
Abstract
Objective
This prospective study aimed to evaluate anterior segment parameters after neodymium-doped yttrium-aluminum-garnet laser posterior capsulotomy.
Methods
The central corneal thickness, anterior chamber depth, lens vault, and pupil diameter measurements were taken using the novel anterior segment swept-source optical coherence tomography system. The tilt of the intraocular lens was measured with the Optical Path Difference Scan III. The examinations were performed preoperatively and repeated at postoperative 30 min, 1 week, and 1 month. The patients were divided into two groups according to the type of lens used: C-loop–type (n = 18) and plate-type (n = 18) intraocular lens.
Results
The mean central corneal thickness (p < 0.001), anterior chamber depth (p < 0.001), and lens vault (p = 0.005) were increased significantly at 30 min and then returned to baseline values at 1 week and 1 month after the capsulotomy. Furthermore, the mean increase in the degree of anterior chamber depth and lens vault in the plate-type intraocular lens group was more than that in the C-loop–type intraocular lens group at postoperative 30 min; however, these increases were not significantly different (p > 0.05). The mean tilt of the intraocular lens values did not change significantly after capsulotomy in both groups.
Conclusion
Neodymium-doped yttrium-aluminum-garnet capsulotomy causes a temporary increase in the central corneal thickness, anterior chamber depth, and lens vault; however, it does not significantly alter the tilt of the intraocular lens.
Keywords
Introduction
After a period of successful cataract surgery, posterior capsular opacification (PCO) is one of the most vision-disturbing problems. Neodymium-doped yttrium-aluminum-garnet (Nd:YAG) laser capsulotomy has remained the optimal choice for the treatment of PCO in pseudophakic eyes for many years.1–3 Although it has fewer complications than surgical removal, Nd:YAG laser posterior capsulotomy has been associated with post-laser intraocular pressure rise, corneal injury, anterior hyaloid disruption, intraocular lens (IOL) damage or movement, cystoid macular edema, and refractive change.4,5 These complications are rare, and Nd:YAG laser capsulotomy is an economic, fast, non-invasive, and relatively easy procedure, resulting in its frequent use. The evaluation of changes in anterior segment parameters after Nd:YAG laser capsulotomy may provide important information about the mechanisms of complications and refraction changes.
Previous studies have addressed the change in anterior chamber parameters and IOL position following Nd:YAG treatment to report inconsistent results and relevant limitations.6–13 Some studies included a mixed group of patients who had undergone phacoemulsification surgery or extracapsular cataract extraction; some included a mixed group of patients treated with different shapes and sizes of Nd:YAG capsulotomy; some included eyes that had been implanted with different types of IOLs, and in others, the examination time points were relatively fewer, including only preoperative and one postoperative evaluation. In addition, different anterior segment analysis systems, because of their distinct sensitivities, may have caused variations in the results.
In the present study, we prospectively evaluated anterior chamber parameters, including central corneal thickness (CCT), anterior chamber depth (ACD) (excluding the cornea), ACD (including the cornea), lens vault, and tilt of IOL before and after Nd:YAG capsulotomy in patients with PCO after uneventful phacoemulsification cataract surgery and single-piece IOL implantation. Considering that the design of the IOLs (C-loop–type or plate-type) implanted in the capsular bag may play a significant role in anterior segment parameters after capsulotomy, this study clarifies the characteristics of the IOLs in the C-loop–type and plate-type IOL groups. To the best of our knowledge, this is the first study to evaluate the effect of different IOL types (C-loop or plate) on anterior segment parameters after Nd:YAG laser capsulotomy, as measured using the novel high-resolution anterior segment swept-source optical coherence tomography (SS-OCT) system.
