
Abstract
Objective
This study aimed to use root cause analysis to identify the underlying causes of defects in receiving loaner instruments and to implement an improvement plan.
Methods
In this retrospective study, 23,780 loaner instrument packages reprocessed by our central sterile supply department from January to July 2023, prior to the root cause analysis–based intervention, were classified into the control group, and 25,258 loaner instrument packages reprocessed by our central sterile supply department from January to July 2024, following the intervention, were classified into the experimental group. The overall incidence rate of defects, incidence rate of each defect, and 37 central sterile supply department staff members’ satisfaction with loaner instrument reprocessing before and after intervention were compared.
Results
Among the 23,780 packages in the control group, 409 (1.72%) exhibited receiving defects, whereas among the 25,258 packages in the experimental group, 159 (0.63%) had receiving defects. Instrument mismatch and lack of source information were identified as the primary receiving defects. Improvements to the training system, operating procedures, traceability system, and hierarchical supervision were the main contributors to the reduction in defects. The mean satisfaction score of the central sterile supply department staff improved from 89.92 to 93.03.
Conclusions
Root cause analysis can be used to reduce defects associated with loaner instrument receiving and improve staff satisfaction.
Keywords
Introduction
Leasing reusable medical devices from medical device companies is common in global healthcare services.1,2 However, this practice presents challenges in reprocessing these devices, especially those with complex structures, which can lead to surgical delays.3,4 Loaner instruments vary widely, particularly orthopedic devices, which are commonly used in surgeries to treat diseases and traumas of the bones, joints, and spine. The substantial variability between loaner instruments and basic surgical instruments makes the reprocessing of loaner instruments challenging. This increases the risk of quality control failures, thereby heightening the risk of nosocomial infections.
According to the National Healthcare Safety Network of the United States survey, the infection rates from 2006 to 2008 were 0.67%–2.4% among patients following femur replacement surgery and 0.68%–1.60% among patients following knee replacement surgery. 5 Surgical debridement and chemotherapy are often ineffective in controlling infections in patients with implants retained in the body. 6
Tipple et al. have reported that low- and middle-income countries exhibit poor quality practices in reusable medical device reprocessing (human resource allocation, material resources, and work procedures) compared with those in high-income countries, 2 resulting in higher surgical site infection rates.7,8 Therefore, it is important to ensure the quality and safety of loaner instruments and implants during leasing, receiving, cleaning, disinfection, and sterilization. 9 For reprocessing loaner instruments and implants, risk awareness among the central sterile supply department (CSSD) staff should be strengthened. Each reprocessing step should be considered, and standard operating procedures should be strictly followed to reduce the risk of nosocomial infections and ensure the quality of medical devices and patient safety. 3
After each use, the loaner instruments are sent by instrument suppliers to the CSSD’s decontamination area for handover. These instruments typically have complex structures and can be used across multiple healthcare institutions. Consequently, the number of loaner instruments is not fixed. If an inaccurate number of loaner instruments is collected or collection efficiency is low, reprocessing of loaner instruments becomes difficult, thereby affecting the progress and quality of reprocessing and delaying diagnosis and medical treatment. Adopting scientific and systematic management methods to optimize work procedures from the source has become an urgent concern for sterile item supply. Through comprehensive, systematic, and objective analyses, we hoped to determine the root causes and implement targeted intervention to reduce defects in loaner instruments during the conventional receiving process. Root cause analysis is a method of retrospective, structural analysis of problems 10 used to investigate root causes by analyzing adverse events and improving the process to prevent recurrence of similar events. Previous studies on loaner instruments have focused on cleaning quality, sterilization quality, and distribution management, whereas few studies have focused on the conventional receiving process of loaner instruments using root cause analysis.1,2,11–13 Therefore, this study aimed to employ root cause analysis to reduce the defect rate associated with the receiving of loaner instruments.
