
Abstract
Background
The interaction between manifest refractive astigmatism and topographic astigmatism is critical in planning refractive surgery. This study aimed to investigate the predictive relationship between manifest refractive astigmatism and topographic astigmatism across different age groups.
Methods
This is a retrospective observational study comprising 149 patients. Manifest refractive astigmatism was evaluated through subjective refraction methods, and topographic astigmatism was measured using corneal topography. Inclusion criteria were patients aged 20–41 years without a history of ocular surgery or severe corneal pathology. The main outcome was to determine the relationship between manifest refractive astigmatism and topographic astigmatism and to test whether manifest refractive astigmatism served as a reliable predictor of topographic astigmatism in two age groups (≤30 and >30 years).
Results
Pearson correlation analysis revealed a strong positive correlation between manifest refractive astigmatism and topographic astigmatism (r = 0.846, p < 0.001). Linear regression analysis indicated that manifest refractive astigmatism accounted for 71.7% of the variance in topographic astigmatism. No significant differences were observed between younger and older age groups in the predictive relationship.
Conclusions
Manifest refractive astigmatism is a reliable predictor of topographic astigmatism, and it is not a substitute for topographic astigmatism in surgical practice but serves as a supportive measure. The strong correlation across age groups highlights its value in clinical practice.
Introduction
Astigmatism is the most prevalent refractive error, which is believed to affect 40% of the population. 1 Clinically, astigmatism is frequently measured using various instruments, such as manifest refractive astigmatism (MRA) and topographic astigmatism (TA). MRA, obtained through subjective refraction measurements, reflects the eye’s overall refractive state by incorporating contributions from both the cornea and lens, while TA, derived from corneal topography, measures only the anterior corneal surface.2,3 Numerous studies have reported discrepancies between MRA and TA, particularly in magnitude and axis.4,5 These discrepancies are largely attributed to ocular residual astigmatism (ORA), defined as the vector difference between MRA and TA arising from posterior corneal curvature, lens-induced astigmatism, and other ocular factors. 3 When considering laser-assisted in situ keratomileusis (LASIK) and other refractive surgeries, such discrepancies are critically important because they influence the predictability and outcomes of the surgery.2,3
The use of topography-guided (TG) therapy has historically been limited to challenging cases, such as irregular astigmatism. 6 In normal eyes without irregular astigmatism, TG LASIK has been demonstrated to provide outstanding visual results; at 12 months, 93% of eyes achieved 20/20 or higher uncorrected distance visual acuity (UDVA), and 34% achieved 20/12.5 or better UDVA. 7 Ideally, the Manifest and Topo cylinders should be identical or comparable, but they occasionally differ significantly. High-order corneal aberrations, posterior corneal astigmatism, and lenticular astigmatism are potential causes of this discrepancy.2,8 A study conducted among schoolchildren in Iraq found astigmatism as the most prevalent refractive error, affecting 14.5% of the studied population, surpassing hyperopia (13.9%) and myopia (3.8%). 5 The study emphasized the need to address uncorrected refractive errors, as 32.2% of the students had visual impairments due to refractive errors, with astigmatism being a significant contributor. These findings highlight the importance of understanding the relationship between different forms of astigmatism, especially as they affect visual outcomes across various age groups.
The biomechanics of the lens and cornea also exhibit age-related changes, affecting the interaction between MRA and TA. Younger patients have more flexible lenses and smooth corneal surfaces, while older individuals are prone to lens opacification and corneal hardening, rendering astigmatism correction more challenging. 5 These factors necessitate an age-dependent strategy for astigmatism correction in procedures such as LASIK, where outcomes may vary depending on patient age and the chosen astigmatism axis.4,5
ORA, first conceptualized by Alpins in 1997, is defined as the vectorial difference between MRA and anterior corneal astigmatism (ACA) and is considered clinically elevated when it exceeds 0.73–0.81 diopters (D). 9 Unlike scalar comparisons of magnitude alone, ORA accounts for both magnitude and axis, making it an essential parameter in vector planning for astigmatism correction. The Alpins method of astigmatism analysis uses double-angle vector diagrams to evaluate how residual astigmatic components from the lens and posterior cornea influence outcomes. 10 Clinical data indicate that high ORA values (≥0.75 D) are associated with reduced refractive accuracy and increased postoperative visual disturbances, particularly glare and halos. 11 Consequently, Alpins and others advocate routine preoperative calculation of ORA and incorporation of vector planning to balance refractive and corneal components, improving overall surgical predictability and preserving corneal shape. Patients with uncorrected astigmatism may experience distorted vision, eyestrain, and diplopia. In addition, such patients often experience reduced vision-related quality of life, increased risk of falls, difficulty driving at night, and overall poorer well-being. 12
This study aimed to explore the predictive relationship between the severity of MRA and TA across different age groups. By comparing young and older patients, we sought to identify patterns that may enhance the precision of refractive surgeries and improve long-term visual outcomes.
