
Abstract
Objective
This study aimed to evaluate the effectiveness of biting on a cotton roll in reducing pain during metal bracket removal using a Weingart plier compared with the conventional method.
Methods
This two-arm, parallel-group, randomized controlled trial included 36 patients (11 males and 25 females) with a mean age of 20.5 ± 3.08 years (range: 16–25 years). The study was conducted among patients who had completed orthodontic treatment with a fixed appliance using MBT prescription 0.022-inch metal brackets featuring a single-mesh base (Pinnacle®, MBT compatible 0.022, OrthoTechnology™, Florida, USA), and they were referred for metal bracket debonding. Brackets were removed using a Weingart plier, and participants were randomly assigned to one of two groups: the open-mouth group and the biting-on-a-cotton-roll group. Pain intensity was assessed for each tooth using a visual analog scale (0–100 mm) immediately after each bracket removal. Pain levels were compared between the two groups, between the upper and lower jaws, and across sexes.
Results
Patients in both groups reported pain levels ranging from mild to mild–moderate, with lower mean pain levels observed in the biting-on-a-cotton-roll group compared with the open-mouth group. Significant differences in mean pain scores were found between the open-mouth group and biting-on-a-cotton-roll group in the upper and lower incisors (13.61 and 13.19, P < 0.001, respectively), upper and lower canines (4.03 and 3.61, P < 0.001, respectively), and upper and lower premolars (12.78 and 11.11, P < 0.001, respectively). No significant differences in pain perception were observed between males and females across all regions (P > 0.05).
Conclusions
Biting on a cotton roll significantly reduces pain during metal bracket debonding in the upper and lower incisor regions. The anterior regions of both jaws exhibit increased sensitivity to pain during the debonding procedure, whereas no differences in pain perception were observed between male and female patients.
Introduction
Debonding the orthodontic brackets at the end of treatment involves removing all parts of the appliance and the remaining adhesive material. It aims to restore the tooth surface to its initial state before the brackets. 1 Therefore, correct adhesive and removal processes are necessary. 1 Although debonding is a necessary step in orthodontic treatment, it may also contribute to one of its most common side effects—pain.
Orthodontic pain is considered one of the unpleasant side effects that may occur during orthodontic treatment. 2 Additionally, 95% of orthodontic patients expressed mild-to-severe pain and discomfort during or after applying various orthodontic treatment procedures, which may lead patients to withdraw from treatment and not complete it. Orthodontic procedures that may cause pain include applying separation elastics,3–5 inserting orthodontic mini-implants, 6 activating wires to induce different orthodontic tooth movements, 7 expanding the upper-dental arch, 8 using a removable appliance, 9 and debonding orthodontic appliances.
The debonding procedure should be safe, painless, and efficient. 10 Pain may be affected by many factors, such as the patient’s psychological state and previous experiences, cultural background, the patient’s sex, consuming systemic medications, the condition of the periodontal tissue as well as the type and location of the tooth, and the patient’s expectations about pain in addition to age. 11
Pain experienced during debonding brackets is significantly influenced by the orientation of the applied force and the mobility of the teeth; during the debonding of brackets, the teeth are more tolerant of intrusive vertical forces and more sensitive to extrusive vertical forces, and the more stable the tooth is during debonding brackets, the less pain. 12
Many studies have evaluated different procedures for debonding brackets, such as mechanical methods using cutters and removing pliers,13,14 the use of ultrasound waves, 15 the application of lasers, 16 and electrical and thermal methods. 17 Several methods have been used to control the possible pain associated with metal bracket deboning. 18 These methods include using pain-relieving medications10,19; applying finger pressure10,20,21; biting on a cotton roll 12 ; biting on a chewing material 22 ; or using a wax template, 19 acrylic wafer,11,19 elastomeric wafer, 20 and plastic wafer. 21
A pilot study confirms the need to apply finger pressure or instruct the patient to firmly bite into a cotton roll to provide an intrusive, stabilizing force during bracket removal. 12 A prospective split-mouth study investigated the effectiveness of bracket remover and a Weingart plier in combination with biting on a cotton roll in metal brackets debonding and found no clinical difference between the two pliers. 23
When reviewing the literature, two recent studies focused on biting on a cotton roll during debonding. The first study compared this method with high-frequency vibration and elastomeric wafers during metal bracket debonding, concluding that biting on a cotton roll effectively reduced pain during debonding but was less effective than the high-frequency vibration. 24 The second study compared biting on a cotton roll with traditional debonding in a split-mouth design using a bracket remover plier, determining that biting on a cotton roll was ineffective in reducing pain during the debonding process. 25 Both studies used a bracket remover plier for debonding, and no study has evaluated the effect of biting on a cotton roll for reducing pain when debonding metal brackets with a Weingart plier.