Patients and methods
Study population
This prospective study was designed as a comparative study that included 36 pseudophakic eyes of 36 patients with visually significant PCO. All patients underwent Nd:YAG laser capsulotomy between September 2024 and January 2025 at our hospital. This study was conducted as per the ethical standards of the Declaration of Helsinki of 1975, as revised in 2024, and was approved by the institutional ethical committee of our hospital. All participants in this study provided written informed consent for study participation and data publication, and we have de-identified all patient details. All participants underwent an ophthalmic examination, including visual acuity assessment, slit-lamp biomicroscopy, air-puff tonometry, indirect retinoscopy, ocular ultrasound, and optical coherence tomography for macular evaluation. As per the exclusion criteria, patients who had undergone any ocular surgery other than uneventful phacoemulsification; had corneal pathology, corneal irregularities, history of glaucoma, uveitis, or posterior segment pathology, which effected the anterior segment dynamics, or contact lens use; those with high myopia (−6.00 diopter or worse) or microphthalmia (axial length <21 mm in adulthood); and those who were unable to understand the study were excluded. All the pseudophakic patients were divided into two groups according to the IOL type as follows: C-loop–type (n = 18) (acrylic hydrophobic, SA60AT, Alcon, Texas, USA, and acrylic hydrophobic, ZCB00, AMO, California, USA) and the plate-type (n = 18) (acrylic hydrophobic, 409MP, Carl Zeiss Meditec, Jena, Germany) IOL groups. A single surgeon performed all the cataract surgeries using the Infiniti Vision System (Alcon Laboratories). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14
Measurement techniques
The SS-OCT (Intalight, Henan, China) and Optical Path Difference Scan III (OPD-Scan III, NIDEC, Japan) measurements of the studied parameters were performed before, and 30 min, 1 week, and 1 month in dilated conditions after Nd:YAG laser capsulotomy. The SS-OCT and OPD-Scan III measurements were performed carefully three times by the same examiner, and the average values were used for statistical evaluations.
SS-OCT measurements
The SS-OCT system delivers detailed high-resolution images of the anterior segment along with accurate and reliable measurements of the anterior segment, which include the CCT, ACD (excluding the cornea), ACD (including the cornea), lens vault, pupil diameter, and some other anterior segment parameters, such as anterior chamber angle, lens thickness, anterior chamber volume, and white-to-white. The anterior segment images of a patient obtained before and after Nd:YAG laser capsulotomy using SS-OCT are shown in Figure 1, with the anterior segment parameters evaluated in this study marked. Measurements were performed while the device was brought into focus, and the participant’s eye was aligned to the central fixation light.

Anterior segment image of a patient obtained before and after Nd:YAG laser capsulotomy using SS-OCT. (a) Anterior segment image obtained before the Nd:YAG laser capsulotomy using SS-OCT and (b) anterior segment image obtained after the Nd:YAG laser capsulotomy using SS-OCT. SS-OCT: swept-source optical coherence tomography; Nd:YAG: neodymium-doped yttrium-aluminum-garnet.
OPD-Scan III measurements
The new-generation corneal topographer, the OPD-Scan III device, directly provides the tilt of IOL as data based on aberration calculations in the wavefront mode. Tilt values were used for evaluation as deviations at the intersections of the horizontal plane perpendicular to the axis of view of the eye and the constant position of the fixation point. 15 The anterior segment images of a patient obtained before and after Nd:YAG laser capsulotomy using OPD-Scan III are shown in Figure 2.

Anterior segment image of a patient obtained before and after the Nd:YAG laser capsulotomy using OPD-Scan III. (a) Anterior segment image obtained before the Nd:YAG laser capsulotomy using OPD-Scan III and (b) anterior segment image obtained after the Nd:YAG laser capsulotomy using OPD-Scan III. Nd:YAG: neodymium-doped yttrium-aluminum-garnet; OPD-Scan III: Optical Path Difference Scan III.
