
Abstract
This case report presents a rare instance of neovascular glaucoma secondary to central retinal vein occlusion in a previously healthy man in his early 30s who exhibited acute unilateral vision loss, ocular pain, and elevated intraocular pressure. Ophthalmic imaging, including ultra-widefield fundus photography and optical coherence tomography, revealed retinal hemorrhages, intraretinal fluid, and iris neovascularization consistent with ischemic central retinal vein occlusion and secondary neovascular glaucoma. Notably, systemic evaluation revealed severe hyperlipidemia associated with the patient’s strict nonvegetarian diet, with no other identifiable risk factors. Treatment included intravitreal antivascular endothelial growth factor injections, Ahmed glaucoma valve implantation, and panretinal photocoagulation followed by pars plana vitrectomy. The patient experienced partial visual recovery after the initiation of lipid-lowering therapy and dietary counseling. This case underscores the importance of considering modifiable metabolic factors, particularly extreme dietary patterns, in young patients presenting with central retinal vein occlusion. It supports the incorporation of systemic lipid screening and dietary assessment into the diagnostic workup of atypical retinal vascular events. Although causality cannot be established, this case advocates the need for further investigation into the systemic implications of diet-related hyperlipidemia in ocular vascular disease.
Keywords
Introduction
Neovascular glaucoma (NVG) is a vision-threatening complication defined by the pathologic neovascularization of blood vessels in the iris and anterior chamber angle, leading to a marked increase in the intraocular pressure (IOP).1,2 Central retinal vein occlusion (CRVO) is one of the most common retinal vascular incidents linked with severe vision loss, frequently occurring in individuals 65 years or older, and is a well-recognized precursor to NVG. 3 Known systemic risk factors for CRVO include hypertension, diabetes mellitus, hyperlipidemia, and hypercoagulability as well as several ocular risk factors such as a history of glaucoma and ocular trauma.4,5 Advanced imaging modalities, including optical coherence tomography (OCT) and fluorescein angiography, have been shown to play a critical role in accurately localizing vascular occlusions, assessing retinal ischemia, and guiding clinical decision-making in patients with retinal vein occlusion (RVO). 6
Hyperlipidemia is a well-established systemic risk factor for both CRVO and branch retinal vein occlusion (BRVO). Multiple studies, including recent epidemiological and mechanistic investigations, support its role in the pathogenesis of retinal vascular occlusions through mechanisms such as endothelial dysfunction, increased blood viscosity, and systemic atherogenesis.7–10 Although these associations are supported by clinical and mechanistic data, a definitive causal link between hyperlipidemia and CRVO remains to be fully established.11–14
Here, we describe the case of a young man with no prior medical history, presenting with NVG secondary to CRVO, suspected to result from hyperlipidemia attributed to a restrictive, strictly nonvegetarian diet. This case highlights a potential gap in clinical practice guidelines for younger individuals presenting with CRVO and NVG without traditional vascular risk factors. The findings indicate that dietary-induced hyperlipidemia may be a modifiable risk factor contributing to retinal vascular disease in this population. Although this case supports the rationale for considering systemic lipid screening and dietary assessment, further studies are necessary to establish causality and inform evidence-based screening and management protocols.
Methods
This case report adheres to the Case Report (CARE) guidelines 15 to ensure thorough and transparent reporting. All patient data were obtained through retrospective analysis of clinical records, ophthalmologic examinations, laboratory investigations, imaging findings, and treatment outcomes. The CARE checklist was completed and is included as supplementary research data with this manuscript. Informed consent was obtained from the patient before publication of the manuscript.
Case presentation
A male patient in his 30s with no prior ocular, medical, or family history presented to the emergency department of the Alamance Regional Medical Center in October 2021 with a 5-day history of severe pain, redness, and progressive vision loss in the left eye. Visual acuity was measured at 20/20 in the right eye and was limited to hand motion in the left eye, with markedly elevated IOPs of 23 mmHg and 66 mmHg, respectively. Examination revealed a relative afferent pupillary defect, conjunctival injection, extensive neovascularization of the iris and anterior chamber angle, peripheral anterior synechiae (360°), and angle closure on gonioscopy. Fundoscopic examination demonstrated vitreous hemorrhage, optic disc edema, widespread retinal hemorrhages in all four quadrants, cotton wool spots, and tortuous veins, findings consistent with CRVO (Figure 1(a)).