Jeha and Haddad, 26 in a systematic review, highlighted the inadequate documentation of the pain and discomfort associated with bracket removal. They confirmed the need for more clinical trials. In addition, this systematic review and another one 2 did not include any study about the effectiveness of biting on a cotton roll during the removal of brackets. However, previous studies have yielded mixed findings on the effectiveness of biting on a cotton roll in managing pain during the debonding of metal brackets.
The objective of this study was to evaluate the effectiveness of biting on a cotton roll when removing metal brackets using a Weingart plier compared with the conventional method in reducing pain associated with metal bracket debonding.
Materials and methods
Study design, registration, and settings
This study was designed as a double-blinded, two-arm randomized controlled trial. The patients were unaware of their group allocation and remained blinded during bracket removal. In addition, the data analysis was carried out by a statistician who was also not informed of the group assignments. The protocol of this trial was registered in the clinical trials database (Registration number: NCT06873503). This study was conducted at the Department of Orthodontics, Faculty of Dentistry, the University of Damascus, Syria, and was funded by Damascus University (Ref No: 501100020595). This study was conducted by the principles of the Declaration of Helsinki (1975, as revised in 2024). Informed consent was obtained from all patients before their participation, and ethical approval was obtained from the Biomedical Research Ethics Committee at Damascus University (DN-180225-420). The patients included in this study did not participate in the design, implementation, or writing of the article.
Estimation of the sample size
The G*Power software (version 3.1.3 Universität Düsseldorf, Düsseldorf, Germany) was used to calculate the required sample size. The calculation was performed considering the results of a previous study, 27 which reported a mean visual analog scale (VAS) of 8.25 (SD = 4.78) for the test group and 4.20 (SD = 2.91) for a control group, a significance level of 0.05, and a power of 90%. This calculation indicated a necessity of 18 patients per group, and 36 patients were included in the study.
Patient recruitment and entry in this trial
The sample included patients who underwent planned orthodontic treatment performed by three fourth-year resident orthodontists in the Department of Orthodontics at the Faculty of Dentistry (University of Damascus). After ensuring that orthodontic treatment was completed, they were referred for the removal of metal brackets according to the current study between May 2024 and January 2025.
Inclusion criteria for the patients were as follows: (a) being aged 16 to 25 years, and being in good mental and physical health; (b) undergoing orthodontic treatment with MBT prescription 0.022-inch metal brackets with a single-mesh base (Pinnacle®, MBT compatible 0.022, OrthoTechnology™, Florida, USA) who were in the final stage of their treatment and planned for debonding; (c) having brackets bonded with the same bonding cement (Ivoclar Heliosit Orthodontic Adhesive Composite), the same primer (Ivoclar Vivadent Tetric N-Bond), and the same curing time, as well as the curing light device; (d) the absence of lost brackets at the debonding process; (e) having 0.017 × 0.025-inch stainless-steel finishing archwires in their places for at least 1 month; (f) having good occlusal relationships and strong intercuspation; (g) having no recent use of medications such as painkillers or corticosteroids on the last day; (h) the absence of acute or chronic dental pain induced by periodontal/periapical lesions or caries; (i) the absence of a history of surgical treatment, including impacted tooth eruption, tooth transplantation, or the presence of mini-screws; and (j) the absence of craniofacial deformities. All participants received an information sheet and provided informed consent before their recruitment. The reporting of this study conforms to the Consolidated Standards of Reporting Trials (CONSORT) statement. 28 Figure 1 illustrates the CONSORT flow diagram for patient enrollment.