Method
Study design
This study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 13 A retrospective observational study was conducted among 149 patients with astigmatism who visited a private ophthalmic clinic. The primary aim was to investigate the relationship between MRA and TA in young (≤30 years old) and older (>30 years old) individuals. Refractive and topography values were extracted from patient records to assess the correlation between MRA and TA.
Study setting and dates
The study was conducted in a private ophthalmology clinic, and the patient data were collected over a 6-month period. All patients underwent comprehensive ocular examinations during routine visits.
Sample size justification
The sample size of 149 patients was selected based on practical constraints, including the availability of patient records and the timeline of data collection. Although this limited the study’s power, the sample was considered adequate to provide preliminary insights into the MRA–TA relationship across different age groups.
Inclusion and exclusion criteria
Inclusion criteria included a confirmed diagnosis of astigmatism through manifest refraction and corneal topography and the availability of complete refractive and topographic data. Exclusion criteria included a history of ocular surgery (e.g. LASIK, photorefractive keratectomy, and cataract surgery), corneal diseases such as keratoconus, incomplete medical records, or ocular surface diseases such as dry eye.
Measurement of MRA
MRA was measured using subjective refraction techniques performed by a trained optometrist. Refraction was performed using standardized methods with a retinoscope, phoropter, and Snellen chart at a distance of 6 m, following the guidelines set by the American Academy of Ophthalmology.
Measurement of TA
TA was measured using Sirus corneal topography, focusing on the steep and flat meridians of the anterior and posterior cornea; the measured astigmatism represented true corneal power. All patients underwent comprehensive anterior segment evaluations, and keratometry readings (K1 and K2) were recorded to calculate the corneal astigmatic cylinder and meridian.
Data collection and variables
Data collection included patient age, MRA (cylinder power and axis), and TA (cylinder power and meridian). ORA, defined as the vectorial difference between MRA and TA, was calculated for each patient to evaluate any discrepancies. Patients were stratified by age into younger and older groups to analyze age-related differences in the MRA–TA relationship.
Bias
Potential sources of bias included selection bias from convenience sampling in a private clinic and measurement bias inherent in subjective refraction methods.
Handling of missing data
All patient records had complete refractive and topographic data. Therefore, no imputation for missing data was required.
Statistical analysis
Descriptive statistics, including mean, standard deviation, and range, were calculated for MRA and TA across both age groups. Pearson’s correlation coefficient was used to assess the strength of the MRA–TA relationship, with separate analyses performed for the younger and older age groups. Independent t-tests were used to compare MRA and TA between the two age groups, with statistical significance set at p < 0.05. Linear regression analysis was conducted to evaluate whether MRA could predict TA, with age as a moderating variable.
Ethical considerations
The study adhered to the ethical standards of the 1975 Declaration of Helsinki, as revised in 2024. Ethical approval was obtained from the Research Ethics Committee, Department of Surgery, College of Medicine, University of Baghdad (Approval No. 336, dated 12 April 2024). As this was a retrospective study, signed consent was not required. All data were anonymized and used in accordance with institutional ethical standards.
Results
Descriptive data
A total of 149 patients were included in the analysis, comprising 92 females and 57 males (Table 1). The mean patient age was 27.05 (SD = 6.55) years, with 52.3% of the cohort being 30 years or younger and 47.7% being older than 30 years. Both MRA and TA were recorded for all patients. The magnitude of MRA ranged from 0.00 to 11.0 D, while that of TA ranged from 0.00 to 4.25 D. No patients had missing data, and all cases were included in the final analysis.
Demographic characteristics of the patient cohort (n = 149).

Relationship between MRA and TA
Pearson’s correlation was performed to assess the strength of the relationship between MRA and TA (Figure 1). The correlation coefficient was 0.846, indicating a strong positive relationship between the two variables. This result suggested that as the severity of MRA increased, the degree of TA also increased proportionally across the studied cohort.

Scatter plot showing the X and Y vector components of astigmatism. Blue points represent topographic astigmatism (TA), orange points represent manifest refractive astigmatism (MRA), and gray points represent ocular residual astigmatism (ORA). Yellow, green, and red points represent the corresponding support vector machine predictions for TA, MRA, and ORA, respectively. The X-axis shows the double-angle cosine component, and the Y-axis shows the double-angle sine component of astigmatism.
Regression analysis
A linear regression analysis was performed to evaluate whether MRA could predict TA (Table 2). The regression model explained 71.7% of the variance in TA (R2 = 0.717), demonstrating a high degree of predictability. The regression coefficient for MRA was 0.983 (p < 0.001), indicating that for each unit increase in MRA, TA increases by approximately 0.98 units on average. The constant term in the model was −0.168 (p = 0.082) and was not statistically significant. The F-statistic was 19.28 (p < 0.001), confirming that the overall model was highly statistically significant.