Methods
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. This was a retrospective study aimed at optimizing the CSSD’s conventional receiving process for loaner instruments after clinical use. The collected data included the names of medical device companies, names of device packages, quantities of devices in each package, and information about the CSSD staff. It did not include private information of the patients. This study was approved by the Biomedical Ethics Committee of West China Hospital, Sichuan University (2025 Nian Shen (63)). The need for written informed consent was waived by the Biomedical Ethics Committee of West China Hospital, Sichuan University. The Standards for Quality Improvement Reporting Excellence (SQUIRE) guidelines were followed. 14
Study design
A total of 23,780 loaner instrument packages reprocessed by our CSSD from January 2023 to July 2023 were classified into the control group, and 25,258 loaner instrument packages reprocessed by our CSSD from January 2024 to July 2024, after implementing improvements in reprocessing based on root cause analysis, were categorized into the experimental group. The data regarding defects were collected from the CSSD’s daily work shift report and through on-site investigation.
This study included loaner instruments that, after inspection and registration for receiving and temporary use following delivery, were cleaned, disinfected, packaged, and sterilized by our CSSD. The exclusion criteria were as follows: (a) basic surgical instruments, clinical instruments, and surgical bowls, which were delivered from other hospitals to our CSSD for reprocessing and (b) implants provided by external suppliers to our CSSD for centralized sterilization.
Structure of the loaner instrument management team
The loaner instrument management team was established in our CSSD in August 2023 and comprised 13 members. Of them, 1 was the head of the CSSD, 2 were head nurses, 3 were working group leaders, 1 was a quality controller, 1 was a teaching and training supervisor, 2 were device receiving personnel, 2 were device packaging personnel, and 1 was a device sterilization in-charge. Their average age was 42.69 years. With respect to their professional titles, 2 were co-chief nurses, 6 were supervising nurses, 4 were nurse practitioners, and 1 was a worker. Every team member had rich work and management experience in the CSSD.
Data collection
A quality controller (with >20 years of working experience in the CSSD and >5 years of research experience) reviewed work shift reports in August 2023 to identify the steps where problems occurred. On-site interviews were conducted to find similar events, determine the nature of the problems, and classify and record these issues.
Defects
Among the 23,780 loaner instrument packages received by our CSSD from January 2023 to July 2023, the following 409 defective cases were identified: 286 cases of instrument mismatch (quantity and model number of the instruments in the package were inconsistent with the information on the package label), 55 cases with inadequate source information (no receiving information), 41 cases with errors in delivery destination (information concerning delivery destination in the label was missing or different from the actual delivery destination), 12 cases of damaged instruments (instruments were missing, distorted, or functioned abnormally), 10 cases where instruments from different sources were mixed, and 5 cases with other defects. The defect rate was 1.72%. On analyzing the data using the Pareto principle, based on the 80/20 rule, where 80% of outcomes stem from 20% of causes, we found that defects caused by instrument mismatch and lack of source information accounted for 83.37% of all defective cases. Therefore, these two causes were identified as the primary receiving defects for loaner instrument packages (Figure S1).
Cause analysis
A structured, facilitated workshop was held to obtain more objective results for root cause analysis.15,16 The workshop duration was 5 h, and it included 16 participants from the loaner instrument management team for this project, the Disinfection Supply Committee of the Chinese Nursing Association, the Disinfection and Infection Control Committee of the China Health Inspection Association, and the China Hospital Association Logistics Specialized Committee. An experienced member of the research team served as the facilitator to ensure strict adherence to established procedures, focused discussions, and equal participation among workshop members. The content of this workshop included the following.
Factor determination
The facilitator clarified that the core issues were instrument mismatch and lack of source information in loaner instrument packages. Workshop participants were encouraged to brainstorm, provide supplementary information, and make revisions. The causes were determined from the following components: man, machine, material, method, and environment (Table S1, Figures S2 and S3).
Causality building
The facilitator instructed participants to conduct pairwise evaluations of all factors. For each pair, they discussed, “Can factor A directly cause factor B?” Causality was accepted if at least 80% of the participants agreed, and the resulting causal diagram was adopted in this study.
