
Abstract
Sternocleidomastoid muscle injury is a rare traumatic lesion of the neck that may mimic several severe emergent conditions. Additionally, it can result in a significant hematoma that compresses vital structures. We herein report the case of a 27-year-old male patient who presented with sudden-onset neck pain following exercise. Ultrasound revealed a linear anechogenic area within the enlarged, relatively heterogeneous, and hyperechogenic left sternocleidomastoid muscle, with a hematoma originating from the muscle and herniating through a disrupted fascia. Contrast-enhanced computed tomography demonstrated a protruding cystic lesion from the enlarged sternocleidomastoid muscle, consistent with a hematoma. The hematoma was mild and did not compress the neighboring structures; therefore, the patient was managed conservatively with analgesics and motion restriction. Awareness regarding the radiological findings of the sternocleidomastoid muscle is essential for ruling out several emergent conditions and determining the extent of the hematoma.
Introduction
The sternocleidomastoid muscle (SCM) is a two-headed, powerful muscle that extends caudocranially from the sternum/clavicle to the temporal/occipital bones at the superficial anterolateral portions of the neck. The functions of the muscle in unilateral contraction are ipsilateral neck flexion and contralateral neck rotation, whereas those in bilateral contraction are neck/head extension and elevation of the sternum/clavicle. 1 It is a relatively thick and strong muscle; therefore, significant injury is rarely observed. Radiological findings of the muscle include hematoma, tear, and rupture, which may be easily detected on ultrasound. 2
In this report, we presented the case of a male patient with a unilateral SCM tear, rupture, and hematoma following exercise.
Case description
A 27-year-old male patient presented to the emergency department of Yuzuncu Yıl University Faculty of Medicine with left neck pain spreading to the left retroauricular region and medial supraclavicular area, which worsened with neck movements. He reported sudden onset of pain 6 h ago following a forced right rotation of the neck during exercise. He denied any history of blunt or penetrating trauma. On physical examination, all neck movements, particularly left rotation and flexion of the neck, were painful. Mild swelling was observed at levels III and IVB of the left neck. His laboratory examination was unremarkable, and he had no medication history. His vital parameters were within normal limits, with a heart rate of 92 beats/min, respiratory rate of 12 breaths/min, body temperature of 37.4°C, and blood pressure of 120/75 mmHg. A posteroanterior (PA) chest roentgenogram revealed asymmetric opacification in the left neck compatible with soft tissue swelling and a mild, right-sided tracheal deviation (Figure 1). Gray-mode and Doppler ultrasound of the neck revealed an enlarged left SCM with a heterogeneous, hyperechogenic fiber architecture compared with the normal right side—findings compatible with a sprain. Additionally, a cystic area compatible with a tear at the medial part of muscle and a rupture protruding through a neighboring fascial defect were observed. (Figure 2). An enlarged and heterogeneous SCM and a protruding cystic lesion compatible with a hematoma arising from the muscle, mildly compressing the left carotid artery, were observed on contrast-enhanced neck computed tomography (CT) (Figure 3). Based on clinical and radiological findings, the patient was diagnosed with a left SCM hematoma and rupture. He was managed conservatively using analgesics and neck-motion restriction. At 15 days after admission, a follow-up contrast-enhanced magnetic resonance imaging of the neck was planned; however, the patient declined the procedure because of complete clinical improvement.

A PA chest X-ray shows soft tissue swelling in the left neck (Long arrows (⇦)) and a mild right-sided tracheal deviation (Short arrow (➭)). PA: posteroanterior.