Ultra-widefield color fundus photographs of the left eye. (a) At initial presentation, the fundus examination demonstrated extensive retinal hemorrhages and microaneurysms. (b) One year later, fundus examination demonstrated complete, 360° panretinal photocoagulation and the absence of vitreous hemorrhage or neovascular changes.
Initial management involved maximal medical therapy (topical timolol 0.5%, brimonidine 0.2%, dorzolamide 2%, and oral acetazolamide 250 mg four times daily prior to surgical intervention) to control IOP, anterior chamber paracentesis, and intravitreal bevacizumab (1.25 mg) injection, resulting in an initial IOP reduction to 7 mmHg. An Ahmed glaucoma valve implantation was urgently performed. An OCT performed 2 weeks later revealed significant intraretinal fluid and dense vitreous hemorrhage in the left eye (Figure 2(a)). Subsequent systemic investigations, including complete blood count, chest X-ray, glycosylated hemoglobin, erythrocyte sedimentation rate, coagulation profile, and tests for autoimmune and hypercoagulable markers, were all within normal limits. However, his lipid profile results were significantly abnormal, showing elevated total cholesterol (359 mg/dL), triglyceride (313 mg/dL), low-density lipoprotein (248 mg/dL), and very low-density lipoprotein (63 mg/dL) levels. The patient reported following a strictly nonvegetarian diet, suggesting dietary hyperlipidemia as the underlying cause. Diagnostic challenges included differentiating dietary-induced hyperlipidemia from other systemic conditions owing to the patient's atypical demographic profile and the absence of classic vascular risk factors.
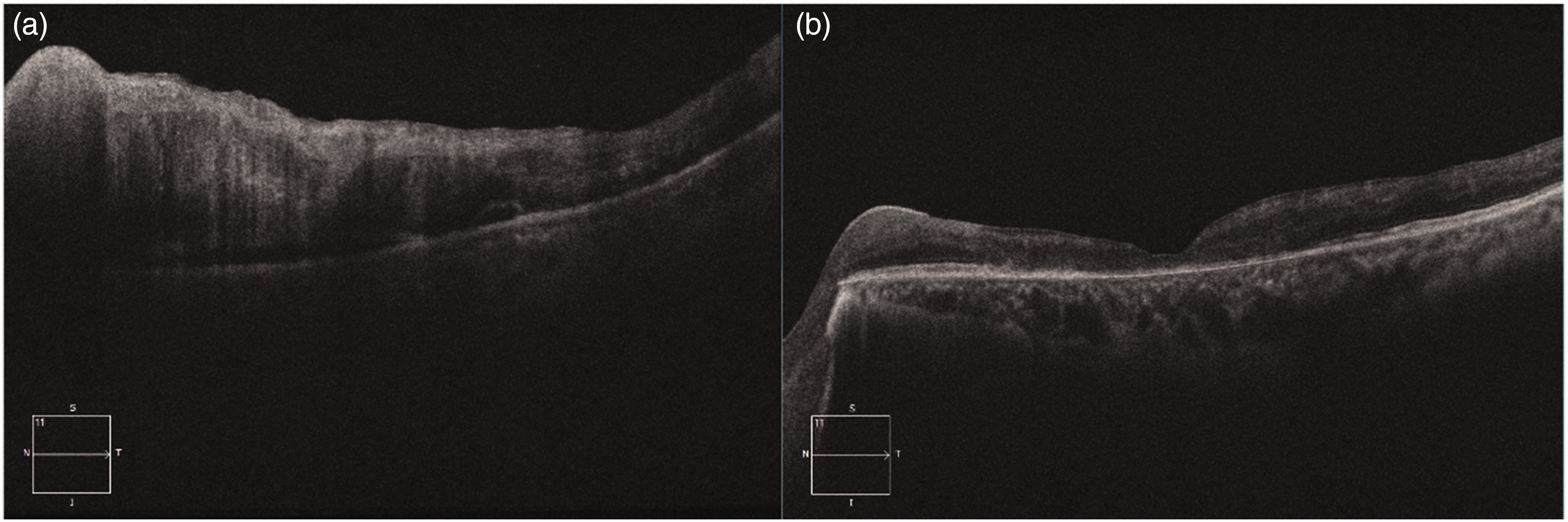
Optical coherence tomography (OCT) of the left eye. (a) Initial OCT at presentation showing marked intraretinal fluid and disorganization of the retinal layers with associated vitreous hemorrhage and (b) follow-up OCT at 12 months demonstrating resolution of intraretinal fluid and development of retinal atrophy.