Consensus confirmation and revision
After the causal diagram was initially constructed, the facilitator instructed participants to conduct a comprehensive review, rediscussing disputed causal relationships and conducting anonymous voting (rating scale: 1, strongly disagree; 2, somewhat disagree; 3, neutral; 4, somewhat agree; 5, strongly agree). When at least two-thirds of participants assigned a rating of 4 or 5, the causality was considered widely supported, indicating that consensus had been reached. 17
Causality was presented in two causality matrix diagrams to visually represent the causal relationships among the factors (Figures S4 and S5). In these matrices, the number “1” indicated that the factor in the horizontal row was the result of the factor in the vertical column; the number “−1” indicated that the factor in the horizontal row was the cause of the factor in the vertical column; and the number “0” indicated no direct causality between the two factors. A large number of “−1” values occurred in the causality matrix diagrams, whereas “1”values were rare or absent, reflecting that the root cause was the initial cause of the causal relationship chain leading to the corresponding result. Ultimately, the root causes of instrument mismatch and lack of source information were identified as understaffing during peak hours, insufficient training, lack of supervision, inadequate operating procedures for receiving loaner instruments, and ineffective information traceability system (with the frequency of “−1” occurrence >3 times and the frequency of “1” occurrence 0 times).
Formulation of an improvement plan
The root causes included understaffing during peak hours, insufficient training, inadequate operating procedures for receiving loaner instruments, inefficient information traceability system, and lack of supervision by working group leader. Accordingly, the following improvement measures were formulated: optimizing personnel allocation, enhancing the training system, refining the receiving procedures for loaner instruments along with the information traceability system, and strengthening hierarchical supervision of loaner instruments.
Implementation of the improvement plan
Manpower optimization
The delivery of loaner instruments was standardized and streamlined. Two CSSD nursing staff members were assigned to the receiving positions during peak hours in the morning and afternoon each day to manage end-to-end receiving of loaner instruments. This could prevent errors caused by irrelevant personnel helping the receiving personnel in counting the instruments. Due to the high level of difficulty and risk associated with receiving loaner instruments, the frequency of rotation between receiving posts and other posts within the CSSD should be minimized. Ensuring that the same personnel handles instrument receiving for an extended period of time allows them to gain sufficient work experience, thereby reducing defects caused by frequent rotations and incompetence of receiving personnel. In addition, a double-check position for receiving loaner instruments was created in the CSSD. Flexible shift scheduling was implemented, with manpower dynamically adjusted based on peak and off-peak surgery days to match workload fluctuations. A “flexible manpower reserve” for loaner instrument reprocessing was created in the CSSD. In cases of a sudden increase in the workload for loaner instrument receiving or manpower shortages, members of the flexible manpower reserve would automatically take over to prevent congestion or errors in the instrument receiving process, thereby maintaining overall work efficiency.
Improvement of the training system
A knowledge graph learning library for medical devices was developed using the information traceability system, enabling CSSD staff to access it at any time and perform online and offline self-study using the printed graph album. A hierarchical training system was established for CSSD staff involved in loaner instrument reprocessing throughout their entire career cycle (from onboarding to offboarding). For loaner instruments with complex or special structures, suppliers were invited to provide training through on-site demonstrations and WeChat video calls. Professional training and assessment sessions were offered to CSSD staff on a quarterly basis, enabling them to master the functions, structures, disassembly, and assembly of loaner instruments; this enhanced their understanding and identification of the devices while preventing defects caused by staff incompetence. Training was also provided to the CSSD staff on job responsibilities and communication skills. Daily, monthly, and quarterly data on defects during loaner instrument reprocessing were analyzed, and case study seminars were held based on the results.
Improvement of the operating procedures
A dedicated liaison system was established between loaner instrument suppliers and CSSD staff. Suppliers were required to submit loaner instrument delivery applications through the system at least 4 h in advance, minimizing time wastage. An emergency manpower allocation mechanism for peak periods of loaner instrument reprocessing was developed within the CSSD. A training system for loaner instrument reprocessing and an emergency response plan for using the information traceability system were also developed, strengthening specialized training management and emergency handling. Standardized operating procedures for receiving loaner instruments were developed (Figure S6), clearly defining inspection details and the double-check mechanism. Job responsibilities for loaner instrument reprocessing personnel were clearly defined and a work performance evaluation form was created. Handover rules for loaner instruments were optimized using an electronic daily handover system. This enabled loaner instrument reprocessing personnel to quickly inquire about reprocessing information and easily track any issues.