The CONSORT flow diagram of patients’ recruitment, follow-up, and entry into data analysis.
Randomization and allocation concealment
After finishing the orthodontic treatment, patients were distributed randomly into groups through the block randomization method. A randomized patient list was created using Minitab® by an MSc student from the Department of Orthodontics, who had no involvement in this study. Patients were randomly allocated to six permuted blocks (with each block comprising six patients, including three from each group) in a 1:1 ratio to one of the two groups: the first group, the open-mouth group (OMG), and the second group, the biting-on-a-cotton-roll group (BCRG). Each patient received a serial number, and their allocation was hidden from the researcher to prevent selection bias. Patient names and group assignments were placed in closed opaque envelopes and only opened during the debonding stage of the metal brackets.
Each patient picked an envelope, and the intervention they received was determined according to its contents.
Interventions
Deboning in the OMG
The debonding procedure was conducted by the principal researcher (B.A.D.) using the open-mouth technique. All brackets were removed using a Weingart plier (American Orthodontics, Sheboygan, Wisconsin, USA) and squeezed from both sides of the mesial-distal surfaces (Figure 2). Before debonding, the stainless-steel finishing archwires (0.017 × 0.025-inch) were removed.

Debonding metal brackets in the open-mouth group.
Debonding in the BCRG
All brackets were removed by the same principal researcher (B.A.D.), and debonding was performed using a Weingart plier (American Orthodontics, Sheboygan, Wisconsin, USA), by squeezing them from both sides of the mesial-distal surfaces. Additionally, cotton rolls were placed between the upper and lower teeth, and the patients were instructed to bite on them during the procedure (Figure 3). Before debonding, the stainless-steel finishing archwires (0.017 ×0.025-inch) were removed. Patients in the second group were instructed to bite on a cotton roll throughout the debonding process. Brackets were then removed one at a time in both groups, in sequence from the upper right to the upper left and from the lower right to the lower left, with the central incisor bracket being the first to be removed in each quadrant. All bracket removals were performed using a right-handed technique.

Debonding metal brackets in the biting-on-a-cotton-roll group.
Outcome measures: perceived pain intensity
Pain intensity was effectively gauged using a 100-mm VAS, in which a score of zero indicated “no pain,” with increasing scores reflecting greater pain levels. Patients were tasked with recording their pain scores on the scale immediately after each bracket removal, ensuring accurate record-keeping before moving on to the next tooth. Before debonding, every patient was informed about the study’s objectives and instructed to evaluate the pain intensity of the procedure with a VAS after the debonding was completed. The VAS scores for the upper and lower jaws were meticulously tabulated, considering the comprehensive assessment and the specific evaluation within each region (incisors, canines, and posterior regions). In order to minimize bias, the VAS scores were evaluated by an independent orthodontist who had no prior knowledge of the group assignments.
Statistical analysis
The SPSS program (version 25.0; IBM, Armonk, New York, USA) was used for statistical analysis. The Shapiro-Wilk test was conducted to assess data normality, which indicated a non-normal distribution. As a result, the Mann–Whitney U test was employed to compare VAS pain scores between the two groups, whereas the Wilcoxon signed ranks test was used to compare VAS scores within each group. The chi-square test was used to detect significant differences in sex and extraction between the study groups. The Mann–Whitney U test was used to detect significant differences in VAS scores between males and females. A significance level of 0.05 was used.
Results
Baseline sample characteristics
The sample consisted of 36 patients (11 men and 25 women) with a mean age of 20.5 ± 3.08 years (16–25 years); tooth extraction was performed in 47.2% of the patients.
