
Abstract
Proximal femoral nail antirotation, a common surgical procedure for intertrochanteric fractures, is rarely associated with deep femoral artery injury during distal locking in clinical practice. This article reports a unique case in which excessive penetration of a distal locking drill bit through the medial cortex during proximal femoral nail antirotation internal fixation caused accidental injury to the mid-to-distal branch of the deep femoral artery, resulting in a pseudoaneurysm with active bleeding. The diagnosis was confirmed using digital subtraction angiography, after which emergency endovascular coil embolization was successfully performed to achieve hemostasis. The patient showed significant improvement and was discharged without recurrence during follow-up. This case highlights the need for a high index of suspicion for potential deep femoral artery injury in patients presenting with extensive skin bruising accompanied by a pulsatile mass, particularly in older individuals and those with osteoporosis. Additionally, implementing appropriate preventive measures during surgery to avoid deep femoral artery injury is crucial.
Keywords
Introduction
Intertrochanteric fractures are common in older individuals, accounting for approximately one-third to half of all hip fracture cases. 1 Despite significant advancements in the treatment of intertrochanteric fractures over the past 30 years, they remain a major challenge for orthopedic surgeons, particularly in cases of unstable intertrochanteric fractures. Femoral artery injury is a rare complication of internal fixation for intertrochanteric fractures (0.2% incidence),2,3 predominantly involving the common femoral artery, superficial femoral artery, and profunda femoris artery and its branches.4–6 Depending on the extent of vessel wall damage, massive intraoperative bleeding or the formation of a subacute hematoma may lead to arterial pseudoaneurysm. The first case of distal locking pin–related injury to the deep femoral artery and subsequent pseudoaneurysm formation was reported in 1964. 7
Herein, we report the case of a patient with an injury to the middle and distal branches of the profunda femoris artery caused by excessive insertion of a distal locking drill bit during proximal femoral nail antirotation (PFNA) fixation for the treatment of an intertrochanteric fracture (Table 1). Furthermore, we systematically describe the clinical presentation, diagnostic process, and treatment approach for this case. Comprehensive knowledge of the profunda femoris artery is essential to prevent clinical risks associated with delayed diagnosis and incomplete treatment. To the best of our knowledge, this report presents one of the few such cases reported worldwide.
