
Abstract
Objective
Robot-assisted partial nephrectomy is increasingly being performed; however, its benefits compared with those of laparoscopic partial nephrectomy remain controversial. This study aimed to compare the differences between robot-assisted partial nephrectomy and laparoscopic partial nephrectomy in the treatment of renal tumors.
Methods
A retrospective analysis was conducted on 74 patients who underwent partial nephrectomy between January 2022 and February 2024. Of these, 68 patients with a postoperative pathological diagnosis of renal cell carcinoma and complete clinical data were included. Clinical, perioperative, and follow-up data were collected to compare the therapeutic outcomes between the robot-assisted partial nephrectomy and laparoscopic partial nephrectomy groups.
Results
The average warm ischemia time was significantly shorter in the robot-assisted partial nephrectomy group (18.80 ± 3.49 vs. 21.02 ± 3.68 min, p = 0.044), with lesser intraoperative blood loss (15.47 ± 6.91 vs. 74.06 ± 112.60 mL, p = 0.049). The positive surgical margin rates in the robot-assisted partial nephrectomy and laparoscopic partial nephrectomy groups were 0% and 1.89%, respectively, with no significant difference (p = 0.592). No patients experienced complications greater than Clavien–Dindo grade III.
Conclusion
Compared with laparoscopic partial nephrectomy, robot-assisted partial nephrectomy for renal tumors results in a shorter warm ischemia time and reduced intraoperative blood loss.
Introduction
Renal cell carcinoma (RCC) is the most common type of kidney cancer, and its incidence is increasing globally. The incidence of RCC varies across regions, with higher rates reported in Europe and North America than in other areas.1–3 The surgical approach for clinical T1 RCC has transitioned from radical nephrectomy to partial nephrectomy to preserve renal function.4,5
With the development of minimally invasive techniques, laparoscopic partial nephrectomy (LPN) and robot-assisted partial nephrectomy (RAPN) have become more common in clinical practice.6–8 These procedures typically result in smaller incisions, reduced blood loss, decreased postoperative pain, and shorter hospital stays. 9 The precision provided by robotic assistance can enhance the surgeon’s ability to perform delicate dissection and reconstruction, potentially preserving more healthy renal tissue and maintaining better overall renal function. Additionally, technological advancements in these surgical approaches contribute to improved visibility of the surgical field, facilitating more precise and controlled resection of renal tumors.10–12 This is particularly advantageous in complex cases where the tumor location and patient anatomy present challenges. Based on this background, we aimed to report our experience in a series of minimally invasive partial nephrectomy procedures, including laparoscopic and robotic surgeries, and compare the intraoperative and postoperative outcomes between the two techniques.
In previous studies, comparisons of clinical outcomes between LPN and RAPN have primarily focused on procedures performed using the da Vinci robotic system.13–18 However, with the advancement of robotic surgical systems, several other systems have been introduced in clinical practice.19,20 The KangDuo system, an emerging robotic surgical platform, is currently being explored for clinical applications across various fields, including urology and general surgery.21,22 This study compared the application and safety of the KangDuo robotic surgical system versus laparoscopy in partial nephrectomy, aiming to provide references to support its clinical application in this surgical procedure.
Materials and methods
Study design and patient population
A total of 74 patients underwent partial nephrectomy at Peking University First Hospital-Miyun Hospital from January 2022 to February 2024. Of these, 68 patients had postoperative pathological findings of RCC and complete clinical data. Among them, 53 patients underwent LPN and 15 underwent RAPN (Figure 1). Clinical data of the patients were collected, including general clinical data, perioperative data, and postoperative complications. The surgeries were performed by a single surgeon, who had more than 20 years of surgical experience and expertise in urinary system tumor surgeries. This study contains no information that can identify patients.