Age, sex, and extraction did not significantly differ between the two groups (P = 0.717, P = 0.346, P = 0.738, respectively). The baseline sample characteristics related to sex, age, and extraction are shown in Table 1. Descriptive statistics about VAS pain scores for each tooth and each region are given in Table 2.
Baseline sample characteristics.

n: number of patients.
Chi-square test.
Mann–Whitney test.
Descriptive statistics of pain perception using the visual analog scale for each tooth and each region.

1: central incisor; 2: lateral incisor; 3: canine; 4: first premolar; 5: second premolar; Min: minimum; Max: maximum; L: lower tooth; U: upper tooth.
Comparisons of pain levels between the two groups
Patients in both groups experienced mild or mild-to-moderate pain, with lower mean pain levels in the BCRG than the OMG across all regions. The greatest mean pain values were recorded in the lower incisor region (
Descriptive statistics of debonding pain scores for the incisor, canine, and premolar regions in each jaw across both groups, along with P values of significance testing between the two groups and between males and females.
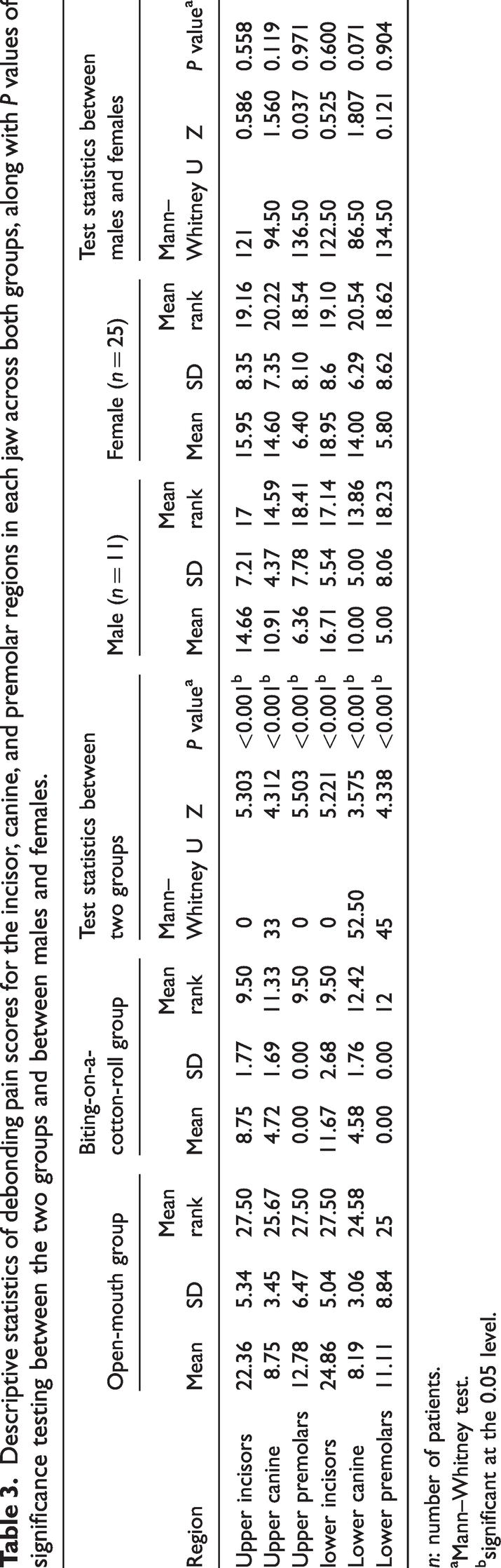
n: number of patients.
Mann–Whitney test.
significant at the 0.05 level.

A bar chart illustrating pain scores for the different regions in both groups.
Comparisons of pain levels within each group
Comparisons of pain levels between the right and left sides
In the OMG, greater mean pain levels were reported in the lower incisor region on the left side (
Descriptive statistics of debonding pain scores for the right and left sides for each quadrant in both groups along with the P values of significance testing between the two sides.