Improvement of the information traceability system
The module for loaner instruments in the information traceability system was optimized. Electronic images of each loaner instrument were imported into the system’s backend. Individual login account was created for each supplier, enabling them to update loaner instrument information in a timely manner, thus allowing the receiving personnel to consult and review the updates in real time. A refined management approach was adopted in collaboration within the CSSD. Electronic illustration diagrams for 56 types of loaner instruments from 13 suppliers, including high-resolution overall images captured by cameras and smallest-unit images after disassembly, were prepared for the CSSD staff. Detailed configuration lists for loaner instruments were also provided, which indicated the quantity of instruments in each package and the quantity of the components for each instrument after disassembly, facilitating identification of loaner instruments across various working scenarios. The electronic illustration diagrams enabled real-time updates, searches, and checks on loaner instruments, reducing the risk of errors during receiving and assembly processes while improving the efficiency of loaner instrument reprocessing. A visual identification system compatible with the traceability system was implemented in the CSSD. When doubts arose about loaner instruments during the handover process, they could be placed on the equipment for scanning; this triggered a search of the electronic illustration diagrams within the traceability system to retrieve detailed information about the instrument, including its appearance, model number, quantity, and the name of the package to which it belonged.
Strengthening the hierarchical supervision of loaner instruments
A three-level quality control system for loaner instruments was developed in the CSSD. The head of the CSSD and the head nurses completed the level-3 quality control. They were responsible for building the organizational structure for loaner instrument management and regulating human resources and equipment. They supervised the quality control nurses as they completed routine and regular special quality control tasks and organized regular meetings to discuss and analyze feedback problems and assessment results to ensure continuous quality improvement. For level-2 quality control, the dynamic quality controller was responsible for performing daily spot checks and guiding working group leaders in proper receiving management of loaner instruments; the education and training specialist provided training and conducted assessments. For level-1 quality control, working group leaders provided on-site guidance for frontline staff during the morning and afternoon peak receiving hours every day. They evaluated quality using the work performance rating form. Each level of quality control management strictly implemented a closed-loop process of “standard—execution—monitoring—evaluation—feedback—improvement.”
Verification and confirmation
The teaching and training supervisor implemented and assessed the training plan. The working group leaders analyzed and reported abnormal events daily according to work shift reports and inspected them monthly using the relevant quality control checklist. Data were dynamically collected by the quality controller, and the identified problems were analyzed for continuous quality improvement. For any difficulties encountered during the implementation, discussions were organized by head nurses to bring unresolved issues into the next continuous quality improvement cycle.
Evaluation criteria
Relevant indicators before and after the root cause analysis–based improvements to loaner instrument receiving were compared. These included the following: (a) defect rates for conventional loaner instrument receiving before and after the improvements; (b) the contribution of each improvement measure to defect reduction; and (c) CSSD staff satisfaction before and after the improvements.
A questionnaire titled “Central Sterile Supply Department Staff Satisfaction Survey on Loaner Instrument Reprocessing” was developed following discussions among project members, tailored to the CSSD’s context (Supplemental file 1). It comprises 20 items addressing the delivery and handover of loaner instruments by suppliers, rationality and smoothness of each work process within the CSSD, working environment and operating tools in the CSSD, management support within the CSSD, coordination among CSSD staff at different positions, and training. A five-point Likert scale was used, with response options rated as follows: 5, very satisfied; 4, satisfied; 3, neutral; 2, unsatisfied; and 1, very unsatisfied. A total of 37 questionnaires were distributed before and after the improvements to assess the satisfaction level of CSSD staff members with loaner instrument reprocessing. All 37 questionnaires were completed and returned before and after the improvements, achieving a 100% response rate. Corrected item–total correlation values ranged from 0.536 to 0.819, with a Cronbach’s alpha of 0.946 and a Kaiser–Meyer–Olkin value of 0.670, indicating good reliability and validity.
Statistical analysis
The Statistical Package for Social Sciences (SPSS) software (version 27.0, International Business Machines Corporation; USA) was used for data analyses. Continuous variables were reported as mean ± SD and noncontinuous variables as frequencies or percentages. After conducting the pre-survey regarding satisfaction among the CSSD staff, reliability analysis using Cronbach’s alpha coefficient was performed to evaluate the internal consistency of the scale. A Cronbach’s alpha coefficient ≥0.7 indicated good internal consistency of the scale. The validity analysis used the Kaiser–Meyer–Olkin test and Bartlett’s test of sphericity to evaluate the questionnaire’s structural validity. The Kaiser–Meyer–Olkin value was used to determine whether the sample data were suitable for factor analysis, with higher values indicating greater suitability of the data for factor analysis. Bartlett’s test of sphericity was used to determine whether the data’s correlations were sufficiently strong. Chi-square test (χ2) was used to compare the overall incidence rate of defects, incidence rate of each defect, and improvement in each defect before and after the intervention. A p value of <0.05 indicated statistically significant difference. Paired t-test was performed to compare the satisfaction scores of the same respondents before and after the intervention.