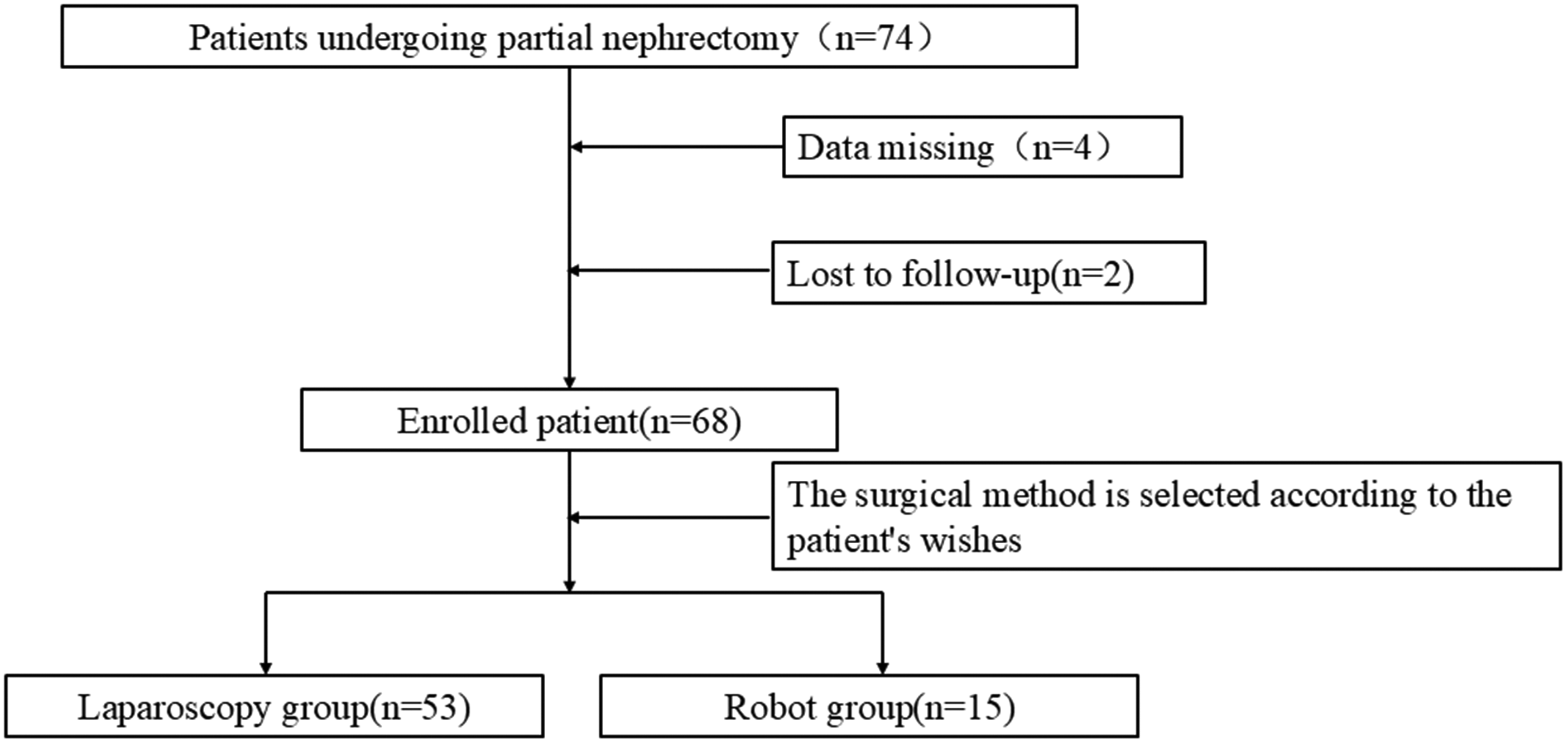
Study flow chart.
This study primarily compared the clinical outcomes of laparoscopic and robot-assisted laparoscopic surgeries. The evaluation was conducted through three indicators, namely, the incidence of positive surgical pathological margins, intraoperative warm ischemia time, and occurrence of complications with a Clavien–Dindo grade of >III. A positive surgical pathological margin after surgery indicates that the resection margin of the excised renal tissue contains tumor cells, as confirmed by pathological examination. The warm ischemia time refers to the time from the start of blocking the renal blood flow to the restoration of blood flow. Complications are classified according to the Clavien–Dindo grading system. 23 The intraoperative blood loss was estimated by the surgeon and anesthesiologist based on the surgical field, degree of blood staining on the gauze, and color and volume of the liquid in the suction apparatus.
