
Abstract
Objective
This study compared the perioperative outcomes following neoadjuvant immunochemotherapy in elderly (≥70 years) and non-elderly patients with esophageal squamous cell carcinoma.
Methods
This retrospective study included patients with locally advanced esophageal squamous cell carcinoma who underwent neoadjuvant immunochemotherapy followed by esophagectomy (July 2020–June 2024). Patients were stratified into elderly (≥70 years) and non-elderly groups. Primary outcomes included 30-day mortality, 90-day mortality, 30-day readmission rate, and R0 resection rate. Secondary outcomes included pathological complete response, major pathological response, post-neoadjuvant pathological tumor/node stages, tumor regression grade, and complications.
Results
Among 73 patients (25 elderly, 48 non-elderly), no 30-day or 90-day mortality occurred in either group. The 30-day readmission rates (P = 0.331) and R0 resection rates (P > 0.999) were comparable between the two groups. Secondary outcomes, including pathological complete response (P = 0.685), major pathological response (P = 0.417), post-neoadjuvant pathological tumor stage (P = 0.732), post-neoadjuvant pathological node stage (P = 0.124), and tumor regression grade (P = 0.081), also showed no significant differences. The rates of complications, including severe (P = 0.825), pulmonary (P = 0.314), and cardiac (P = 0.269) complications; anastomotic leakage (P > 0.999); recurrent laryngeal nerve palsy (P > 0.999); and wound complications (P > 0.999), were similar between the two groups.
Conclusion
Elderly and non-elderly patients exhibited similar 30- and 90-day mortality, readmission, and R0 resection rates as well as comparable pathological responses and complication profiles following neoadjuvant immunochemotherapy. These findings indicate that age alone cannot exclude elderly patients from receiving neoadjuvant immunochemotherapy, and patients should undergo thorough individualized assessment and optimization.
Keywords
Introduction
Esophageal cancer ranks as the 11th most common malignancy and the 6th leading cause of cancer-related mortality worldwide. 1 In 2020, esophageal cancer accounted for approximately 604,100 new cases and 544,100 deaths globally, with age-standardized incidence and mortality rates of 6.3 and 5.6 per 100,000, respectively. 2 China presents a disproportionately high burden, accounting for over 50% of global cases, with esophageal squamous cell carcinoma (ESCC) comprising over 90% of cases.3,4 In certain high-risk regions of China, the incidence of ESCC exceeds 100 per 100,000 individuals, underscoring the urgent need for improved prevention, early detection, and treatment strategies.5,6 Although early-stage esophageal cancer is primarily treated with surgery, most patients are diagnosed at an intermediate or advanced stage, resulting in low curative rates and a high risk of recurrence and metastasis. 7 Consequently, optimizing perioperative management and multimodal therapy has become a key focus to improve both short- and long-term outcomes following esophagectomy.
In recent years, programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) inhibitors have significantly improved the survival rate in patients with esophageal cancer, with regimens combining immune checkpoint inhibitors (ICIs) and chemotherapy outperforming conventional treatments. Studies such as KEYNOTE-590, 8 JUPITER-06, 9 and ORIENT-15 10 have demonstrated that neoadjuvant immunochemotherapy (nICT) can activate antitumor immunity, reduce tumor burden, and improve the tumor microenvironment, thereby enhancing survival. In addition to improved oncological outcomes, emerging evidence indicates that nICT demonstrates acceptable perioperative safety profiles. Several retrospective and multicenter studies have shown that nICT does not increase postoperative morbidity or mortality compared with neoadjuvant chemotherapy or neoadjuvant chemoradiotherapy (nCRT) while maintaining high R0 resection and pathological response rates.11–13
However, older patients remain underrepresented in these studies, limiting the understanding of their perioperative tolerance and long-term outcomes. Given that elderly patients with ESCC often have comorbidities and reduced physiological reserve, evaluating whether nICT yields comparable perioperative results in this group is critical. Evaluating perioperative mortality, readmission, surgical radicality, and other short-term outcomes in elderly versus non-elderly patients with ESCC undergoing nICT followed by surgery may help address this evidence gap. Previous meta-analyses have shown that elderly patients undergoing esophagectomy experience substantially higher perioperative risks than younger patients, including approximately 1.5–2-fold higher rates of overall complications and short-term mortality. 14 However, recent evidence suggests that with careful preoperative selection and management of comorbidities, elderly patients with ESCC can achieve complication rates and survival outcomes comparable to those of their non-elderly counterparts. 15
With increasing life expectancy and a rising proportion of elderly patients with ESCC, 16 it has become increasingly important to determine whether the safety and efficacy of nICT observed in general populations also apply to this vulnerable group. Elderly patients often face higher perioperative and surgical risks due to declining organ function and multiple comorbidities, including hypertension, diabetes, and coronary heart disease. 17 Research on nICT in elderly patients with ESCC remains relatively limited. Therefore, this study aimed to compare the perioperative outcomes between elderly and non-elderly patients with locally advanced ESCC who underwent nICT followed by esophagectomy.