Operation technique
All Nd:YAG laser capsulotomies (Carl Zeiss Meditec, Jena, Germany) were performed by the same doctor. A contact lens with a coupling agent was applied to the eye to improve the focusing of the laser beam on the posterior capsule. The capsulotomy was performed in a circular pattern to create a diameter opening of at least a 4–4.5 mm. The laser energy range used was between 0.80 and 1.2 mJ, with a single pulse mode ranging between 18 and 56 shots. All patients were advised to use tobramycin dexamethasone eye drops four times daily for 1 week. There were no complications due to the capsulotomy procedure, and all patients' intraocular pressure was within the normal range.
Statistical analyses
Statistical Package for Social Sciences (SPSS) for Windows Version 27.0 (IBM Armonk, New York, USA) was used for statistical analyses. Analytical methods (Shapiro–Wilk tests) were used to assess whether the data were normally distributed. Normally distributed data were analyzed using paired samples t-test. Non-normally distributed data were evaluated using the Wilcoxon test. Data were expressed as mean ± SD. p < 0.05 was considered to be statistically significant.
Results
In total, 36 consecutive pseudophakic patients (21 women and 15 men) were included in this study. There were no complications due to the capsulotomy procedure, and all patients' intraocular pressure was within the normal range. The mean age of the patients was 70.0 ± 11.0 (45–93) years. The mean age was 70.6 ± 10.0 (48–85) years in the C-loop–type IOL group and 69.4 ± 12.2 (45–93) years in the plate-type IOL group, there was no significant difference in the age of the two groups (p = 0.75). The mean axial length was 23.51 ± 0.63 (22.3–24.5) mm in the C-loop–type IOL group and 23.54 ± 0.64 (22.5–24.6) mm in the plate-type IOL group, with no significant difference in the axial length between the two groups (p = 0.88). The mean diameter of Nd:YAG laser capsulotomy was 4.21 ± 0.11 (4.01–4.35) mm in the C-loop–type IOL group and 4.27 ± 0.12 (4.05–4.40) mm in the plate-type IOL group, with no significant difference in the diameter of Nd:YAG laser capsulotomy between the two groups (p = 0.16).
The mean values of anterior segment parameters, including the CCT, ACD (excluding the cornea), ACD (including the cornea), lens vault, pupil diameter, and tilt of IOL at baseline and at 30 min, 1 week, and 1 month after capsulotomy were summarized in Table 1. The mean CCT (p < 0.001), ACD (excluding the cornea) (p = 0.002), ACD (including the cornea) (p < 0.001), and lens vault (p = 0.005) values increased significantly at 30 min after the capsulotomy and returned to baseline levels at 1 week and 1 month postoperatively. In our study, the mean pupil diameter and tilt of IOL values did not change significantly after posterior capsulotomy (p > 0.05).
Comparisons of CCT, ACD (excluding the cornea), ACD (including the cornea), lens vault, pupil diameter, and tilt of IOL values before and after Nd:YAG laser posterior capsulotomy.