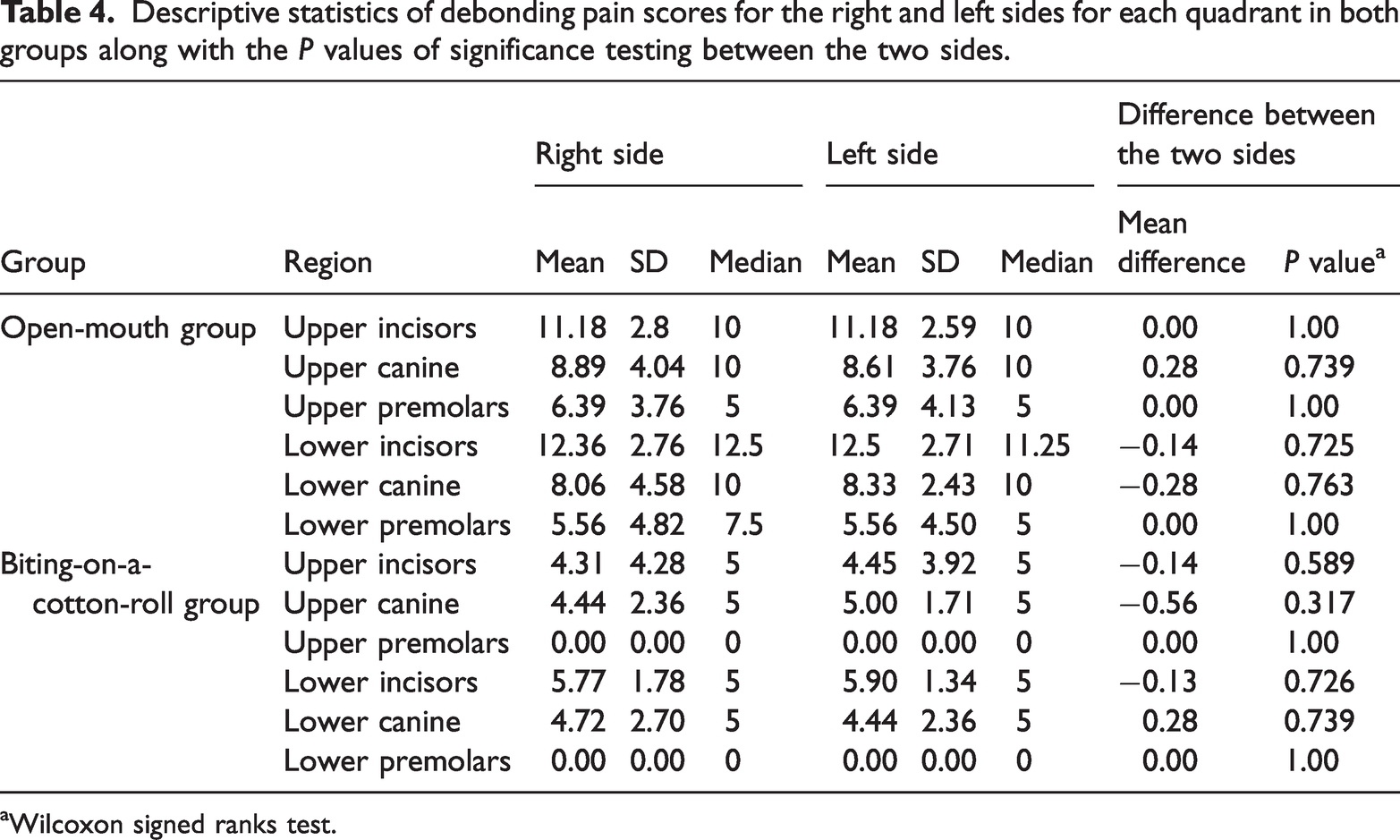
Wilcoxon signed ranks test.
Comparisons of pain levels between the incisors and premolar regions
In the OMG, the greater mean pain values were recorded in the upper and lower incisors regions (
Comparison of debonding pain scores across different tooth regions and both jaws in the two study groups.

Wilcoxon signed ranks test.
significant at the 0.05 level.