Results
Defect rates for loaner instrument receiving
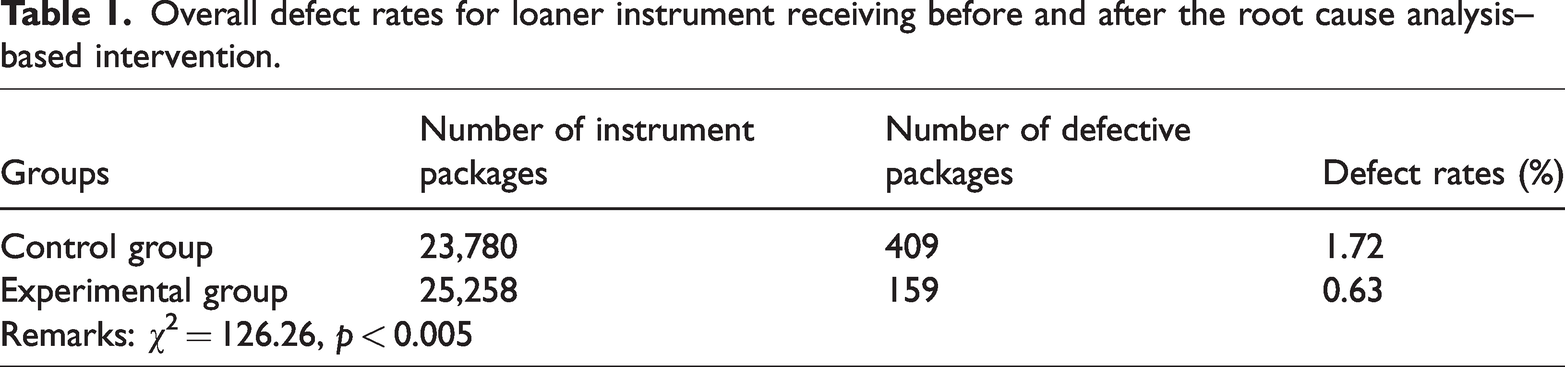
There were 409 defective cases in the control group, with a defect rate of 1.72% and 159 defective cases in the experimental group, with a defect rate of 0.63%. Chi-square analysis showed that defect rates were associated with the classification of groups, and a statistically significant difference was identified (χ2 = 126.26, p < 0.001). The control and experimental groups had different numbers of defective cases. The defect rates for loaner instrument receiving in the experimental group was significantly lower than that in the control group, as shown in Table 1.
Overall defect rates for loaner instrument receiving before and after the root cause analysis–based intervention.
The overall defect rate in 2024 was significantly lower than that in 2023. Variations in the defect rate across the 12 months of 2024 were smaller than those observed in 2023, with no significant increases detected. These changes indicated that defect incidence became more stable and controllable after the interventions were implemented (Figure S7).
Types of defects for loaner instrument receiving
Chi-square analyses indicated that defects caused by instrument mismatch were associated with the classification of groups (χ2 = 114.205, p < 0.001). The two groups had different defect rates caused by instrument mismatch, with significantly higher defect rate in the control group than that in the experimental group. Similarly, the defect caused by the lack of source information was associated with the classification of groups (χ2 = 17.574, p < 0.001). The two groups had different defect rates due to the lack of source information, with significantly higher defect rate in the control group than that in the experimental group. In contrast, the classification of groups was not associated with the defects caused by delivery destination errors, damaged instruments found in the instrument packages, mixing of packages from different sources, and other defects, with no statistically significant differences observed between the two groups, as shown in Table 2.
Types of defects for loaner instrument receiving before and after the root cause analysis–based intervention.

Data in parentheses are expressed as percentages.