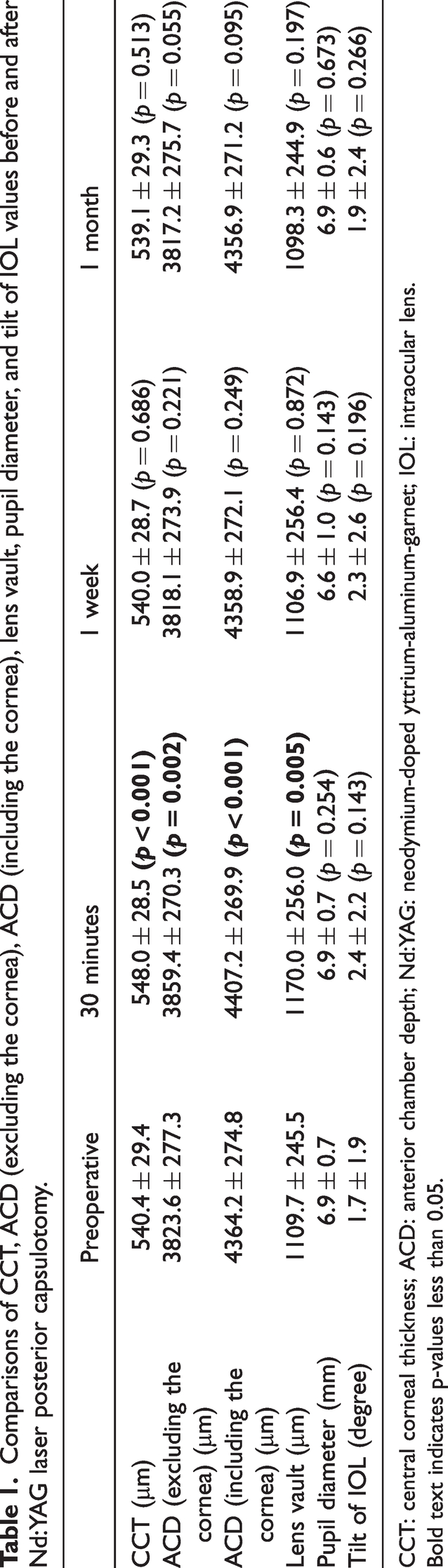
CCT: central corneal thickness; ACD: anterior chamber depth; Nd:YAG: neodymium-doped yttrium-aluminum-garnet; IOL: intraocular lens.
Bold text indicates p-values less than 0.05.
The mean values of anterior segment parameters, including the CCT, ACD (excluding the cornea), ACD (including the cornea), lens vault, pupil diameter, and tilt of IOL, in the C-loop–type and plate-type IOL groups at 30 min, 1 week, and 1 month postoperatively were summarized in Table 2. Both C-loop–type and plate-type IOL groups exhibited statistically significant increases in the CCT, ACD (excluding the cornea), and ACD (including the cornea) after capsulotomy (all p < 0.05), which returned to baseline values at 1 week and 1 month postoperatively. In the C-loop–type and plate-type IOL groups, compared with the values at baseline, the average increases in the degree of ACD (excluding the cornea) at 30 min after Nd:YAG laser capsulotomy were 20 ± 36.3 µm and 51.7 ± 78.9 µm, respectively; there was no significant difference in the increases in the two groups (p = 0.072) (Table 3). With respect to the lens vault values, only the plate-type IOL group showed significant increases at 30 min after Nd:YAG laser capsulotomy (p = 0.025); however, there was still no statistically significant difference in the lens vault values at 30 min postoperatively between the C-loop–type and plate-type IOL groups (p = 0.342) (Table 3).
Comparisons of anterior segment parameters before and after Nd:YAG laser posterior capsulotomy in the C-loop–type (n = 18) and plate-type (n = 18) IOL groups.

CCT: central corneal thickness; ACD: anterior chamber depth; Nd:YAG: neodymium-doped yttrium-aluminum-garnet; IOL: intraocular lens.
Bold text indicates p-values less than 0.05.
Comparisons of the changes in anterior segment parameters obtained before and after Nd:YAG laser posterior capsulotomy at different time points between the C-loop–type (n = 18) and plate-type (n = 18) IOL groups.