Comparisons of pain levels between the maxillary and mandibular regions
Patients in the OMG reported mild-to-moderate pain in the incisor regions, with mean values of 24.86 ± 5.04 in the lower incisor region and 22.36 ± 5.34 in the upper-anterior region. Mild pain was also recorded in the canine regions (
Effect of sex on pain levels
Females reported greater mean pain in the lower incisor region (
Discussion
Pain is a subjective experience that can vary widely among individuals. This variation is influenced by several factors, including age, sex, personal pain threshold, psychological and social conditions, past negative experiences, and the degree of force applied. Recognizing these differences is essential for effective pain assessment and management strategies.19,20,30
Although various methods for bracket debonding, such as ultrasonic instrumentation, lasers, and electro-thermal debonding, are documented in the literature,14,19 hand tools like Weingart pliers remain among the most practical solutions. 23 This study used Weingart pliers to compare the pain scores in two techniques—open mouth and biting on a cotton roll—during bracket removal. These methods are widely used in orthodontic clinics and are readily available to orthodontists. Therefore, this study aimed to investigate the effectiveness of biting on a cotton roll for pain management during metal bracket debonding and the effects of anatomical location and sex on pain scores.
The first study on pain associated with bracket debonding was a pilot study conducted by Williams and Bishara. 12 They found that patients can tolerate intrusive forces. They noted that biting on a cotton roll provides a stabilizing force, which may reduce pain during the debonding process. In another study by Kilinç and Sayar, 19 soft wax and acrylic bite wafers were used to prevent extrusive forces during debonding.
The intergroup comparison revealed that the highest pain values were observed in the OMG compared with the BCRG across all regions, especially in the upper and lower incisor regions where the difference was clinically significant. In the rest of the regions, although the difference was statistically significant, it was not clinically significant. This indicates that the effectiveness of biting on a cotton roll in pain management was associated with metal brackets debonding in the region of the incisors. This finding is consistent with the research conducted by Musawi and Kadhum, 24 which demonstrated that biting on a cotton roll during bracket removal effectively reduced associated pain. Although a different instrument was used for debonding, the median pain score in the lower anterior region was 35 in the OMG and 25 in BCRG, whereas in the current study, the median was 23.75 in OMG and 10 in BCRG. Similarly, Thakkar et al. 22 found that removing brackets while biting on a chewie significantly decreased the pain levels of the patient compared with the OMG. However, these results contrast with those of Celebi, 25 who reported that biting on a cotton roll did not alleviate pain during bracket removal in all regions. The discrepancy might stem from the use of the split-mouth design in that study; the design used in that study raises concerns about possible carry-over effects, as pain in the orofacial region, particularly dental pain, can radiate from one side of the oral cavity to the other or even to various parts of the orofacial area. As a result, it becomes difficult for patients to evaluate the precision of their pain. 31 In addition to the variation in tools used for bracket removal, a bracket remover plier was used in their study; this tool exerts a symmetrical bilateral force on the bracket wings, concentrating on a smaller area of force application compared with the Weingart plier. This aligns with the findings of Bishara and Fehr, 32 who highlight that a reduction in the contact surface between the tool head and the bracket leads to a decrease in the force applied.
In this study, debonding began from the upper right, moved to the upper left and lower right, and concluded with the lower left quadrants. Mangnall et al. 11 suggested that the initial quadrant debond could be more painful. However, in the current study, there was no difference in pain perception between the right and left sides in both regions of the group.
The intragroup comparison revealed that tooth location significantly affected pain perception. Bavbek et al. 20 found that upper and lower anterior teeth are more pain-sensitive than posterior teeth, whereas Nakada et al. 30 noted greater pain in the upper and lower anterior segments compared with the posterior segments. In this study, lower incisors had the highest pain scores among all evaluated teeth, consistent with previous studies.10,11,13,19,20 This observation may be attributed to the relatively small root surface area of the lower incisors, leading to a higher force concentration per unit area during the debonding process. This increased pressure is likely to enhance sensitivity and pain perception in these teeth compared with those with larger root surfaces.