The differential diagnosis initially included hypercoagulable states, systemic inflammatory vasculitis, and conditions such as systemic lupus erythematosus and sarcoidosis, all of which were ruled out by extensive laboratory testing. Given the absence of systemic disease, dietary hyperlipidemia was identified as the most probable cause of CRVO. The prognosis for visual recovery in patients with CRVO complicated by NVG remains guarded, and patients often require long-term multidisciplinary management to prevent recurrence and preserve their residual vision.
Ongoing ocular management consisted of monthly bevacizumab (1.25 mg/0.05 cc) injections and panretinal photocoagulation. One year later, following recurrence of dense vitreous hemorrhage, the patient underwent pars plana vitrectomy with endolaser treatment that successfully resolved hemorrhagic complications. The patient was followed up regularly over the course of 12 months with monthly evaluations, including IOP monitoring, fundus examinations, and OCT imaging. At the subsequent follow-up, visual acuity in the affected eye stabilized at counting fingers at 1 ft with an IOP of 23 mmHg. Fundus examination revealed effective panretinal photocoagulation without retinal neovascularization (Figure 1(b)). OCT revealed resolution of intraretinal fluid and subsequent retinal atrophy (Figure 2(b)). The patient's right eye remained unaffected, and systemic lipid-lowering therapy was initiated. Continued ophthalmologic and primary care follow-up demonstrated stable visual function with no further complications.
Discussion
CRVO typically affects individuals aged above 65 years and is usually accompanied with other systemic comorbidities, such as hypertension, diabetes mellitus, and hyperlipidemia. 4 The development of CRVO in a male in his 30s with sequelae of NVG is extremely unusual and necessitates investigation into other potential risk factors. In addition to systemic assessment, additional imaging tools such as OCT are indispensable for confirming the diagnosis and evaluating the extent of retinal involvement in CRVO. Munk et al. 6 have demonstrated how OCT imaging can delineate macular edema, venous congestion, and inner retinal thinning, features that inform both prognosis and therapeutic response. The existing literature addresses conventional risk factors that are commonly observed in older populations but does not address metabolic aberrations in younger patients. Although CRVO is less prevalent among younger populations, certain risk factors have been previously reported. A systematic analysis of the National Inpatient Sample database found primary open-angle glaucoma, retinal vasculitis, pseudotumor cerebri, hypercoagulable states, and history of deep vein thrombosis or pulmonary embolism as major risk factors for CRVO in the 18–40 years age group. 16 Importantly, classic risk factors such as hypertension and diabetes mellitus did not show a strong association with CRVO in this age group, whereas hyperlipidemia was the major risk factor. 16 These findings are consistent with a growing body of evidence supporting hyperlipidemia as a key modifiable risk factor in both CRVO and BRVO. Lam et al. 11 demonstrated significant associations between dyslipidemia and RVOs based on population-level data. More recent studies, including those by Garnavou-Xirou et al., 12 Voigt et al., 17 and Schreiberova et al., 14 confirm the contribution of elevated lipid levels toward retinal vascular occlusion risk, emphasizing the importance of lipid control in both primary and secondary prevention strategies.