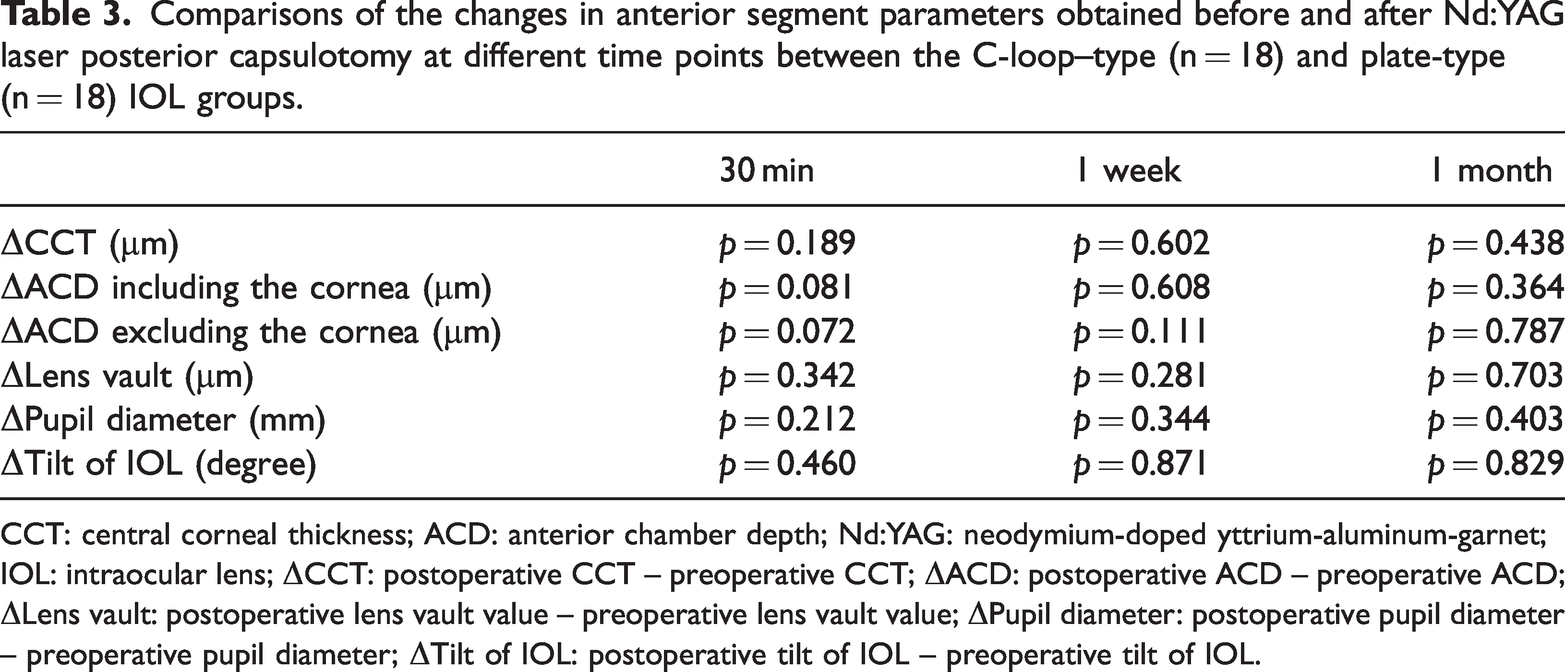
CCT: central corneal thickness; ACD: anterior chamber depth; Nd:YAG: neodymium-doped yttrium-aluminum-garnet; IOL: intraocular lens; ΔCCT: postoperative CCT – preoperative CCT; ΔACD: postoperative ACD – preoperative ACD; ΔLens vault: postoperative lens vault value – preoperative lens vault value; ΔPupil diameter: postoperative pupil diameter – preoperative pupil diameter; ΔTilt of IOL: postoperative tilt of IOL – preoperative tilt of IOL.
Discussion
The intact posterior capsule supports the IOL and sustains the barrier function between the anterior and posterior compartments of the eye. Stability of the IOL position has been an important problem after Nd:YAG laser capsulotomy for unexpected visual problems. The possible collateral damage mechanisms of laser capsulotomy on the ocular structures include plasma formation and expansion, emission of acoustic waves, cavitation bubble formation, focusing errors, and the generation of inflammatory debris and mediators.6,13 Despite wide clinical use, not many studies have reported the impact of laser capsulotomy on the ocular tissues, particularly the anterior segment. In current clinical practice, accurate and stable IOL positioning after cataract surgery is becoming increasingly important. Every year, new multifocal and extended-depth-of-focus IOLs are released, widening the variety of options and ability to offer the best solution to patients with higher demands. However, these IOLs are extremely sensitive to movement and decentration, 16 resulting in increased higher-order aberrations, coma, photic phenomena, and visual quality degradation,17,18 especially during near-vision activities. Although IOL positioning seems to exert considerable influence on multifocal IOL performance, monofocal IOL decentration has also been studied and is shown to compromise vision quality. 19 Thus, movement of the IOL after Nd:YAG capsulotomy in the treatment of PCO could potentially cause refractive changes and visual quality degradation.