Demographic data of the patient and details of the procedure and clinical response.
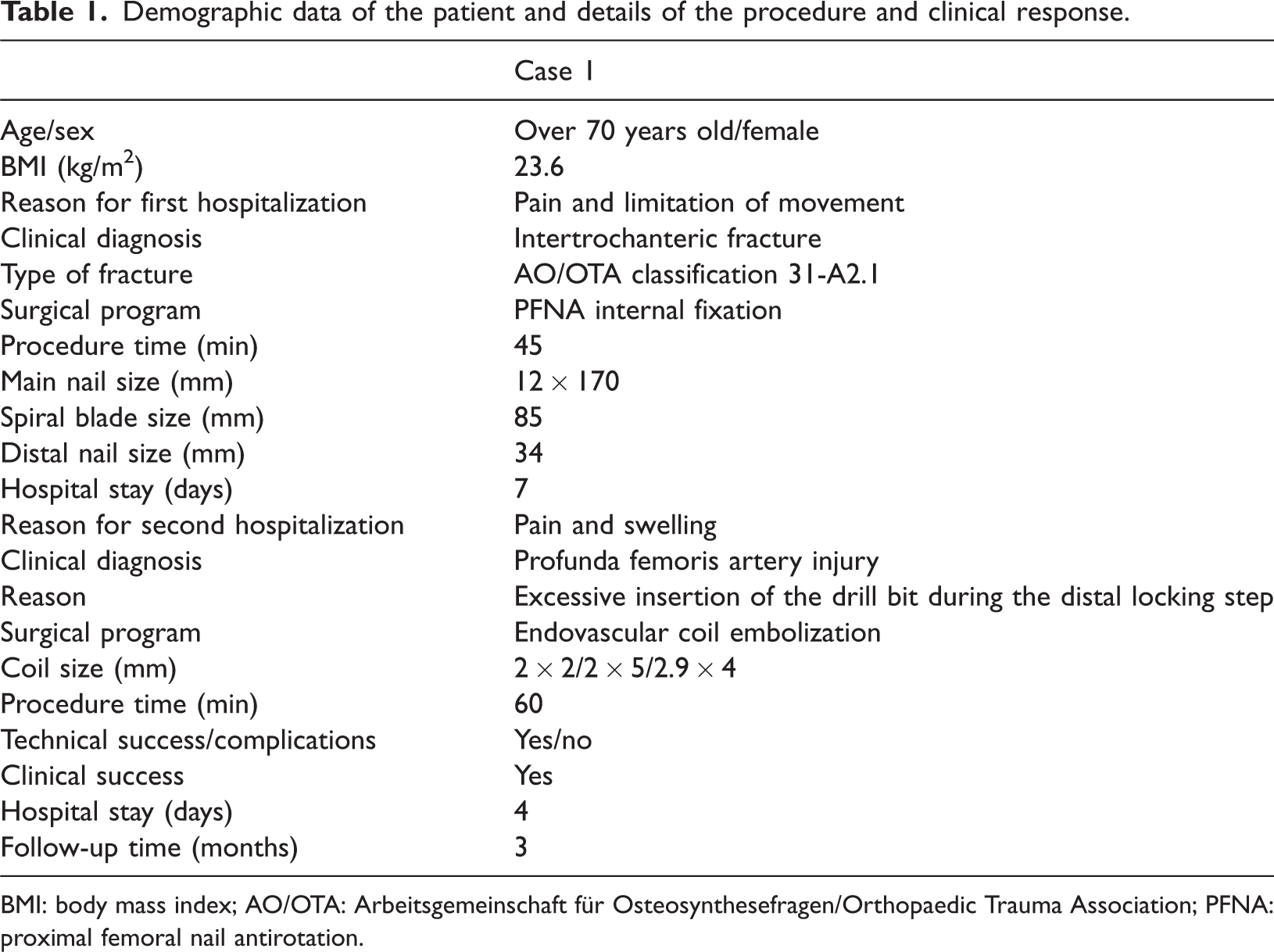
BMI: body mass index; AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association; PFNA: proximal femoral nail antirotation.
Case presentation
A female patient in her 70s was admitted to the Guiyang Fourth People’s Hospital, Guizhou Province, China, in March 2024 due to right hip pain and limited mobility following an accidental fall while walking. She was diagnosed with a right intertrochanteric femoral fracture (Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) classification 31-A2.1, Figure 1(a)) and subsequently underwent closed reduction and internal fixation using PFNA under anesthesia. The main nail measured 12 × 170 mm, the helical blade 85 mm, and the distal locking nail 34 mm; postoperative hip radiographs were obtained (Figure 1(b)). The surgical procedure and postoperative recovery were uneventful, and the patient was discharged 5 days after surgery.

Imaging examination and thigh inspection. (a) Intertrochanteric fracture: X-ray image showing a right intertrochanteric fracture. (b) Postoperative X-ray showing the status after internal fixation with PFNA for right intertrochanteric fracture. (c) Thigh inspection: One month after surgery, a large region of skin bruising was visible on the back of the patient’s thigh, along with a palpable pulsatile mass. (d) MRI showing a mixed-signal mass in the medial soft tissue of the upper femur, measuring approximately 97 × 83 mm, suggesting hematoma formation. (e) DSA showing contrast extravasation in the middle branches of the penetrating artery of the right profunda femoris artery, and “clumpy shape” contrast retention was seen in the soft tissues. (f) DSA showing contrast extravasation in the distal branches of the penetrating artery of the right profunda femoris artery, with “clumpy shape” contrast retention seen in the soft tissues. (g) Coil insertion: Under the guidance of a microguidewire, the microcatheter was placed in the middle branch of the profunda femoris penetrating artery, where two “coils” were deployed. (h) Coil insertion: Under microguidewire guidance, the microcatheter was further advanced to the distal branch of the profunda femoris penetrating artery where two “coils” were deployed and (i) thigh inspection: Three months following embolization of the profunda femoris artery, skin bruising on the back of the patient's thigh disappeared, and the pulsatile mass was no longer present. DSA: digital subtraction angiography; MRI: magnetic resonance imaging; PFNA: proximal femoral nail antirotation.
