
Abstract
Objective
Anemia is the most common complication in patients with adult primary nephrotic syndrome. However, research on anemia in patients with adult primary nephrotic syndrome is limited. Our study aimed to explore the clinical characteristics and relevant factors of anemia in patients with adult primary nephrotic syndrome.
Methods
In total, 150 patients with primary nephrotic syndrome, who were followed up in the nephrology department of Hebei General Hospital from 2018 to 2021, were included. The patients were divided into baseline anemia and baseline no anemia groups. The clinicopathologic indices of anemia between the two groups were compared for screening the independent risk factors for anemia.
Results
Of the 150 patients with primary nephrotic syndrome, 34 had anemia, including 31 (20.67%) with mild anemia, 3 (2.00%) with moderate anemia, 25 (16.67%) with normocytic anemia, 3 (2.00%) with simple microcytic anemia, and 6 (4.00%) with microcytic hypochromic anemia. Diastolic blood pressure, albumin level, prealbumin level, estimated glomerular filtration rate, total cholesterol, triglyceride level, and habitual alcohol consumption were lower in the baseline anemia group than in the other group (p < 0.05). The results demonstrated that albumin level (odds ratio = 0.838, 95% confidence interval: 0.713–0.986, p = 0.033), prealbumin level (odds ratio = 0.838, 95% confidence interval: 0.722–0.966, p = 0.015), total cholesterol (odds ratio = 0.544, 95% confidence interval: 0.399–0.742, p < 0.001), and habitual alcohol consumption (odds ratio = 0.119, 95% confidence interval: 0.019–0.740, p = 0.022) were independent risk factors for baseline anemia in patients with primary nephrotic syndrome.
Conclusion
Patients with adult primary nephrotic syndrome have a high prevalence of comorbid anemia, mainly mild anemia and normocytic anemia. Reduced albumin, prealbumin, and total cholesterol and the absence of habitual alcohol consumption were independent risk factors for baseline anemia in patients with adult primary nephrotic syndrome.
Introduction
Nephrotic syndrome (NS) is a group of clinical syndromes characterized by the impaired barrier function of the glomerular filtration membrane and increased permeability of the basement membrane, which leads to the development of massive proteinuria, hypoproteinemia, edema, and hyperlipidemia. NS can be categorized into primary, secondary, and hereditary, depending on the etiology of the disease. Primary nephrotic syndrome (PNS) manifests in different types of pathological changes, mainly including membranous nephropathy (MN), minimal change disease (MCD), and focal segmental glomerulosclerosis (FSGS).1,2
In patients with NS, in addition to albumin (ALB), there is a loss of many other types of proteins, particularly binding proteins, in the urine.1,2 Therefore, the plasma levels of iron, vitamin D, hormone-binding proteins, lipoproteins, coagulation factors, erythropoietin, and transferrin may be lower in patients with NS than in healthy individuals. Hence, the liver stimulates the nonselective synthesis of proteins to balance these losses, 3 leading to the development of a range of complications, including hyperlipidemia, infections, thromboembolic events, acute kidney injury, endocrine disruption, and anemia.4,5
Anemia is the most common hematologic complication in patients with chronic kidney disease (CKD), which is associated with decreased quality of life and an increased risk of cardiovascular events, hospitalization, and mortality.6–11 Therefore, early attention to the anemia status of patients with kidney disease is of great importance. However, most domestic and international studies on anemia in kidney disease are limited to patients with CKD stage 3–5 with reduced renal function. There are some studies on the clinical characteristics of anemia in patients with immunoglobulin A (IgA) nephropathy and diabetic nephropathy.12–15 However, most studies on anemia in patients with PNS are focused on pediatric patients.16–19 In addition, there is limited research revealing the association between disease progression and anemia in adult PNS patients who do not have severely reduced renal function. Therefore, our study aimed to explore the prevalence of anemia, type of anemia, and the factors affecting anemia in PNS patients for a theoretical reference for clinical intervention.
Materials and methods
Research objectives and methodology
The data of 150 inpatients with clinical and renal biopsy-proven PNS in Hebei General Hospital from 2018 to 2021 were reviewed retrospectively in this research. We have de-identified all patient details. The study was approved by the Ethics Committee of Hebei General Hospital (NO. 2023097). The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013.