Methods
Study design and participants
This retrospective study enrolled patients with locally advanced ESCC who underwent nICT followed by esophagectomy at our hospital between July 2020 and June 2024. The inclusion criteria were as follows: (a) histopathologically confirmed ESCC; (b) received nICT; (c) clinical stage II–IV A (cT2N+M0 or cT3anyNM0) based on standardized physical and imaging examinations, including positron emission tomography–computed tomography (PET–CT) and ultrasound; and (d) an Eastern Cooperative Oncology Group (ECOG) performance status score of 0 or 1 (0 indicating full activity and 1 indicating the inability to perform strenuous physical activity). Exclusion criteria included the following: (a) nonsquamous histological types of esophageal malignancies; (b) a history of other malignancies; (c) major organ dysfunction precluding surgery; and (d) prior treatment with radiotherapy, targeted therapy, chemotherapy, or immunosuppressive agents. Ethical approval for this study was obtained from the Ethics Committee of our hospital, and all procedures were conducted in accordance with the principles of the Declaration of Helsinki. Given the retrospective nature of the study, the requirement for informed consent was waived by the ethics committee.
Patients were divided into elderly (aged ≥70 years) 18 and non-elderly (aged <70 years) groups based on age. For both elderly and non-elderly patients, the neoadjuvant chemotherapy regimens were consistent in terms of drug selection, dosage, and treatment cycles. No dose reductions or adjustments were made in the elderly group, as all patients met ECOG performance status 0–1 and had no severe organ dysfunction, ensuring comparability and clinical relevance of the two groups.
Data collection and outcomes
Data were obtained from medical records, including age, sex, body mass index (BMI), smoking, alcohol drinking, comorbidities, tumor location, staging before treatment, use of ICIs, treatment cycles, treatment-to-surgery intervals, ECOG scores, and complications of neoadjuvant therapy. The ECOG score is mainly obtained by directly interviewing the patients and their family members and by combining the clinical observation of the patients’ daily activity abilities.
The primary outcomes included 30-day mortality, 90-day mortality, 30-day readmission rate, and R0 resection rate. Secondary outcomes included pathological complete response (pCR), major pathological response (MPR), pathological staging after neoadjuvant therapy (post-neoadjuvant pathological tumor (ypT) and post-neoadjuvant pathological node (ypN) stages), tumor regression grading (TRG), and complications, including severe complications (Clavien–Dindo grade > 2), pulmonary complications, cardiac complications, anastomotic leakage, recurrent laryngeal nerve palsy, and wound complications. Tumor response was evaluated 3–5 weeks after completing at least two cycles of nICT using the Response Evaluation Criteria in Solid Tumors (RECIST 1.1). A multidisciplinary team assessed the tumor response by comparing baseline imaging data with contrast-enhanced CT of the chest and abdomen, cervical ultrasound, and PET–CT. The pCR was defined as the complete absence of residual tumor cells, while MPR was characterized by the presence of less than 10% residual tumor cells. 19 The R0 resection rate was determined as the proportion of patients achieving complete tumor resection with no residual tumor tissue at the resection margins, confirmed by pathological examination. Pathological staging following neoadjuvant therapy was determined according to the 8th edition of the American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) guidelines. TRG was assessed based on the criteria established by the College of American Pathologists/National Comprehensive Cancer Network (CAP/NCCN), which classifies tumor regression into four grades: TRG0 (no residual tumor), TRG1 (residual tumor cells appearing as single cells or small clusters), TRG2 (partial residual tumor), and TRG3 (no regression). Postoperative complications were classified using the Clavien–Dindo grading system, 20 which categorizes complications into five grades based on their severity and type of intervention required. Grades I and II represent mild-to-moderate complications managed conservatively or with medication, while grades III to V represent more serious conditions. Specifically, grade III complications require surgical, endoscopic, or radiological intervention; grade IV includes life-threatening complications requiring intensive care unit (ICU) management; and grade V refers to death due to complications. In clinical practice, grade III–V complications are generally considered severe and may pose a significant risk to patient outcomes.