Four weeks after discharge, the patient presented with sudden pain and swelling in the posterior aspect of the right thigh. Physical examination revealed extensive subcutaneous bruising over the posterior thigh, accompanied with a palpable pulsatile mass (Figure 1(c)). Magnetic resonance imaging revealed a mixed-signal mass in the medial soft tissue of the upper femur, measuring approximately 97 × 83 mm, suggestive of hematoma formation (Figure 1(d)). Digital subtraction angiography (DSA) demonstrated injury to the middle and distal branches of the penetrating right profunda femoris artery (Figure 1(e) and (f)). Endovascular coil embolization of the injured artery was subsequently performed to achieve hemostasis.
During the operation, the patient laid supine on the operating table, and the puncture site was selected at the point of strongest femoral artery pulsation, 0.5 cm below the skin line of the right groin. Local infiltration anesthesia with 2% lidocaine was administered, and femoral artery puncture was performed using Seldinger’s technique. Under fluoroscopic guidance, a 5-F catheter sheath was placed and successively advanced into the right external iliac artery, profunda femoris artery, and superficial femoral artery under the guidance of an ultrasmooth guidewire. A contrast agent was slowly injected to perform angiography. Contrast extravasation was observed in the middle and distal branches of the penetrating artery of the right profunda femoris artery and in the surrounding soft tissues; however, no contrast leakage was observed in the right external iliac or superficial femoral arteries. Under microguidewire guidance, the microcatheter was placed in the middle branch of the deep femoral penetrating artery, where two coils (2 × 2 mm) were deployed (Figure 1(g)). Subsequently, the microcatheter was further advanced to the distal branch of the deep femoral penetrating artery, where two coils (2 × 5 mm/2.9 × 4 mm) were deployed (Figure 1(h)). Following injection of the contrast agent, the results showed that complete embolization was achieved without any significant contrast extravasation or contrast retention in the soft tissues. Both the technical success rate and clinical response rate were 100%. The patient was hospitalized for 4 days and followed up for 3 months after discharge. The skin bruising completely resolved, and the symptoms of the pulsatile mass and pain subsided.
Written informed consent was obtained from the patient for treatment, use of clinical data for research, and publication of individual medical information and accompanying images. We deidentified all patient details. The reporting of this study conformed to the Case Report (CARE) guidelines. 8
Discussion
Femoral vascular injury is a rare complication of internal fixation for intertrochanteric fractures, predominantly involving the common femoral artery, superficial femoral artery, and profunda femoris artery and its branches. In our case, DSA confirmed that the pseudoaneurysm resulted from injury to the middle and distal branches of the penetrating deep femoral artery. We believe that excessive insertion of the drill during the distal locking step of the procedure caused injury to the middle and distal branches of the profunda femoris artery, leading to arterial perforation. Additionally, when the drill was withdrawn, the originally injured blood vessels and surrounding soft tissues were embedded between the nail tail and the femur, further exacerbating vascular damage. During postoperative limb movement, the injured blood vessels were subjected to continuous traction and stimulation, which, coupled with the use of anticoagulant medication, ultimately led to the formation of a pseudoaneurysm. However, atherosclerosis and weakening of the elasticity of the vessel wall, which occur in older patients, may also be contributing factors.9,10
The treatment strategy for profunda femoris artery injury should be determined based on the patency of the superficial femoral artery. 11 Treatment options primarily include endovascular approaches, such as coil embolization, followed by open surgical techniques, including arterial ligation with or without the removal of the bone fragment and, in some cases, stent implantation or vein patch repair.12,13 However, owing to the presence of hematoma and active bleeding, the technical difficulty of open surgery has significantly increased. 14 Consequently, minimally invasive alternatives are more appealing because they effectively avoid complications associated with open repair, such as large incisions, bleeding, or infection. 15 Endovascular embolization for vascular injuries represents an advancement in both therapeutic philosophy and technical execution. This shift from extensive surgical repair to minimally invasive endovascular closure aligns with contemporary medical trends toward precise and minimally invasive approaches. Compared with alternative treatment modalities, endovascular embolization has emerged as the preferred therapeutic option because of the associated minimal trauma and rapid postoperative recovery.16,17 Our findings support this conclusion.
