e.g. artificial intelligence (AI)-based measurement) include esophageal motility data; and aim to improve AUC values to strengthen the model’s validity and utility. Fifth, the assessments of CO and SH were based on retrospective reviews of still images rather than real-time endoscopic evaluation, which may have introduced measurement variability and represents a limitation of our study design. Sixth, the study focused on the quantitative endoscopic metrics of CO and SH, which were initially proposed by Inoue et al. 4 Although our results validated the utility of these measurements in a larger cohort, we recognize the parallel development of the more comprehensive American Foregut Society (AFS) grading system.27,28 Unfortunately, due to the retrospective nature of part of our dataset, consistent and documented assessment of the gastroesophageal flap valve (GEFV)/Hill grade was unavailable for our cohort. This represents a limitation, as GEFV constitutes a key component of the anti-reflux barrier. Future prospective studies should aim to integrate all three components to provide a more holistic and standardized endoscopic evaluation of GEJ.
Conclusion
This study confirmed that CO (>2 cm) and SH (>1 cm) are sensitive endoscopic predictors of pathological acid reflux (AET > 4%), each receiving an AUROC of 0.648. Both parameters were significantly associated with GERD severity, including AET, DeMeester score, and reflux episode frequency. A nomogram prediction model, incorporating age, BMI, and SH demonstrated moderate predictive performance (AUC = 0.739) and good clinical applicability. The CO–SH measurement method is simple, cost-effective, and may be seamlessly integrated into routine endoscopy, offering a valuable diagnostic alternative for institutions lacking pH monitoring capabilities. Future multicenter studies are warranted to validate these findings and explore their utility in selecting candidates for endoscopic anti-reflux therapies.
Footnotes
Acknowledgments
The authors would like to express their gratitude to all who contributed to this research.
Author contributions
Xue Fan: Writing-Original Draft. Weiran Xu: Predictive Model Development. Lei Zhang: Writing-Review& Editing. Yanyan Shi: Statistical Methodology. Yuan Li: Writing-Review& Editing. Xiangchun Lin: Writing-Review& Editing. All authors have read and approved the final manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest.
Funding
This work was supported by the Peking University International Hospital Internal Grant (Grant Number YN2021QN03).