Contribution of improvement measures to defect reduction associated with instrument mismatch
A reduction rate of 68.53% was observed in the number of defective cases resulting from instrument mismatch between 2023 (286 defective cases) and 2024 (90 defective cases) (χ2 = 12.186, p = 0.016), suggesting that the improvement measures effectively reduced these defects (Table 3).
Root cause analysis–based intervention for instrument mismatch.

The incidence of understaffing during peak hours decreased from 73 to 30, a 58.90% reduction, suggesting that optimizing manpower allocation was a key driver in the overall decrease in the defect rate. This demonstrates that such optimization can substantially reduce errors associated with understaffing during peak hours.
The incidence of insufficient supervision decreased from 175 to 68, representing a 61.14% decline. Similarly, the incidence of insufficient training reduced from 175 to 38 over the same period, reflecting a 78.29% decrease. These findings indicated that strengthening the hierarchical supervision of loaner instruments and improving the training system substantially contributed to the reduction in defect rates. Establishing a three-level quality control system for loaner instruments can effectively reduce instrument manipulation errors. By leveraging the information traceability system to create a knowledge graph learning library for loaner instruments, increasing on-site and online training for those with complex or special structures, and strengthening periodic assessments, the CSSD staff’s awareness regarding standardized operations and operational proficiency was enhanced, which became an important internal driving force for reducing defect rates.
The incidence of inadequate information traceability system decreased from 29 to 3, representing an 89.66% reduction. This substantial improvement demonstrated that the application of digital means (such as the creation of electronic illustration diagrams and installation of visual identification equipment for loaner instruments) effectively reduced human errors and enhanced instrument identification accuracy. The incidence of inadequate operating procedures involved in receiving loaner instruments decreased from 9 to 4, indicating a 55.56% reduction. This also reflected continuous progress in improving work procedures and standardizing execution.
Improving the information traceability system, training system, and hierarchical supervision of loaner instruments contributed the most to reducing defects resulting from instrument mismatch.
Contribution of improvement measures to defect reduction associated with lack of source information
A reduction rate of 63.64% was observed in the number of defective cases resulting from lack of source information between 2023 (55 defective cases) and 2024 (20 defective cases) (χ2 = 12.512, p = 0.002), indicating that improvement measures effectively reduced these defects (Table 4).
Root cause analysis–based intervention for lack of source information.
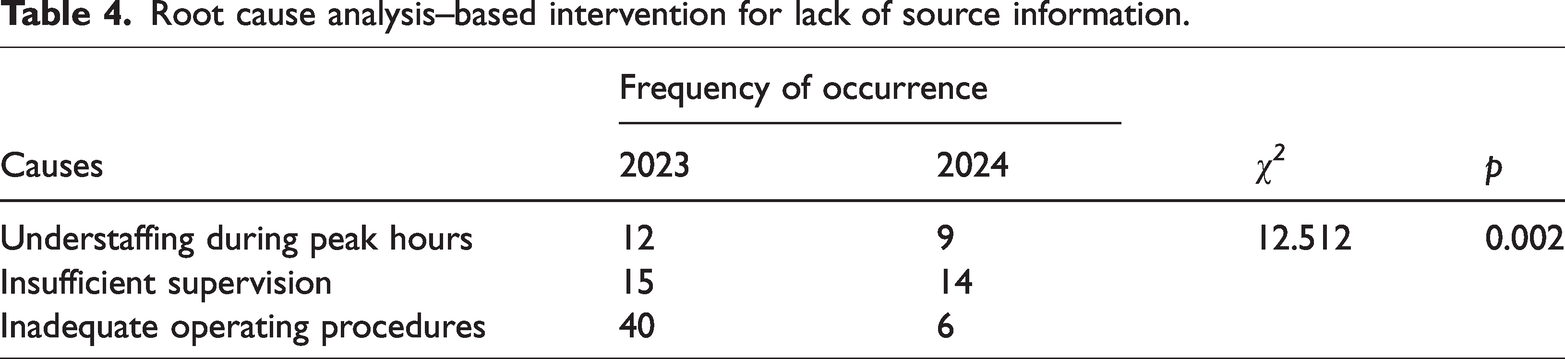
The incidence of understaffing during peak hours decreased from 12 to 9, representing a 25.00% reduction, which indicated that optimizing manpower allocation helped reduce such defects.