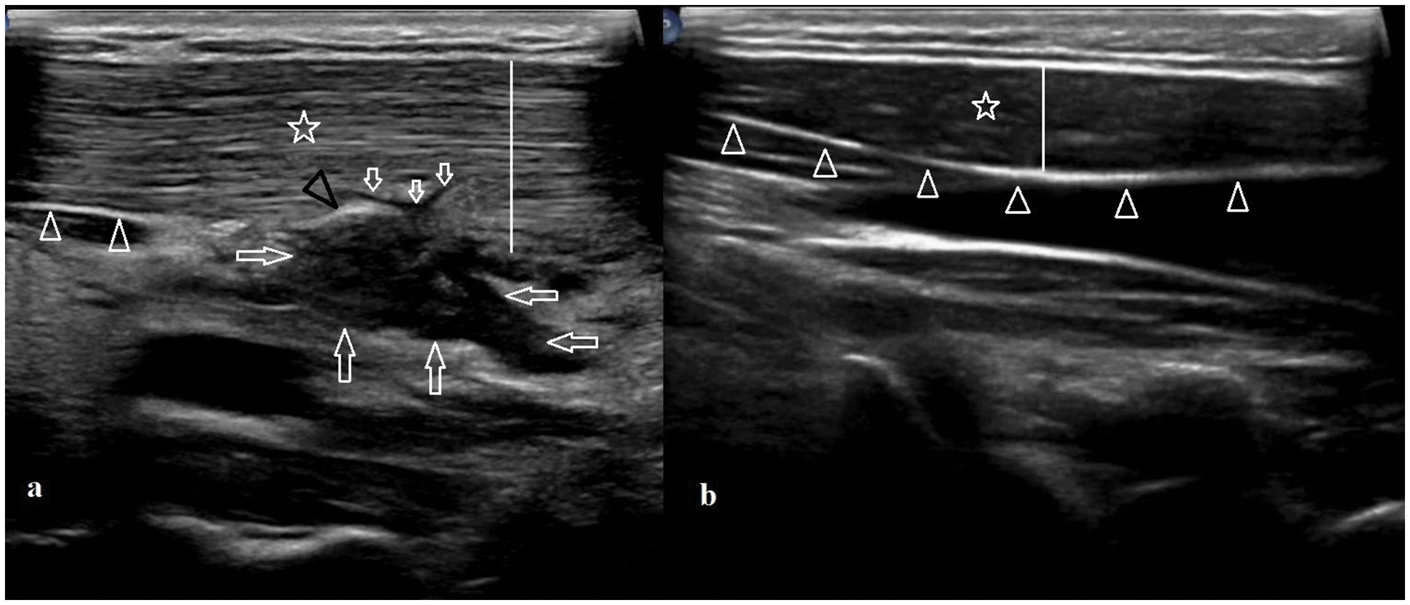
Gray-mode ultrasound of the neck demonstrates an (a) enlarged (lines (|)) and relatively heterogeneous hyperechogenic left SCM (star (⋆)) compared with (b) the normal right side at the same level (star (⋆)). The fascial continuity of the whole right SCM is visible, whereas the fascia is intact only in a small caudal portion on the left side (arrowheads (△)). A linear-shaped fluid collection in visible in the posterior part of the left SCM, which is compatible with a tear (small arrows (➭)). A heterogeneous, hypoechogenic hematoma which arose from the tear site and herniated through the disrupted fascia of the muscle (long arrows (⇦)) is visible. Furthermore, a thickened and irregular portion of the fascia that compressed and displaced by the hematoma near the rupture site is observed (black arrowhead (▶)). SCM: sternocleidomastoid muscle.

(a) Axial and (b) coronal reformatted CT images of the neck show the bilateral SCM (stars (⋆)). Note enlarged and relatively heterogeneous hypodense left SCM with a ruptured hematoma (arrows (⇦)) compared with the normal right side. CT: computed tomography; SCM: sternocleidomastoid muscle.