Mangnall et al. 11 observed elevated pain levels in the upper right posterior segment in 18% of patients. In contrast, the present study recorded only mild pain in the OMG and no pain in the BCRG in the posterior region. This disparity may be attributed to the upper right posterior segment being the first sextant debonded in their study, possibly heightening the participants’ perception of pain. Additionally, differences in pain management methods, such as using a soft acrylic wafer, could also have contributed to this variation.
In addition to the anatomical location of the tooth affecting pain levels, sex differences also play a role in the intensity of pain during the debonding process.10,19,20 It was found that females tend to have a lower pain threshold compared with males. 33 Additionally, the intensity of pain perception can vary based on the patient’s sex. 34 However, the present study found no notable differences in pain levels between males and female participants; this result agreed with the results of the studies of Iqbal et al., 21 Musawi and Kadhum, 24 and Karobari et al. 35 This finding also aligns with the study by Williams and Bishara, 12 who highlighted that sex differences have minimal impact on pain. Furthermore, Koyama et al. 36 observed that subjective pain experiences are influenced more by expectations, as these can alter brain mechanisms. In essence, positive expectations can lead to a reduced perception of pain.
Limitations
This study evaluated the pain associated with metal brackets debonding using Weingart pliers and biting on a cotton roll. However, several significant variables were not explored. Future studies should investigate aspects such as evaluating adhesive remnants on teeth and potential enamel damage. Another limitation of the study was focusing on pain levels in the incisor, canine, and premolar regions without assessing the molar region because of the variations in molar attachments, which depend on individual treatment needs and orthodontists’ preferences. Another limitation of this study was that it exclusively focused on patients aged 16 to 25 years, excluding other age groups. In addition, it did not include the use of the Pain Catastrophizing Scale to assess the patient’s psychological state to filter out those not suitable for inclusion. Furthermore, sex-specific subgroup analysis was not considered in the sample size calculation, which may reduce the statistical power of post-hoc analysis and increase the risk of type II errors.
Generalizability
The findings of this study, conducted with a sample of adult patients and minimizing bias, suggest that this technique could be a useful addition to orthodontic debonding protocols. However, the applicability of these results may be constrained by factors such as the unique traits of the study population, the clinical environment, and the specific methodologies employed. Further research involving diverse populations and varying clinical settings is recommended to verify the broader relevance of these findings and develop standardized protocols for using Weingart pliers with biting on a cotton roll in metal bracket debonding.
Conclusion
Biting on cotton significantly alleviates pain during metal bracket debonding in all regions, with clinically significant efficacy in the upper and lower incisor regions. Pain levels during the debonding of metal brackets were higher in the incisor region compared with the premolar region in both jaws, with the lower incisors being the most painful. Both jaws showed no difference in pain perception between the right and left sides. Male and female patients exhibit no disparity in pain perception.
Footnotes
Acknowledgments
Not applicable.
Authors’ contributions
Belal A Drmch: The principal researcher recruited patients, performed clinical procedures, collected questionnaires, analyzed the data, interpreted the results, and wrote the initial drafts of this paper. Kinda Sultan supervised the whole research project, helped in data analysis and interpretation of the results, and corrected the early drafts of this manuscript. Mohammad Y Hajeer and Ahamd Burhan co-supervised this project, helped in statistical analysis, and participated in writing this manuscript. The manuscript was read and approved in its final form by all authors. Shadi Azzawi participated in the inception of this work and study design, assisted in data analysis and interpretation, edited the final drafts of this manuscript. All authors read and approved the final version of this manuscript.
Availability of data and materials
Data concerning the current study can be obtained from the corresponding author upon reasonable request.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors have confirmed that there are no conflicts of interest related to the submitted manuscript.
Ethics approval and consent to participate
This project was approved by the Biomedical Research Committee at the University of Damasucs (Reference number: DN-180225-420).
Funding
This research work was financially supported by the University of Damascus (Ref No: 501100020595).