Inclusion criteria were as follows: (a) age ≥18 years; (b) presence of single tumor; (c) history of partial nephrectomy; (d) diagnosis of cT1a-b nonmetastatic renal tumors; and (e) availability of complete clinical data. Exclusion criteria included the following: (a) patients with abnormal coagulation function; (b) patients with cardiopulmonary dysfunction who cannot tolerate surgery; and (c) pregnant women.
This study was conducted in accordance with the principles of the Declaration of Helsinki (revised in 2013) and approved by the Ethics Committee of Peking University First Hospital-Miyun Hospital. The need for informed consent was waived because of the retrospective nature of this study.
Surgical technique
The KangDuo robotic surgical system was used in this study. The patient was placed in a 60° oblique position on the healthy side, and routine disinfection and draping were performed. A small incision, 1 cm below the costal margin along the midclavicular line on the affected side, was made to insert a pneumoperitoneum needle and trocar to place Robot arm 1. A trocar was inserted through a puncture at the outer edge of the rectus abdominis muscle on the affected side, 3 cm above the umbilicus, for the placement of the camera. Another trocar was inserted 3 cm below the umbilicus, at the outer edge of the rectus abdominis muscle on the affected side, to introduce Robot arm 2. The ureter was dissected free at the lower pole of the affected kidney. Dissection was performed along the gonadal vein toward the renal pedicle of the affected kidney to expose the renal artery and vein. The renal tumor was fully dissected free (Figure 2(a)). The renal artery of the affected kidney was blocked with a “bulldog” clamp (Figure 2(b)). The boundary was drawn along the edge of the tumor, 0.5 cm away from the tumor, and the tumor was completely resected by cutting along the edge toward the depth with scissors (Figure 2(c)). The wound surface of the affected kidney was sutured with absorbable sutures (Figure 2(d)).

Surgical steps of robotic partial nephrectomy. (a) Mobilization of the kidney; (b) clamping of the renal artery; (c) resection of the renal tumor; and (d) suturing of the kidney.
Statistical analysis
Excel software (version 2019) was used for data management, and Statistical Package for Social Sciences (SPSS version 27.0) software was used for statistical analysis. Normality tests were performed using the Shapiro–Wilk test (for sample sizes <50) and Kolmogorov–Smirnov test (for sample sizes ≥50). Measurement data conforming to a normal distribution were expressed as mean ± SD, whereas data with a skewed distribution were presented as median (range). For continuous variables, the t-test was used to analyze the variables conforming to a normal distribution, and the Mann–Whitney U test was used to analyze the variables that did not conform to a normal distribution. The chi-square test and Fisher’s exact probability test were used to analyze categorical variables.
Postoperative management and follow-up
The abdominal drainage tube and transurethral catheter were removed, and the patients were discharged from the hospital between postoperative days 2 and 7. Patients were advised to undergo computed tomography (CT) once a year for 2 years after the operation. Regular evaluations, particularly during the initial years, help detect potential complications and improve the long-term survival. 24 The follow-up assessment included the occurrence of complications within 1 year after the operation and recurrence of the disease thereafter.
Results
Patient baseline data
All patients successfully underwent surgery without conversion to open surgery. The average age of the patients was 52.84 ± 12.75 years. The average warm ischemia time during the operation was 20.53 ± 3.75 min, and the average intraoperative blood loss was 61.13 ± 102.38 mL. Among the cases, one had a positive pathological margin. The overall incidence rate of Clavien–Dindo grade I complications (fever) was 8.8% (6/68), with 7.55% (4/53) in the LPN group and 13.33% (2/15) in the RAPN group. The overall incidence rate of Clavien–Dindo grade II complications (infection) was 5.89% (4/68), with 5.66% (3/53) in the LPN group and 6.67% (1/15) in the RAPN group. There were no complications of Clavien–Dindo grade ≥III.