The incidence of insufficient supervision decreased from 15 to 14. This small reduction suggested that improvements to the regulatory mechanism may not have been fully implemented or effectively executed, resulting in limited contribution on reducing the defect rate.
The incidence of inadequate operating procedures for receiving loaner instruments decreased from 40 to 6, reflecting an 85% reduction. This substantial change indicated that measures to standardize operating procedures played a key role in reducing defects caused by the lack of source information. Standardizing operating procedures contributed most to reducing improper handling, thereby lowering defects due to a lack of source information.
Satisfaction among CSSD staff
Among the 37 CSSD staff members investigated, the satisfaction score after implementing improvements was 93.03 ± 6.98, significantly higher than the pre-improvement score of 89.92 ± 7.38, as shown in Table 5. Paired t-test comparing satisfaction scores before and after the improvements revealed a significant difference (t (36) = −10.29, p < 0.001. When expressed as “after improvement−before improvement,” the mean difference in the score was 3.11 (95% confidence interval: 2.50, 3.72). These findings indicated that the improvement measures led to a meaningful enhancement in satisfaction.
Satisfaction among CSSD staff before and after the root cause analysis–based intervention.

CSSD: central sterile supply department.
Discussion
The CSSD can be considered the “heart” of a hospital because it plays a significant role in controlling nosocomial infections. More and more loaner instruments are being commonly used in hospitals. The reprocessing and use of loaner instruments involve multiple departments and steps; therefore, the risk of surgical site infections caused by loaner instruments is higher than that caused by basic surgical instruments. According to investigations on bacterial sources at surgical sites,18,19 the source was air in 5% cases; patient skin in 50%; mouth, nose, and hands of patients who had undergone surgery in 35%; and surgical instruments in 10%. 20 With respect to adverse events associated with medical devices, ≥85% were caused by implants. 21 The progress and development of trauma surgery have increased the use of loaner instruments and implants. Loaner instruments may pose risks to surgical outcomes and patient prognosis. 22 Therefore, it is crucial to strengthen the management of loaner instrument reprocessing.
Application of root cause analysis could effectively reduce the occurrence of adverse events during the conventional receiving of loaner instruments
In response to defects in loaner instrument reprocessing in the CSSD, a root cause analysis was conducted to identify proximate causes based on defect timing, work steps, and frequency of occurrence; isolate direct causes; and analyze causality to determine the root causes. These causes included understaffing during peak hours, insufficient training, inadequate operating procedures for receiving loaner instruments, ineffective information traceability system, and lack of supervision. Key improvement measures included refining the conventional handover process for loaner instruments, optimizing staffing, enhancing training, improving electronic illustration diagrams for loaner instruments to enable reprocessing personnel to conveniently consult and verify information on instrument packages, and strengthening quality control supervision at all management levels. The study results demonstrate that improvements to the training system, operating procedures, information traceability system, and hierarchical supervision played a key role in reducing defects caused by instrument mismatch and lack of source information. This suggests that root cause analysis can effectively identify underlying causes of adverse events. Targeted measures can lead to overall standardization and refinement of loaner instrument management and manipulation, thereby reducing the incidence of similar events. Therefore, these findings highlight the practical application value of root cause analysis.
Application of root cause analysis could effectively improve satisfaction levels among loaner instrument reprocessing personnel
The receiving process for loaner instruments differs from that of other reusable medical devices. Their complex structures make reprocessing loaner instruments difficult and risky. The receiving step initiates the entire reprocessing workflow, with its quality and efficiency directly affecting the safety and timeliness of subsequent steps. Any failures or errors in receiving can trigger ongoing corrections later, consuming considerable time and effort, slowing the progress, and affecting the reprocessing personnel’s emotional state and work quality. Therefore, greater attention must be given to the conventional receiving of loaner instruments.