Statistical analysis
All statistical analyses were performed using SPSS version 28.0 (IBM Corp., Armonk, NY). Normally distributed data were expressed as mean ± standard deviation and compared between groups using the independent t-test. Non-normally distributed data were expressed as median (interquartile range) and analyzed using the Mann–Whitney U test. Categorical data were reported as counts and percentages (n, %) and compared using the chi-square (χ2) test or Fisher’s exact test. Two-sided P-values <0.05 were considered statistically significant.
Results
Baseline and nICT characteristics
A total of 73 patients with ESCC were included, comprising 25 patients in the elderly group and 48 in the non-elderly group. No statistically significant differences were observed between the two groups in terms of sex distribution (male: 88.0% vs. 97.9%, P = 0.113), BMI (23.18 [20.45, 24.51] vs. 22.00 [20.02, 24.34], P = 0.613), smoking (68.0% vs. 58.3%, P = 0.581), alcohol drinking (56.0% vs. 60.4%, P = 0.910), or comorbidities such as hypertension (56.0% vs. 35.4%, P = 0.150), diabetes mellitus (12.0% vs. 16.7%, P = 0.738), and coronary heart disease (8.0% vs. 6.2%, P > 0.999). Regarding tumor staging, no significant difference was observed in the clinical N stage (P = 0.649) or TNM stage (P = 0.232). No significant differences were observed between the elderly and non-elderly groups in terms of ICIs used (P = 0.124), number of treatment cycles (P = 0.597), treatment-to-surgery interval (41 vs. 38 days, P = 0.572), or ECOG performance status score ≥ 1 (8.0% vs. 6.2%, P > 0.999). During neoadjuvant treatment, adverse events were observed in 32.0% of elderly patients and 37.5% of non-elderly patients, without significant differences between the two groups (P = 0.641). The main adverse events included gastrointestinal discomfort (16.0% vs. 20.8%, P = 0.619), hematologic abnormalities (20.0% vs. 16.7%, P = 0.754), and rashes (12.0% vs. 10.4%, P > 0.999) (Table 1).
Baseline and nICT characteristics.

BMI: body mass index; ICIs: immune checkpoint inhibitors; ECOG: Eastern Cooperative Oncology Group; nICT: neoadjuvant immunochemotherapy.
Perioperative characteristics
No significant differences were observed in the operation duration (5.00 [5.00, 6.50] vs. 6.25 [5.00, 7.13] h, P = 0.143), blood loss (100 [50, 100] vs. 50 [50, 100] mL, P = 0.208), or number of resected lymph nodes (20 [15, 28] vs. 25 [17.75, 33.25], P = 0.151). Postoperative hospital duration was comparable between the two groups (19 [15, 23] vs. 15.5 [13.75, 23.25] days, P = 0.308). The distribution of surgical procedures also did not vary significantly. Minimally invasive McKeown esophagectomy was performed in 92.0% and 93.8% of the elderly and non-elderly patients, respectively (P > 0.999). The rates of ICU admission (8.0% vs. 6.2%, P > 0.999) and unplanned reoperation (4.0% vs. 2.1%, P > 0.999) were low in both groups (Table 2).
Perioperative characteristics.

ICU: intensive care unit.
Outcomes
No 30-day or 90-day mortality occurred in either group. The 30-day readmission (12.0% vs. 4.2%, P = 0.331) and R0 resection (96.0% vs. 95.8%, P > 0.999) rates were similar between elderly and non-elderly patients. Secondary outcomes, including pCR (12.0% vs. 8.3%, P = 0.685), MPR (28.0% vs. 37.5%, P = 0.417), ypT stage (P = 0.732), ypN stage (P = 0.124), and TRG (P = 0.081), also showed no significant differences. The rates of complications, including severe (24.0% vs. 18.8%, P = 0.825), pulmonary (44.0% vs. 29.2%, P = 0.314), cardiac (8.0% vs. 2.1%, P = 0.269) complications; anastomotic leakage (4.0% vs. 6.2%, P > 0.999); recurrent laryngeal nerve palsy (8.0% vs. 6.3%, P > 0.999); and wound complications (12.0% vs. 10.4%, P > 0.999), were comparable between the two groups (Table 3).
Outcomes between the two groups.