In the present case, lipid screening revealed elevated total cholesterol and triglyceride levels, likely secondary to a highly restrictive and purely nonvegetarian diet. Further, hyperlipidemia is associated with the development of a prothrombotic state via mechanisms that involve elevated levels and activity of clotting factors VII, VIII, and X, and plasminogen activator inhibitor-1, all of which can lead to platelet aggregation and enhance blood viscosity. 18 All these alterations collectively heighten the risk for thrombosis, including RVO.
The patient’s highly restrictive diet, consisting solely of meat-based products could be the cause of the hypercholesterolemia and hypertriglyceridemia observed in the serum lipid profile results. A diet high in saturated fats and low in essential nutrients can lead to the hyperproduction of very-low-density lipoproteins and result in very high levels of triglycerides. 2 Elevated triglycerides can predispose patients to systemic vascular abnormalities and thrombosis. 8 Given the extreme nature of the patient's diet, we believe that the chronic effects of hyperlipidemic metabolism played a central role in CRVO development.
This case highlights a significant gap in the current clinical practice guidelines for the evaluation of young patients with CRVO. In the absence of established screening protocols for atypical presentations of CRVO in young patients, associated systemic conditions such as hyperlipidemia can remain undetected.
No routine lipid screening guidelines exist in young CRVO patients to date, although new evidence has implicated hyperlipidemia in retinal vascular occlusions. 3 Given the possibility of vision-threatening ocular sequelae such as NVG, the addition of lipid profile screening to commonly performed standard workups for hypercoagulable states may be appropriate in younger CRVO patients.
This case also underscores the emerging consideration for clinical practice that unconventional risk factors, such as diet-induced hyperlipidemia, may play a more prominent role in retinal vascular events among younger patients. Although current RVO workups focus on hypercoagulability, autoimmune disease, and hypertension, this report suggests that targeted metabolic screening, including lipid profile screening and dietary history, could help identify modifiable risk factors contributing to the condition. Incorporating these evaluations into the standard of care for atypical RVO cases may facilitate earlier intervention, reduce recurrence risk, and provide opportunities for preventive care through lifestyle or pharmacologic lipid management.
This case of CRVO and subsequent NVG in a young patient with hyperlipidemia highlights the potential role of lipid metabolism in retinal vascular disease. It suggests that hyperlipidemia may be a modifiable risk factor for CRVO even in the absence of other comorbidities. Given the risk of severe vision loss, lipid screening should be considered in young patients presenting with RVO. Further research is needed to clarify the mechanisms involved and to develop evidence-based screening and treatment guidelines.
The findings in this case may hold relevance for ophthalmologists globally because dietary patterns and lifestyle-driven metabolic diseases continue to rise in many countries. Although CRVO in younger adults remains rare, the increasing prevalence of hyperlipidemia in younger populations makes such presentations more likely to occur in the future across diverse geographic and socioeconomic settings. By drawing attention to a reversible and preventable systemic contributor, this case encourages a more comprehensive and multidisciplinary approach that can be applied globally.
Conclusion
This case highlights a critical gap in clinical practice guidelines for younger individuals presenting with CRVO and NVG without conventional vascular risk factors. The identification of diet-induced hyperlipidemia as a significant and modifiable risk factor emphasizes the need for routine, systemic lipid screening in young patients with atypical presentations of retinal vascular disease. Developing comprehensive guidelines for early recognition, screening, and multidisciplinary management in this demographic is essential to prevent severe visual impairment and systemic complications.
Footnotes
Acknowledgments
The authors thank the clinical staff involved in the patient's care and follow-up.
Author contributions
All authors contributed significantly to the conception, design, acquisition, analysis, and interpretation of data; drafting of the manuscript; and critical revisions. All authors approved the final manuscript version.
Data availability statement
All relevant data supporting the findings of this study are included within the manuscript.
Declaration of conflicting interests
The authors declare no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Ethics
This case report did not require IRB approval, as determined by the University of North Carolina Institutional Review Board (UNC IRB). Informed consent for publication was obtained from the patient. Written informed consent for publication of case details and accompanying images was obtained from the patient.
Financial support
None.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.