Comparison of the clinical outcomes of LPN and RAPN
The baseline data and preoperative clinical data of the patients in the LPN and RAPN groups are shown in Table 1. The average tumor sizes in the LPN and RAPN groups were 3.43 ± 1.66 and 3.00 ± 1.42 cm, respectively, with no statistically significant difference between the two groups (p = 0.367). The average renal scores in the LPN and RAPN groups were 5.09 ± 1.52 and 4.87 ± 1.45, respectively, exhibiting no statistically significant difference between the two groups (p = 0.612).
Comparison of the preoperative data between the LPN and RAPN groups.
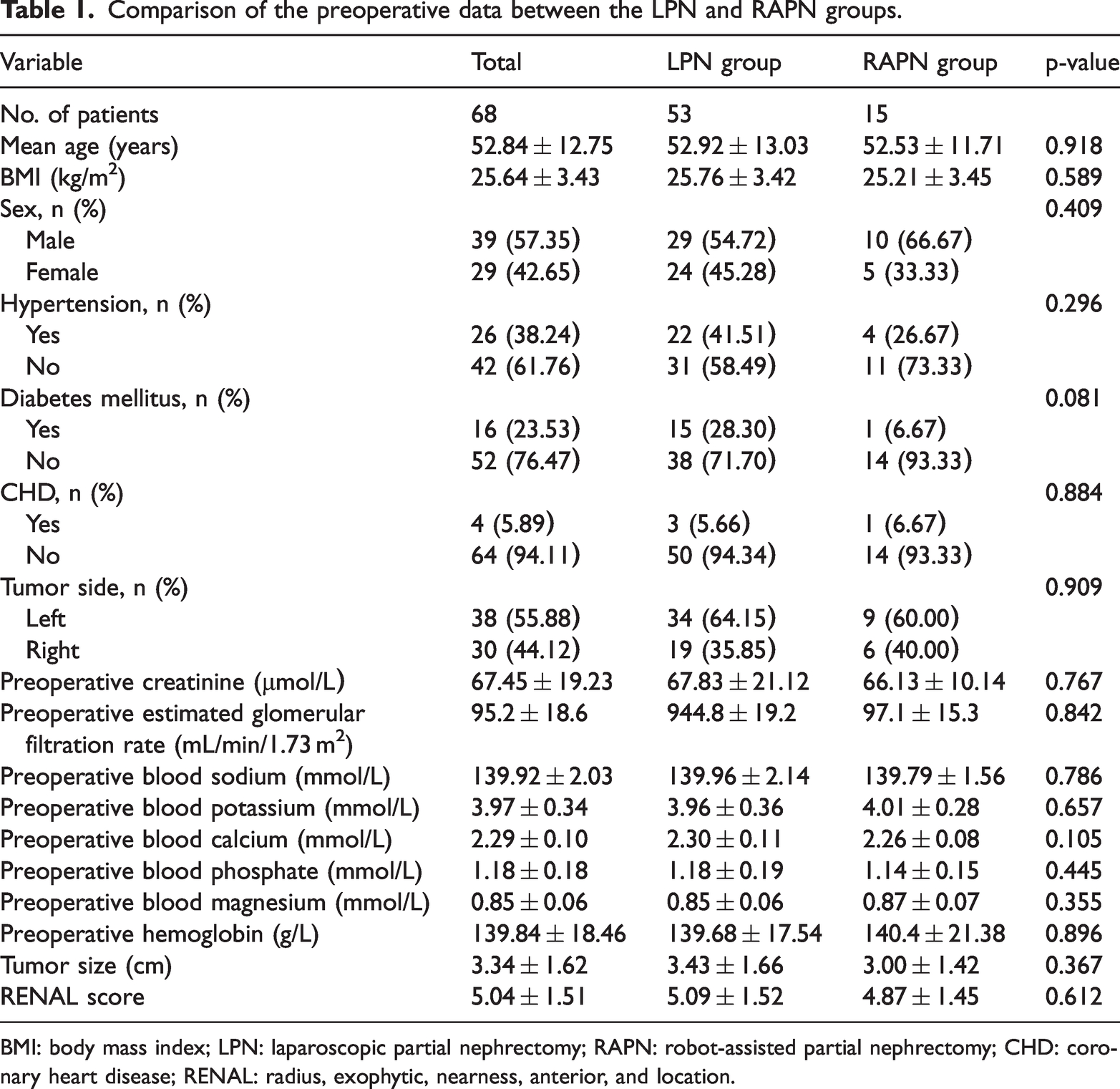
BMI: body mass index; LPN: laparoscopic partial nephrectomy; RAPN: robot-assisted partial nephrectomy; CHD: coronary heart disease; RENAL: radius, exophytic, nearness, anterior, and location.