Linear regression analysis predicting TA from MRA.

MRA: manifest refractive astigmatism; TA: topographic astigmatism.
Subgroup analysis by age
To investigate age-related differences, the sample was divided into two age groups: those aged 30 years or younger and those aged over 30 years. The correlation between MRA and TA remained strong in both groups (r = 0.846 for younger patients and r = 0.847 for older patients), with no significant differences observed in regression coefficients.
A multiple linear regression was conducted to evaluate the relationship between MRA and TA while controlling for age and sex. MRA remained a statistically significant predictor of TA (β = 0.738, p < 0.001), while age (p = 0.850) and sex (p = 0.240 for females, p = 0.526 for males) were not significant contributors. The model explained 72.4% of the variance in TA (R2 = 0.724) (Table 3).
Multiple linear regression predicting TA value.
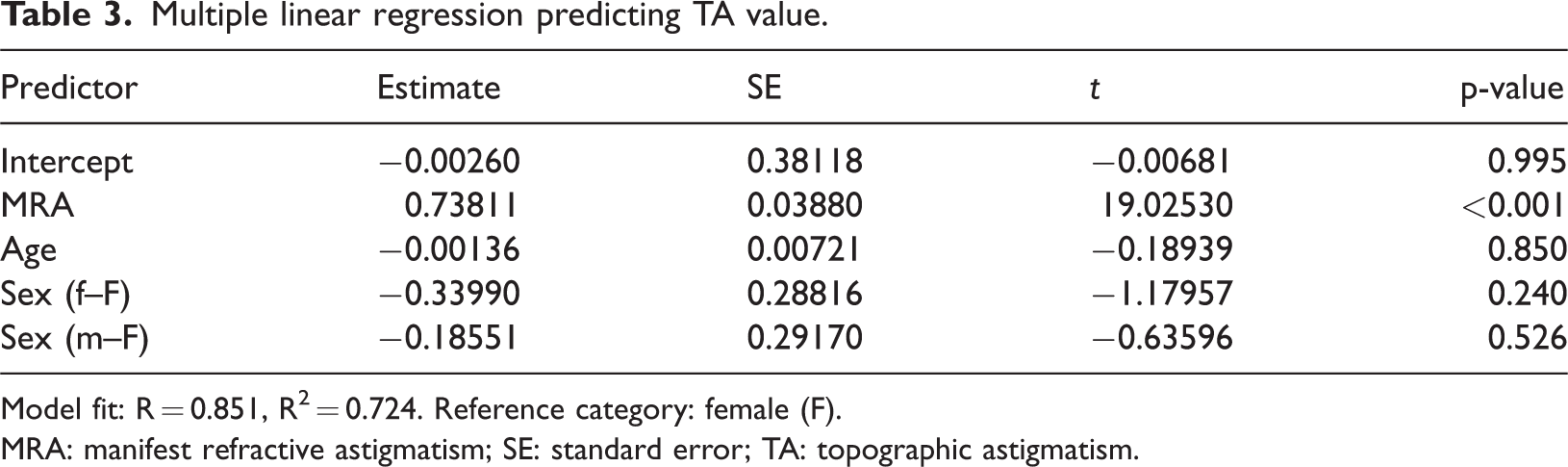
Model fit: R = 0.851, R² = 0.724. Reference category: female (F).
MRA: manifest refractive astigmatism; SE: standard error; TA: topographic astigmatism.
Discussion
Astigmatism, first defined by Thomas Young in the early 19th century, evolved from a rare curiosity to a well-understood refractive error. George Airy’s use of cylindrical lenses in 1825 marked the beginning of effective correction. 14 This study revealed a strong positive association between MRA and TA, with a Pearson correlation of 0.846, demonstrating that MRA values are associated with greater TA. The high predictability of TA from MRA observed in this study supports the clinical practice of prioritizing MRA when planning corrective procedures.
The 30-year threshold was selected based on the literature suggesting that age-related biomechanical changes in the cornea and crystalline lens begin to emerge in the third decade of life, affecting refractive stability and astigmatic correction outcomes.1,12 This cutoff has been adopted in previous ophthalmic research to distinguish younger adults with more flexible lenses and corneal biomechanics from older patients who may show early lens opacities and corneal stiffening. Therefore, the 30-year threshold serves as a clinically relevant cutoff for assessing age-related differences in the MRA–TA relationship.