Staff satisfaction with work content reflects the sense of fulfillment they derive from daily tasks and their recognition of them. It also indirectly indicates the rationality of work arrangement as well as the orderliness and efficiency of processes. To address weaknesses in the receiving process for loaner instruments, work procedures were revised and refined; nurses were assigned to receiving positions; a double-check mechanism was implemented; supervisors’ job responsibilities were specified; training was strengthened; and the information traceability system was improved. These measures enhanced staff competence and cooperation, improved their professional skills and problem-solving abilities, provided support for facilities and management, and established a clear system and process for the staff to follow. This study demonstrated that applying root cause analysis can improve satisfaction levels among reprocessing personnel handling loaner instruments, enabling smoother implementation of loaner instrument reprocessing and enhancing its quality and efficiency. It highlighted that monitoring defective cases using root cause analysis to identify problems and implementing targeted improvement measures can ensure the continuity and quality of the reprocessing work. This approach contributed to enhanced recognition by the staff regarding the importance of their work. 23
Limitations
This single-center retrospective study used data collection and root cause analysis to identify the key steps and primary factors associated with defects occurring in the conventional receiving process for loaner instruments. Based on the root cause analysis, comprehensive improvement measures were implemented, resulting in reduced defect rate in the conventional receiving process of loaner instruments. The satisfaction of CSSD staff who reprocessed the loaner instruments was analyzed before and after the improvements. However, this study was conducted in a single CSSD, with a limited sample size and short observation period. The study results need to be validated through wider application to enhance their generalizability. In addition, this study focused on the receiving process of loaner instruments, and the satisfaction survey was conducted only with the CSSD staff. The satisfaction of staff members from other departments was not investigated, limiting the study’s comprehensiveness. A multicenter study will be necessary to conduct full life-cycle management of loaner instruments for long-term monitoring, continuous quality tracking, and improvement. Greater attention should be given to comprehensively reviewing and considering various influencing factors. For example, personal characteristics (age, work experience, and professional qualifications) should be considered to improve the study design and enhance the analysis, thereby providing a basis for managing loaner instrument reprocessing.
Conclusions
CSSD is a hospital department responsible for reprocessing all reusable medical devices. It is crucial for the smooth implementation of diagnosis and treatment as well as patient safety. China’s relevant national standards and the guidelines for reprocessing loaner instruments issued by the Chinese Nursing Association emphasize the importance of strengthening standardized management of loaner instruments. CSSDs must adapt to changing times, adjust traditional working mode, and integrate information technology with other means to manage loaner instruments effectively. Such measures could constantly improve risk control and help overcome difficulties at work. It is necessary to make full use of scientific quality management tools to explore the organizational and systematic reasons behind the problems, thereby improving the reprocessing procedures of reusable medical devices.
Supplemental Material
sj-jpg-1-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-jpg-1-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Supplemental Material
sj-jpg-2-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-jpg-2-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Supplemental Material
sj-jpg-3-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-jpg-3-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Supplemental Material
sj-jpg-4-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-jpg-4-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Supplemental Material
sj-jpg-5-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-jpg-5-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Supplemental Material
sj-jpg-6-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-jpg-6-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Supplemental Material
sj-jpg-7-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-jpg-7-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Supplemental Material
sj-pdf-8-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-pdf-8-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Supplemental Material
sj-pdf-9-imr-10.1177_03000605251407884 - Supplemental material for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study
Supplemental material, sj-pdf-9-imr-10.1177_03000605251407884 for Using root cause analysis to improve the quality of loaner instrument receiving in the central sterile supply department: A retrospective study by Nian Qin, Hao Huang, Hui Chen, Jingyu Rao, Xiaoli Zhou, Aiying Zeng and Qing Zeng in Journal of International Medical Research
Footnotes
Acknowledgments
Not applicable.
Authors’ contributions
Nian Qin: Conceptualization, Methodology, Investigation, and Writing-original draft
Hao Huang: Conceptualization, Methodology, and Writing-review and editing
Hui Chen: Investigation and Writing-review and editing
Jingyu Rao: Formal analysis, Data curation, and Writing-review and editing
Xiaoli Zhou: Investigation and Writing-review and editing
Aiying Zeng: Investigation and Writing-review and editinga
Qing Zeng: Investigation and Writing-review and editing
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki (1975, as revised in 2024). All research methods were conducted in accordance with the relevant guidelines and regulations. This study was approved by the Biomedical Ethics Committee of West China Hospital, Sichuan University (2025 Nian Shen (63)). The need for written informed consent was waived by the Biomedical Ethics Committee of West China Hospital, Sichuan University.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.