Discussion
SCM tear and rupture are rare conditions and have been reported secondary to penetrating trauma, 3 difficult labor, 4 lifting weights, 5 epileptic seizure, 6 and motor vehicle accident. 7 The most common complications of SCM hematoma are torticollis and neck pain.4,8 Although it is usually a self-limited entity that does not require aggressive intervention, there are two important considerations. First, the condition may mimic various acute, emergent, life-threatening, or severe chronic events. In cases of such acute neck pain and swelling, vascular pathologies such as jugular–subclavian vein thrombosis, carotid/subclavian artery thrombosis, aneurysms/pseudoaneurysms, and dissections must be first ruled out. Lack of thrombosis, dilatation, and flap formation in the lumen help rule out these vascular pathologies. Contrast-enhanced CT images may be particularly useful in cases of bleeding of a vascular malformation. An abscess typically has a thick, enhancing wall and demonstrates diffusion restriction on diffusion-weighted magnetic resonance images. Malignant or atypical lymphadenopathies demonstrate characteristic ultrasound features, including spherical geometry without echogenic fatty hilum. 9 Second, an extensive muscular hematoma in the neck may compress vital structures such as the carotid artery, jugular vein, vagal nerve, cervical plexus, and trachea, potentially disturbing the blood flow in the central nervous system and causing mediastinal shift. Therefore, accurate and prompt diagnosis of SCM rupture as well as regular follow-up of the lesion are essential. Serial ultrasound scans allow optimal comparison between the initial and follow-up lesion sizes and help determine the extent of hematoma.
Hematoma, rupture, intramuscular fluid, or fascial disruption usually accompany muscular injuries. Hematomas typically appear as hypoechogenic or hyperechogenic (depending on the age of the hematoma), nonvascular areas within or near the muscle on ultrasound. Rupture is identified when a hematoma or a portion of fibers herniates through the damaged region of the fascia surrounding the muscle. Intact fascia appears as a homogeneous, continuous linear band of thin hyperechogenic structures. An irregularity or discontinuity in the fascia suggests injury/rupture. 2 In rare cases, it is challenging to detect a mild or moderate muscle injury, including hematoma, tear, and rupture, in the absence of radiological findings. In addition, the injury may be misidentified as a normal muscle structure when pathological SCM is solely evaluated. However, when the muscles of both sides are compared, particularly using a dual, split-screen menu, differences in their thickness and echogenicity can be easily noticed. Especially, grade 1 strains may appear as general areas with increased echogenicity, without a hematoma, tear, or rupture. 2 Similarly, in our case, the left SCM exhibited diffuse but homogeneously increased echogenicity compared with the intact right side. A neck magnetic resonance imaging would have been particularly helpful; however, the patient declined the examination because of claustrophobia.
SCM hematoma management remains controversial because large hematomas sometimes warrant surgical resection; whereas, in most cases, a conservative approach is preferable.4,5 Although this entity is usually self-limited; the extent and size of the hematoma must be closely monitored. 4 Nonsteroidal anti-inflammatory drugs are generally used in these cases.4,5,7 However, in cases with evidence of infection, antibiotics are added to the medical treatment regimen. 5 Physical therapy and muscle relaxants are used for mild or moderate torticollis secondary to SCM hematomas. 8
Consistent with most previous reports, our patient did not require surgical drainage or excision. His symptoms resolved spontaneously following the administration of oral analgesics. Furthermore, complications such as infection and torticollis were not observed, which have been reported in previous studies.4,8
Radiological findings of our case were similar to those reported previously, including anechoic/hypodense cystic hematomas arising from the SCM and perimuscular edema. However, two findings of our case may add new information to the existing literature on this topic. First, an enlarged and heterogeneous muscle compared with the contralateral side is highly suggestive of muscular injury, which was well demonstrated, particularly on ultrasound images. Second, discontinuity of the fascia is a very important but relatively less-known indicator of rupture. When evaluating a muscle for injury, the fascial structures surrounding muscles must also be examined in detail.
Conclusion
SCM rupture/hematomas must be considered in the differential diagnosis of patients who present with acute neck pain and swelling following a trauma or exercise. Comparison of the affected side with the contralateral symmetrical structures at the same level using ultrasound is essential for detecting mild musculotendinous injuries.
Footnotes
Acknowledgments
None.
Data availability statement
The data associated with this report are available from the corresponding author upon reasonable request.
Declaration of the reporting guidelines
Informed consent was obtained from the patient for this report. All patient details were de-identified. The reporting of this study conforms to the Case Report (CARE) guidelines. 10
Declaration of conflicting interests
There are no conflicts of interest.
Funding
No funding or financial support was received for this report.