More recently, Wallerstein et al. 15 provided supporting evidence for the utility of MRA in clinical decision-making. Their large-scale study involving more than 25,000 eyes found no statistically significant relationship between anterior corneal higher-order aberrations, such as coma, and MRA–TA axis misalignment. Kim et al. 16 provided valuable insights into the comparison of different LASIK platforms, particularly topography-modified refraction (TMR), wavefront-optimized (WFO), and manifest TG LASIK, for astigmatism correction. Their findings demonstrated that although TMR-LASIK yielded comparable visual outcomes to WFO and TG LASIK, it showed a tendency toward overcorrecting astigmatism. Motwani 17 compared the clinical outcomes of manifest refraction with those of newer planning software in TG refractive surgery for astigmatism and myopia. The results indicated that although both methods yielded similar visual outcomes, manifest refraction may help prevent errors associated with corneal higher-order aberrations. This is specifically applicable to our work, in which a strong predictive factor between TA and MRA was highlighted.
Naser 18 proposed a theoretical model for integrating refractive and topography data in planning corneal laser refractive surgery. The technique is designed to maximize performance through a balance between refractive astigmatism and TA, ensuring that astigmatism of the cornea is not augmented with surgery. This approach aimed to reduce surgically induced astigmatism and improve refractive outcomes.
Wallerstein et al. 19 reported that even a significant preoperative axis mismatch between MRA and ACA, reaching up to 80°, did not adversely affect refractive or visual outcomes following topography-based LASIK. Their findings, based on over 25,000 cases, suggest that large axis disparities alone may not predict postoperative complications. However, these conclusions were derived from scalar comparisons of axis orientation rather than from full vectorial analysis. In contrast, ORA provides a more comprehensive measure by simultaneously accounting for magnitude and axis, as demonstrated in vector planning approaches. Although Wallerstein’s study supports targeting the manifest refraction axis in specific surgical settings, our findings further emphasize the predictive value of MRA on TA, particularly through the vectorial framework of ORA.
Several studies have confirmed that when ORA exceeds 0.75 D, visual outcomes may be compromised if not appropriately addressed. Vector planning, which balances both corneal and refractive components of astigmatism, has demonstrated superior outcomes in such cases. In a comparative study, Jun et al. 20 found that vector planning led to improved refractive accuracy compared with manifest planning in small incision lenticule extraction procedures for myopic astigmatism. These findings underscore the importance of incorporating ORA thresholds into surgical planning.
Limitation
One of the main limitations of this study is the small sample size. Additionally, the study was conducted in a single private ophthalmology clinic, which may introduce selection bias. The exclusion of patients with prior ocular surgeries or significant corneal pathologies further restricts the generalizability of the findings, as these conditions are common in clinical practice. Moreover, the potential correlation between both eyes in the same patient was not adjusted for in the analysis. Unfortunately, due to the retrospective nature of the study and the method of storing the clinical records, the dataset did not contain the required patient eye–linking identifiers in a format that would allow accurate clustering by patient ID. This prevented us from applying more robust statistical methods, such as generalized estimating equations (GEE). Although GEE and similar methods were not applied, we acknowledge that failing to account for inter-eye correlation may have resulted in underestimated variance and an increased risk of type I errors. Future studies should consider modeling patient ID as a random effect to address this limitation and strengthen the statistical integrity of the findings.
Conclusion
This analysis revealed a strong predictive association between MRA and TA across all age groups. With the incorporation of ORA and the application of vector planning methodologies, the clinical significance of MRA was further reinforced. These findings supported the use of MRA as a reliable indicator in surgical planning because it reflects both corneal and lenticular components. The lack of significant age-related differences also supports its applicability across age groups. Nevertheless, further prospective studies, incorporating posterior corneal astigmatism and full vectorial assessment, are warranted to confirm these findings and enhance surgical accuracy.
Footnotes
Acknowledgments
The authors acknowledge the support of the ophthalmic staff and patients at the Ibn Al-Haitham Teaching Eye Hospital.
Author contributions
Wissam Yosif contributed to conceptualization, literature review, and data interpretation. Ahmed Shakir Al-Wassiti was responsible for study design, statistical analysis, and manuscript drafting. Ali Nema Abushnein supervised the clinical methodology, provided expert ophthalmological input, and contributed to result validation. Muthanna Basheer Yasir participated in patient data acquisition, critical revision of the manuscript, and final approval of the version to be published.
AI tools
No AI tools were used in the generation of data, results, or analysis.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no conflicts of interest relevant to this manuscript.
Ethical approval
The study protocol was approved by the Research Ethics Committee of the Department of Surgery, College of Medicine, University of Baghdad (Approval No. 336, dated 12 April 2024). The study was conducted in accordance with the ethical standards of the 1975 Declaration of Helsinki, as revised in 2024.
Funding
No funding was received for this study.
Informed consent
As this was a retrospective study using anonymized patient data, informed consent was not required.