The intraoperative and postoperative clinical data of the patients in the LPN and RAPN groups are presented in Table 2. The average warm ischemia time was 21.02 ± 3.68 min in the LPN group and 18.80 ± 3.49 min in the RAPN group, with a statistically significant difference between the two groups (p = 0.044). The average intraoperative blood loss was 74.06 ± 112.60 mL in the LPN group and 15.47 ± 6.91 mL in the RAPN group, showing a statistically significant difference between the two groups (p = 0.049). The positive margin rate was 1.89% (1/53) in the LPN group and 0% (0/15) in the RAPN group, exhibiting no statistically significant difference between the two groups (p = 0.592). There were no statistically significant differences in the postoperative hospital stay (p = 0.515), operative time (p = 0.744), postoperative creatinine level (p = 0.665), postoperative positive margin rate (p = 0.592), and postoperative hemoglobin level (p = 0.773) between the two groups.
Comparison of the intraoperative and postoperative data between the LPN and RAPN groups.
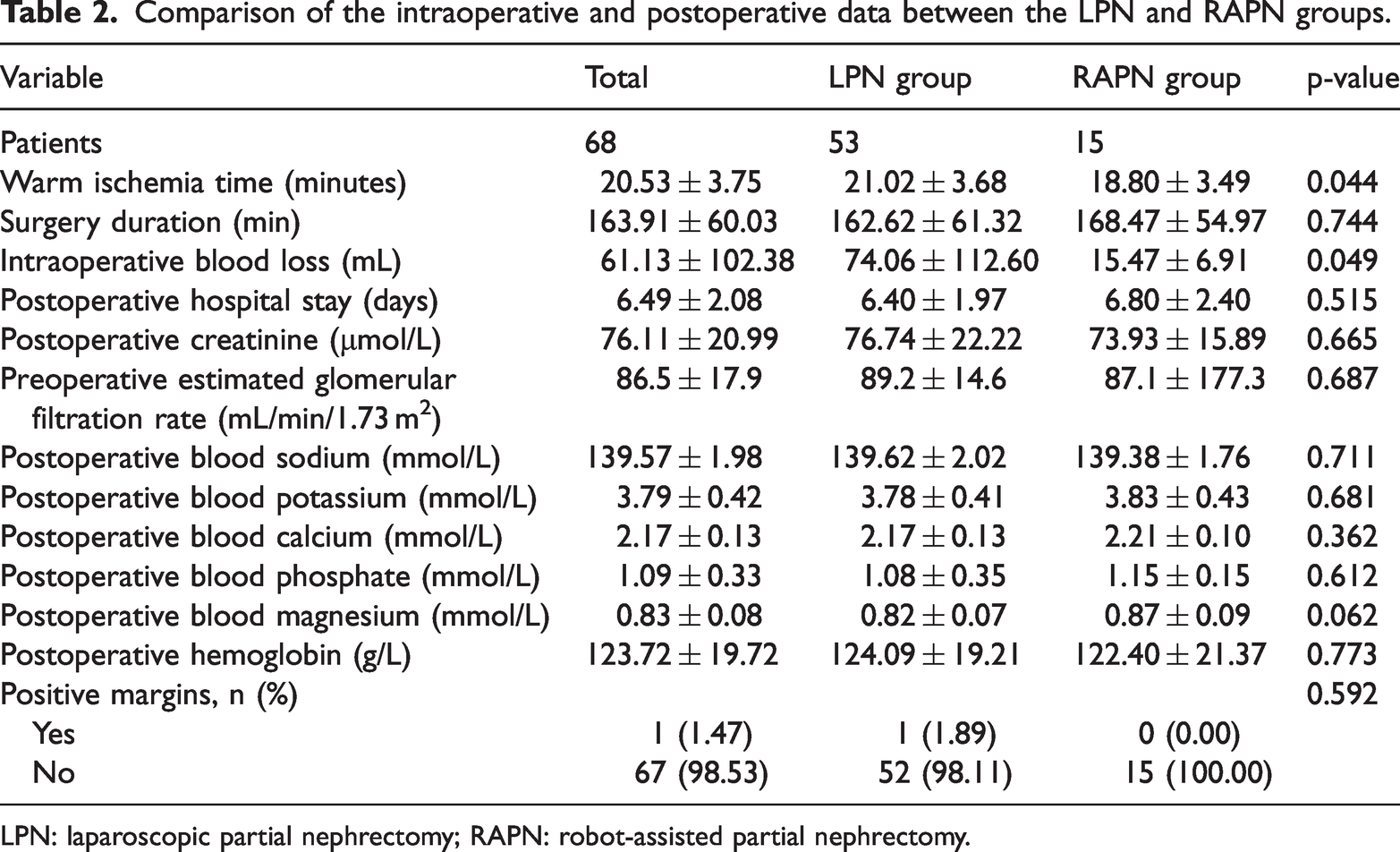
LPN: laparoscopic partial nephrectomy; RAPN: robot-assisted partial nephrectomy.
Discussion
With the recent development of minimally invasive surgical techniques, partial nephrectomy has become the preferred treatment method for stage T1 RCC. Compared with traditional radical nephrectomy, partial nephrectomy can maximize the preservation of healthy renal tissue, thereby contributing to the long-term protection of patients’ renal function. Maintaining the integrity of renal function can not only reduce the incidence of chronic kidney disease but also effectively prevent cardiovascular diseases associated with renal failure. Furthermore, the protection of renal function may delay the progression of end-stage renal disease and reduce the patients’ dependence on hemodialysis, thereby improving the quality of life and reducing treatment costs.25–27