With respect to CCT, SS-OCT revealed that the CCT increased at 30 min after Nd:YAG laser capsulotomy and returned to the baseline value at 1 week and 1 month postoperatively (Table 1). Furthermore, the increase in the degree of CCT at 30 min in the plate-type IOL group was not significantly different from that in the C-loop–type IOL group (Tables 2 and 3). Presumably, the temporary corneal edema occurred after the capsulotomy and was caused by the use of local anesthesia eye drops or contact lens or due to damage to the corneal endothelial cells. Several authors have reported no significant changes in the CCT after Nd:YAG capsulotomy at postoperative 1 week and 1 month, as measured using a Sirius rotating camera 11 (Costruzione Strumenti Oftalmici, Scandicci, Italy) and Scheimpflug camera 6 (Oculus, Wetzlar, Germany), respectively. Furthermore, one study found that CCT increased at postoperative 30 min and reverted to the baseline value at postoperative 1 week and 1 month, as measured using Pentacam HR (Oculus, Wetzlar, Germany), consistent with our results. 7 In another study, the temporary increase in the CCT was observed for up to 3 months postoperatively, and a statistically significant correlation between CCT increase and total laser energy used was found. 20 Vaikoussis et al. 21 showed corneal endothelial damage after laser capsulotomy in rabbit eyes when high laser energy was used. In contrast, Filipecka et al. 22 reported no significant changes in the confocal microscopy images of the cornea after laser capsulotomy.
With respect to ACD, we found increased ACD at 30 min after Nd:YAG laser capsulotomy, which may indicate that the IOL shifted backwardly after the capsulotomy (Table 1), furthermore, the degree of the backward movement in plate-type IOL group was much higher than that in the C-loop–type IOL group (Table 2); however, this difference was not statistically significant (Table 3). Moreover, when we observed the ACD parameter for as long as 1 week and even 1 month postoperatively, we found that the ACD in both types of IOLs returned to their baseline levels after Nd:YAG laser capsulotomy. Optimal cataract surgery aims precise IOL positioning for better refractive results. Visual quality may be compromised with IOL movement; therefore, we evaluated IOL movement by measuring the ACD in our study. Several authors have reported no significant changes in the ACD after Nd:YAG capsulotomy. For instance, Khambhiphant, Pekel, and João reported no significant changes in the ACD, as measured using IOL Master 500 (Carl Zeiss Meditec, Dublin, California, USA), 8 Pentacam HR, 7 and SS-OCT, 23 respectively. In contrast to our study, Oztas et al. 12 and Akmaz et al. 11 reported forward movement of the IOL, as measured using Pentacam HR and Sirius rotating cameras, respectively, and indicated that the 1-piece IOLs moved less than the 3-piece IOLs along the optical axis. However, similar to our results, Parajuli et al. 10 reported backward movement of the IOL, as measured using IOL Master. In addition, with the use of anterior segment OCT (Carl Zeiss Meditec, Dublin, California) Eliacik et al. 9 found an increase in the ACD at postoperative 3 days following Nd:YAG laser capsulotomy. Using optical coherence biometry (Biograph WaveLight OB820), Tiago reported that yttrium-aluminum-garnet (YAG) posterior capsulotomy decreased the ACD in plate-type IOL group but increased it in the C-loop–type IOL group. 24 Different anterior segment analyzing systems may be responsible for variations in results; for example, the anterior vitreous pressure after capsulotomy may be responsible for the temporary anterior IOL movement. In sum, our results suggest that Nd:YAG laser capsulotomy has no significant effect on the IOL movement in the long term.