Arterial embolization, as an interventional treatment method, aims to treat diseases by blocking blood flow; however, it may further lead to a series of complications, such as vascular recanalization, ischemia, vascular injury, and thrombosis. This underscores the need for considerable expertise and a long learning curve to select appropriate embolic materials, understand the vascular anatomy, and perform the procedure effectively to reduce the occurrence of these complications. For patients with coexisting atherosclerosis and severe stenosis or occlusion of the superficial femoral artery, profunda femoris artery embolization should be performed with extra caution, and the embolization scope should be minimized as much as possible to preserve collateral circulation and maintain adequate blood flow to the lower limbs.
Based on these findings, we recommend maintaining a high index of suspicion in patients presenting with the following clinical symptoms: (a) a persistent drop in the patient’s postoperative hemoglobin level, provided that bleeding from other sites is excluded; (b) extensive skin bruising with a pulsatile mass; and (c) persistent thigh swelling and pain. Importantly, such complications can often be avoided during surgery. First, although excessive adduction and internal rotation may be necessary to reduce intertrochanteric fractures, they are not required during distal locking. We recommend positioning the limb in a neutral position during this step. Second, in older patients and those with osteoporosis, the force applied during distal locking should be carefully controlled, or a depth limiter should be used to prevent any excessive insertion of the drill bit and vascular injury. Finally, most crucially, surgeons must thoroughly comprehend the anatomical relationships and clearly identify the “dangerous zone.” The deep femoral artery typically originates from the femoral artery approximately 2.5–6 cm below the tip of the lesser trochanter, traversing medially and posteriorly. It then rapidly produces perforating arteries, which closely follow the linea aspera of the femur as they traverse medially and posteriorly.
This study reports a rare case of iatrogenic deep femoral artery injury caused by excessive drill insertion during the distal locking phase of PFNA internal fixation for an intertrochanteric fracture in an older female patient. This article systematically describes the clinical presentation, diagnostic process, and treatment strategies for such injuries, providing a representative clinical example. This report contributes to enhancing the recognition of characteristic manifestations and offers guidance for treatment decisions in similar cases. This study has certain limitations. As a single case report, the limited sample size makes it difficult to comprehensively assess individual variations in deep femoral artery injury with respect to age, degree of fracture displacement, and severity of injury.
Conclusion
Postoperative vascular injuries following intertrochanteric fracture fixation are relatively rare. However, older patients, who frequently present with comorbid osteoporosis and vascular atherosclerosis, are at higher risk of such injuries. Therefore, orthopedic surgeons should exercise caution during surgery. If there is a high index of suspicion, DSA should be performed promptly to prevent treatment delay. In summary, a thorough understanding of the anatomy of the deep femoral artery and the mechanisms of injury is crucial to prevent the clinical risks associated with delayed diagnosis or inadequate management.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251387943 - Supplemental material for Iatrogenic injury to the profunda femoris artery during distal locking of an intertrochanteric fracture: A case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605251387943 for Iatrogenic injury to the profunda femoris artery during distal locking of an intertrochanteric fracture: A case report and literature review by Zuzhou Wen, Hongqiang Chen, Junzhao Qiao and Yun Ye in Journal of International Medical Research
Footnotes
Author contribution
Zuzhou Wen: manuscript drafting and data collection. Hongqiang Chen: critical revisions and supervision. Junzhao Qiao: critical revisions and supervision. Yun Ye: Formal analysis, writing–review & editing.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the scientific research project of the Science and Technology Association of the Fourth People's Hospital of Guiyang City, Project No. (GYSYKX[2025]05).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.