Several studies have compared RAPN and LPN. Although RAPN is considered to provide better outcomes, the specific variables in which it is superior to conventional LPN vary across studies.12,13,28,29 In the present study, the main finding is that RAPN offers advantages over LPN in terms of intraoperative blood loss and average warm ischemia time. Hinata et al. 30 consistently reported that RAPN had a shorter warm ischemia time than LPN. Reducing the warm ischemia time helps protect the renal tubules and the tubulointerstitium, reducing the risk of acute kidney injury and maintaining renal function. A shorter warm ischemia time facilitates better recovery of the microvascular structure and renal tubule function of the kidney, thereby reducing the postoperative recovery period and improving the patients’ quality of life. The lower intraoperative blood loss in RAPN compared with that in LPN may be attributed to the more precise operational control of the robotic surgical system. The KangDuo surgical robotic system, with its comprehensive advantages, including three-dimensional vision, tremor-filtering technology, flexible instruments, and operational comfort, enables more accurate anatomical dissection as well as more efficient hemostasis and suturing, thereby reducing intraoperative blood loss. Lesser blood loss refers to reduced blood loss during and after the operation, which lowers the occurrence of complications, such as shock, anemia, and cardiovascular events. Excessive bleeding may lead to insufficient renal perfusion, affecting normal kidney function. Reducing intraoperative bleeding helps maintain the blood flow and oxygen supply to the kidneys, thereby lowering the risk of postoperative impairment of renal function. Therefore, in this study, RAPN is believed to indirectly reduce the damage to renal function more effectively than LPN.