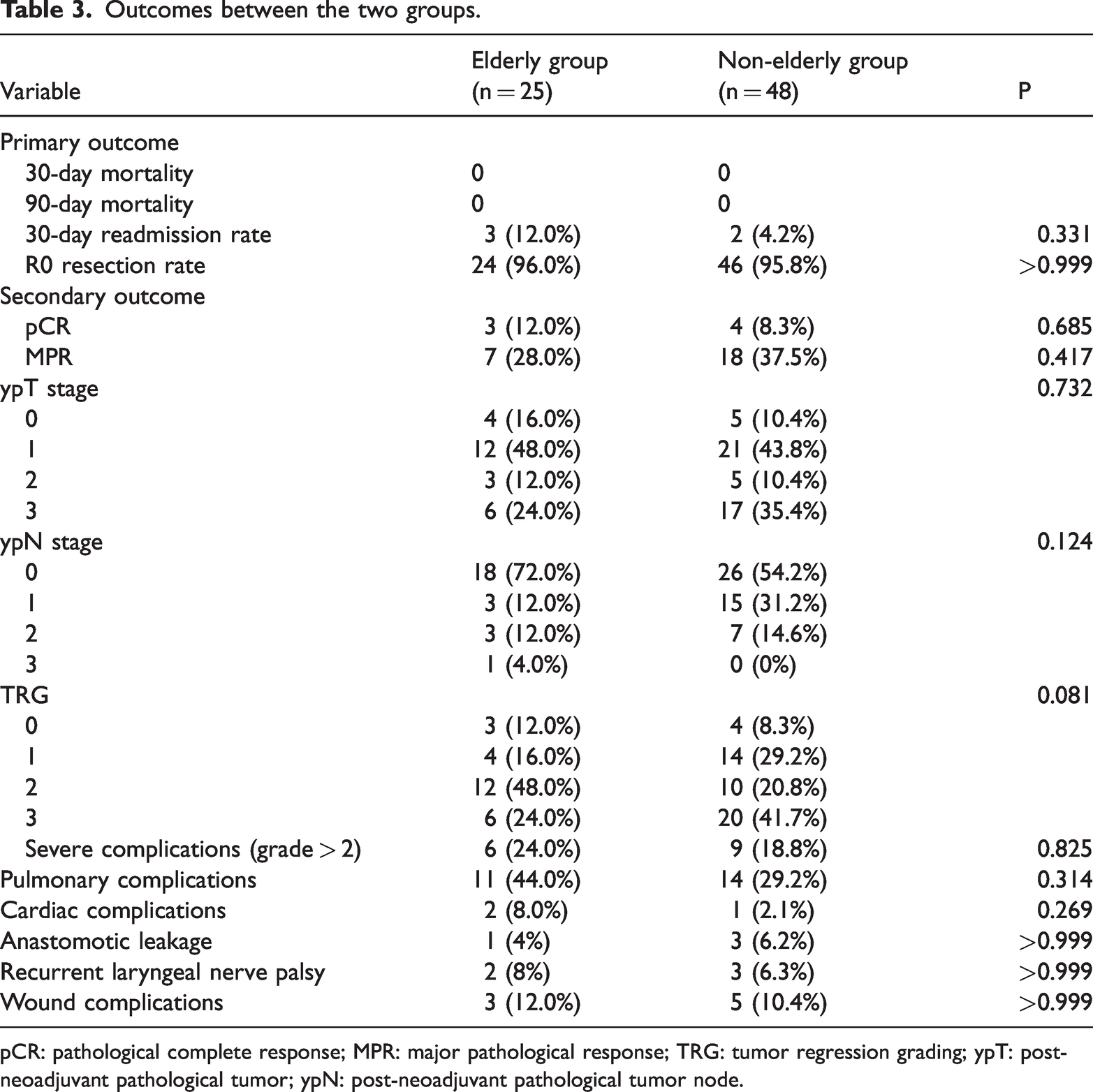
pCR: pathological complete response; MPR: major pathological response; TRG: tumor regression grading; ypT: post-neoadjuvant pathological tumor; ypN: post-neoadjuvant pathological tumor node.
Discussion
This study demonstrated no significant differences in 30-day mortality, 90-day mortality, 30-day readmission rate, R0 resection rates, or secondary outcomes, including pCR, MPR, TRG score, and treatment-related complications between the elderly and non-elderly groups. These results suggested that advanced age alone could not exclude elderly patients from receiving nICT. Individualized physical status evaluation is crucial for optimal therapeutic decision-making, highlighting the clinical potential of nICT in elderly populations.