With respect to lens value, we found increased lens vault values at 30 min after Nd:YAG laser capsulotomy; this may indicate that the IOL shifted in the backward direction after the capsulotomy, similar to the trend observed for ACD (Table 1). Furthermore, although the mean level of lens vault in both C-loop–type and plate-type IOL groups showed an increased tendency, only the plate-type IOL group showed a statistically significant difference at 30 min after Nd:YAG laser capsulotomy compared with the baseline value (Table 2). In addition, there was no statistically significant difference between the two IOL groups (Table 3). When we observed the lens vault parameter for 1 week and even 1 month, we observed that the lens vault in both types of IOLs returned to their baseline values after the Nd:YAG laser capsulotomy. When we reviewed previous literature on the change in lens vault values after Nd:YAG laser capsulotomy, we found only one study that showed no statistically significant changes in lens vault values, as measured using ultrasound biomicroscopy at 1 week and 1 month postoperatively, which is consistent with the results in our study. However, they did not detect the value of lens vault at 30 min after the capsulotomy. 25
With respect to the pupil diameter, considering that the pupil dilation could increase the ACD 26 and even CCT, 27 all patients were evaluated after pupil dilation at the follow-up; pupil diameters showed no statistically significant difference between the preoperative and postoperative groups (Table 1) as well as between the C-loop–type and plate-type IOL groups (Tables 2 and 3).
With respect to the tilt of IOL, most studies found that the tilt of IOL decreased at postoperative 1 month, as measured using a Scheimpflug camera 6 ; however, one study showed that the tilt of IOL did not change at postoperative 1 h, as measured using optical biometry (Lenstar LS900), 13 which is consistent with our results (Table 1).
Limitations
First, a 1-month follow-up duration may be insufficient for detecting long-term anterior segment differences between the two IOL models after capsulotomy. Second, the sample size was relatively small, and larger studies are needed to confirm our results. Third, patients with high myopia and microphthalmia were excluded from this study; therefore, the effects of Nd:YAG laser capsulotomy on anterior segment parameters in patients with excessively long or short axial lengths were not investigated. Despite these limitations, our results can aid further investigation of the IOL movement after Nd:YAG laser capsulotomy.
Conclusion
In this study, we discussed the effect of Nd:YAG laser capsulotomy on anterior segment parameters as well as the IOL movement in patients, using an anterior segment SS-OCT system. We also performed individual comparisons of the IOL movement between the C-loop–type and plate-type IOL groups, with the latter showing less stability at 30 min after the capsulotomy, but both showing no significant changes in the ACD and lens vault values at 1 week and 1 month after the capsulotomy. We suggest that Nd:YAG capsulotomy causes a temporary increase in the CCT, ACDs, and lens vault, but does not cause significant long-term changes in the cornea thickness and IOL movement.
Footnotes
Acknowledgments
We are thankful to the patients who participated in this study.
Authors’ contribution statements
Bei Zhang designed this project, performed all the Nd:YAG laser capsulotomy, and revised this manuscript; Haiyang Yu performed data analysis and prepared the manuscript; Yixu Mao performed the swept-source optical coherence tomography (SS-OCT), Optical Path Difference Scan III (OPD-Scan III) measurements, and data collection. All authors contributed to the article and approved the submitted version.
Consent to participate
All participants in this study provide written informed consent.
Consent for publication
Informed consent for publication was provided by the participants.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors report that there are no competing interests to declare.
Ethical considerations
This study was conducted as per the ethical standards of the Declaration of Helsinki of 1975, as revised in 2024. This study was approved by the institutional ethical committee of our hospital.
Funding
This work was supported by the Basic Public Welfare Research Program of Zhejiang Province under Grant (number GF21H120010) awarded to Bei Zhang.