In partial nephrectomy, the status of the surgical margin, occurrence of complications with Clavien–Dindo grade ≥III, and occurrence of a decrease in estimated glomerular filtration rate ≤30% may be the most concerned focuses. In this study, the positive margin rate was 1.89% (1/53) in the LPN group and 0% (0/15) in the RAPN group. Although there was no statistically significant difference between the two groups (p = 0.592), RAPN exhibited an advantage over LPN in terms of the positive surgical margin rate, which may be related to the more precise and stable operation of RAPN. The two-dimensional planar visual field of LPN is inferior in terms of in-depth perception and detail presentation. This limitation may lead to deviations in judging the resection range, particularly for small, deeply located tumors (such as those within the renal parenchyma or adjacent to the renal sinus) or tumors with indistinct boundaries (such as hypovascular tumors), thereby increasing the risk of a residual positive margin. Traditional laparoscopic instruments used in LPN have only four degrees of freedom, limiting their operational flexibility in complex anatomical locations (such as around the renal calyces or in vascular-rich areas). This limitation may force surgeons to reduce the resection range because of the difficulty of “proper instrument positioning,” thereby increasing the risk of positive surgical margins. Bic et al. 31 reported that RAPN had a lower complication rate than LPN; however, in the present study, neither RAPN nor LPN resulted in complications of Clavien–Dindo grade ≥III. The preoperative creatinine level was 67.83 ± 21.12 μmol/L in patients who underwent LPN, and the postoperative level was 76.74 ± 22.22 μmol/L. The preoperative creatinine level was 66.13 ± 10.14 μmol/L in patients who underwent RAPN, and the postoperative level was 73.93 ± 15.89 μmol/L. The decline in renal function in both groups was ≤30%.
In the study by Liu et al., 32 among 128 patients, the abdominal drainage time was 4.53 ± 0.98 days for RAPN and 5.42 ± 2.71 days for LPN (p = 0.029). The postoperative hospital stay was 5.72 ± 1.23 days for RAPN and 8.22 ± 4.64 days for LPN (p < 0.001). Compared with LPN, RAPN demonstrated significant advantages in terms of the placement time of abdominal drainage and postoperative hospital stay. In the present study, the postoperative hospital stays for RAPN and LPN were 6.80 ± 2.40 days and 6.40 ± 1.97 days, respectively, with no significant difference between the two groups (p = 0.515).
Only a few studies have suggested that LPN has a better clinical outcome than RAPN, and it offers certain economic advantages. However, as the da Vinci robot has passed the patent protection period, various robotic systems are currently in use, considerably reducing the cost of the surgery. The KangDuo robotic system used in this study demonstrated no obvious difference in surgical outcomes compared with the da Vinci robot.22,33,34 With the application of more robotic systems, there is potential for further cost reduction in the future.
This study has certain limitations. It is a retrospective, single-center study with a relatively small sample size, which may introduce certain biases. Additionally, the considerable difference in the sample size between the two groups further increases the possibility of bias. The follow-up period of this study was 1 year, and a longer follow-up period is needed to further evaluate the renal function and the occurrence of complications. Subsequent prospective cohort studies are necessary. Currently, retrospective studies can only provide limited data references for clinical practice and cannot serve as standards for guiding clinical work. Therefore, prospective cohort studies with a larger sample size and balanced patient numbers between the two groups can allow better intergroup comparisons and reduce the possibility of bias.
Conclusion
In our study, RAPN for the treatment of renal tumors has demonstrated a shorter warm ischemia time and lesser intraoperative blood loss compared with those in LPN. Additionally, RAPN exhibited certain advantages in terms of the positive surgical margin rate. In other aspects, such as operative time and postoperative complications, no significant differences were observed between the two approaches.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251390064 - Supplemental material for Comparison of therapeutic effects between transabdominal robot-assisted partial nephrectomy and laparoscopic partial nephrectomy
Supplemental material, sj-pdf-1-imr-10.1177_03000605251390064 for Comparison of therapeutic effects between transabdominal robot-assisted partial nephrectomy and laparoscopic partial nephrectomy by Chao Zuo, Zihui Gao and Yaming Gu in Journal of International Medical Research
Footnotes
Acknowledgment
None.
Author contributions
Conception and design: Chao Zuo and Yaming Gu Administrative support: Chao Zu and Yaming Gu Provision of study materials or patients: Chao Zuo, Zihui Gao, and Yaming Gu Collection and assembly of data: Chao Zuo Data analysis and interpretation: Chao Zuo Manuscript writing: All authors Final approval of manuscript: All authors
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
None declared.
Ethical approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The trial was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study was approved by the Ethics Committee of Peking University First Hospital-Miyun Hospital (No. 2023-01-007).
Funding
None.
Informed consent
Informed consent was waived due to the retrospective design of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.