With the accelerated aging of the society, the proportion of elderly patients with ESCC has gradually increased, 21 prompting investigation into appropriate treatment strategies for this population. nICT has emerged as a promising therapeutic option for ESCC. 11 In this study, neither elderly nor non-elderly patients experienced 30-day or 90-day mortality, indicating that nICT followed by surgery was well tolerated perioperatively across age groups. These findings align with those of recent studies demonstrating the safety of nICT in ESCC. A retrospective study reported favorable perioperative outcomes, with nICT exhibiting a lower rate of surgical complications than nCRT and comparable rates to neoadjuvant chemotherapy alone. 12 Similarly, another study demonstrated superior 2-year overall survival rates for nICT versus surgery alone, with no grade ≥3 postoperative complications. 13
The 30-day readmission rate was slightly higher in the elderly group, although not statistically significant. Most readmissions were attributed to manageable postoperative complications and did not result in mortality. These findings align with those of a multicenter phase 2 study in which perioperative nivolumab with chemotherapy maintained high R0 resection rates across groups and demonstrated no significant difference in postoperative complications. 22 R0 resection rates in both groups were high, suggesting that age did not impair complete tumor clearance, consistent with propensity score-matched studies showing higher pCR rates and improved survival with nICT than with chemotherapy alone, without increased treatment-related adverse events (TRAEs).23,24 Collectively, these findings support the perioperative safety of nICT in elderly patients with ESCC and suggest that chronological age alone should not be considered a contraindication when comprehensive preoperative assessment and optimization are performed.
Regarding secondary outcomes, pCR, MPR, ypT/ypN stage, and TRG were comparable between elderly and non-elderly patients, indicating similar pathological responses and downstaging effects of nICT across age groups. These findings align with those of previous reports in mixed-aged ESCC populations, where pCR and MPR rates following nICT have been favorable and not been significantly influenced by age. In the KEYNOTE-001 study, the combination of pembrolizumab and chemotherapy achieved a pCR rate of 41.4% and an MPR rate of 72.4%, with no reported severe adverse events. 25 However, elderly patients are frequently underrepresented in clinical studies, resulting in limited data on such outcomes in this group. Our study demonstrated that elderly patients achieved comparable esophageal pCR rates to non-elderly patients following nICT with PD-1/PD-L1 inhibitors. These findings align with those of previous research. A study by Bai et al. 26 found that overall treatment tolerance was favorable among elderly patients receiving PD-1 inhibitors, and both survival and quality of life were improved, demonstrating a certain level of safety. Meredith et al. 27 reported that the pathological response following neoadjuvant therapy is a key determinant of survival in patients with esophageal cancer. Patients who achieve complete pathological response following neoadjuvant therapy exhibit higher R0 resection rates, lower recurrence rates, and improved 5-year overall and disease-free survival rates. Although research specifically investigating the efficacy of nICT in elderly patients with ESCC remains limited, evidence from studies on other malignancies supports adopting more aggressive treatment approaches in elderly patients. For instance, Yang et al. 28 demonstrated that elderly patients diagnosed with nasopharyngeal carcinoma, when appropriately selected, can effectively tolerate radical treatment regimens such as intensity-modulated radiotherapy, achieving improved overall survival and cancer-specific survival. These findings align with those of our study, indicating that elderly patients with locally advanced ESCC can safely undergo nICT and surgery. Therefore, individualized evaluation, rather than age alone, should guide therapeutic decision-making in elderly patients.
Postoperative complications remain a significant concern in elderly patients with cancer, largely due to age-related decline in immune, pulmonary, and cardiovascular functions, increasing the risk of pulmonary complications, infections, and anastomotic leakage.29,30 Such complications have been demonstrated to negatively impact long-term survival outcomes. 31 Our findings revealed no significant differences in postoperative complications between elderly and non-elderly patients. Consistent with our results, a real-world multicenter retrospective study reported a TRAE incidence of 53.8%, with the vast majority being grade 1–2; only 13.2% being grade 3–4; and 1.4%.being grade 5 32 In our study, elderly patients exhibited pathological outcomes, including pCR, MPR, ypT/ypN staging, and TRG, comparable to those of non-elderly patients following nICT, suggesting that age alone does not worsen the treatment outcomes. Limited studies have directly compared the pathological response between elderly and non-elderly populations receiving nICT. Most existing studies have either focused on general ESCC populations or compared different neoadjuvant strategies without age stratification. For example, a recent large-scale real-world study by Xu et al. 33 reported pCR and MPR rates of 29.8% and 53.6% following nICT, respectively, supporting its overall efficacy in ESCC; however, age-specific analyses were not provided. Similarly, although Shen et al. 34 highlighted the prognostic importance of achieving pCR in ESCC following nCRT (5-year overall survival: 79.3% in pCR vs. 54.8% in non-pCR, P = 0.001), the applicability of these findings to nICT and elderly cohorts remains uncertain. Given this gap, our study provides novel insights by demonstrating that elderly patients, when carefully selected, can achieve short-term pathological responses from nICT similar to younger patients, underscoring the need for individualized, not age-restricted, treatment decisions.
However, the incidence of postoperative pulmonary complications was slightly higher in the elderly group in this study, which may be closely related to the long-term smoking history, as smoking not only impairs postoperative pulmonary function recovery but also increases the risks of anastomotic leakage and infection. 35 Research has shown that prolonged smoking cessation before surgery can significantly reduce postoperative complications. In a randomized controlled trial, the observed relative risk reduction reached 41%, with smoking cessation for at least 4 weeks being strongly associated with a lower incidence of respiratory complications. 36 Furthermore, for each additional week of smoking cessation, the risk of postoperative complications was further reduced. 37 In the present study, no significant differences were observed between the elderly and non-elderly groups regarding operative time, intraoperative blood loss, number of lymph nodes dissected, length of hospital stay, surgical approach, proportion of minimally invasive McKeown procedures, ICU admission rates, or unplanned reoperation rates.
Complication rates for anastomotic leakage, recurrent laryngeal nerve palsy, and wound complications were comparable between elderly and non-elderly patients. These findings are consistent with those of large nationwide Finnish studies, which reported anastomotic leakage rates of 10%–14%. 38 Recurrent laryngeal nerve palsy rates were similar to those stated in most contemporary reports; however, an analysis using inverse probability weighting found higher rates in the nICT group than in the conventional therapy group. 39 The absence of significant age-related differences aligns with prior evidence that, in appropriately selected elderly patients, major complication rates are comparable to those in younger or less comorbid cohorts14,15 as well as with a prospective cohort study in esophageal cancer demonstrating no association between preoperative functional status and postoperative complication rates. 40
Limitations
This study has certain limitations. First, the retrospective design and relatively small sample size, particularly in the elderly group, might limit statistical power and generalizability. No formal power analysis was performed, and given the limited sample size, the study may not be sufficiently powered to detect small but clinically meaningful differences. Second, patients who could not undergo surgery due to disease progression were not included, introducing potential selection bias. Third, multiple ICIs were used, and potential differences in the therapeutic efficacy among these agents warrant further investigation. Finally, the relatively short follow-up period limited our ability to fully evaluate the long-term survival benefits and quality-of-life outcomes associated with nICT in elderly patients with ESCC.
Conclusion
This study found no differences in 30-day mortality, 90-day mortality, 30-day readmission rate, or R0 resection rates between elderly and non-elderly patients with locally advanced ESCC. Secondary outcomes, including pCR, MPR, ypT/ypN stage, TRG, and postoperative complications, were also comparable between groups. These findings suggest that, in appropriately selected patients, advanced age alone should not be considered a contraindication to nICT followed by surgery. Treatment decisions should be guided by comprehensive assessments of individual physiological status and overall clinical condition.
Footnotes
Acknowledgments
Not applicable.
Authors’ contributions
JiaJun Gao and JinXian He conducted the studies, participated in data collection, and drafted the manuscript. LiJie Wang and WeiYu Shen performed the statistical analysis and were involved in its design. All authors (JiaJun Gao, JinXian He, LiJie Wang, and WeiYu Shen) participated in the acquisition, analysis, or interpretation of data and drafted the manuscript. All authors have read and approved the final manuscript.
Consent to participate
The requirement for informed consent was waived by the Ethics Committee of the Affiliated Li Huili Hospital of Ningbo University owing to the retrospective nature of the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Consent for publication
Not applicable.
Data availability
All data generated or analyzed during this study are included in the published article.
Declaration of conflicting interest
The authors declare that they have no competing interests.
Ethical considerations
The study was approved by the Ethics Committee of the Affiliated Li Huili Hospital of Ningbo University (KY2019PJ058).
Funding
This study was supported by the following grants:
Ningbo Clinical Research Center for Thoracic Malignant Tumors (Project No. 2021L002).
Ningbo Key Medical Discipline Project (Project No. 2022-F02).
Zhejiang Provincial Clinical Key Specialty Construction Project (Department of Thoracic Surgery).