General data of patients at the time of PNS diagnosis were collected, including name, sex, age, systolic blood pressure, diastolic blood pressure, height, weight, clinical manifestations, history (whether there was any combination of hypertension or type 2 diabetes mellitus in the past), and personal history (habitual alcohol consumption and smoking). The relevant clinical laboratory data were collected, including red blood cell (RBC) count and mean corpuscular volume (MCV) as well as the levels of hemoglobin (Hb), hematocrit (HCT), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), platelet (PLT), albumin (ALB), prealbumin (PALB), total cholesterol (TC), triglyceride (TG), blood urea nitrogen (BUN), serum creatinine (Scr), estimated glomerular filtration rate (eGFR), uric acid (UA), and 24-h proteinuria. All clinical indicators were tested in the laboratory of Hebei General Hospital. Pathological data of renal biopsy were collected. Patients were divided into the baseline anemia group and baseline no anemia group based on whether they were anemic at the time of first diagnosis. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 20
Inclusion and exclusion criteria
Inclusion criteria
The inclusion criteria were as follows: (a) patients met the clinical diagnostic criteria for NS; (b) MN, MCD, and FSGS were confirmed via renal puncture biopsy; (c) aged 18–80 years; (d) eGFR (CKD-EPI formula) ≥60 mL/min/1.73 m2; and (e) availability of complete clinical and laboratory data required for this study.
Exclusion criteria
The exclusion criteria were as follows: (a) NS with clear secondary causes, including tumor, systemic lupus erythematosus, Sjogren syndrome, anaphylactic purpura, hepatitis B and C viral infections, and heavy metal poisoning; (b) the existence of hematological disorders such as hemolytic anemia, aplastic anemia, and leukemia; (c) combined with diabetic nephropathy, IgA nephropathy, and other renal diseases; (d) combination of severe infections, malignant tumors, active bleeding, and other diseases that may lead to anemia; and (e) pregnant and lactating women.
Diagnostic criteria
Diagnostic criteria for NS
The diagnostic criteria for NS refer to the clinical diagnostic criteria for PNS described in the 2011 Expert Consensus on the Treatment of Primary Nephrotic Syndrome in Adults, 21 which were as follows: (a) massive proteinuria: 24-h proteinuria >3.5 g/day; (b) hypoalbuminemia: plasma ALB <30 g/L; (c) hyperlipidemia; and (d) edema. Of the above criteria, the first two are necessary for diagnosis.
Diagnostic criteria for anemia
According to the Chinese Clinical Practice Guidelines for the Diagnosis and Treatment of Anemia, the diagnostic criteria for anemia were as follows: 22 Hb <130 g/L in adult men and Hb <120 g/L in nonpregnant adult women. The cytomorphological classification and severity criteria for anemia are presented in an additional document (Supplemental Table 1, Supplemental Table 2). 23
Statistical analysis
SPSS 26.0 software package was used to analyze all data. Normally distributed variables were expressed as mean ± SD, and t test was applied for comparison of differences between the two groups. The non-normally distributed variables were expressed as median and interquartile range (M(25th quartile, 75th quartile)), and the Wilcoxon–Mann–Whitney nonparametric test was applied. Count data were described as frequencies and percentages (%), and the chi-square test was applied for comparison of differences between the two groups. Spearman correlation analysis was performed to analyze the bivariate correlation of baseline Hb levels. A one-way logistic regression model was applied to calculate the odds ratio (OR). Statistically significant parameters (p < 0.10) were included in the multivariable logistic regression model for assessing the independent risk factors for baseline anemia in patients with PNS. All statistical analysis data were two-tailed, and the level of statistical significance was set at 0.05.
Results
Characteristics of the participants
Among the 150 patients with PNS, 88 (58.67%) were male and 62 (41.33%) were female. There were 115 patients with MN, of whom 26 (22.61%) were anemic at the time of diagnosis. There were 32 patients with biopsy-proven MCD, of whom 6 (18.75%) were anemic at the time of diagnosis. Three patients were diagnosed with FSGS, of whom two (66.67%) were anemic. Among the 34 patients with comorbid baseline anemia, 25 (16.67%) had normocytic anemia, 3 (2.00%) had simple microcytic anemia, 6 (4.00%) had microcytic hypochromic anemia, and no patients had macrocytic anemia (Table 1).
Clinical features of the participants.

ALB: albumin; BMI: body mass index; BUN: blood urea nitrogen; eGFR: estimated glomerular filtration rate; Hb: hemoglobin; HCT: hematocrit; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; MCV: mean corpuscular volume; PALB: prealbumin; PLT: platelet; RBC: red blood cell count; Scr: serum creatinine; TC: total cholesterol; TG triglyceride; UA: uric acid.
Comparison of clinical data between the two groups
In this study, the patients were grouped by whether they were comorbid with anemia at the time of PNS diagnosis. Our results revealed that age (p = 0.022) and 24-h proteinuria (p = 0.013) in the baseline anemia group were significantly higher than those in the baseline no anemia group (group 1). However, the diastolic blood pressure (p = 0.038), ALB level (p < 0.001), PALB level (p < 0.001), eGFR (p = 0.011), TC (p < 0.001), TG level (p < 0.001), and habitual alcohol consumption (p = 0.039) were lower in the baseline anemia group. There was no significant difference in terms of sex, systolic blood pressure, BMI, fasting glucose level, BUN level, Scr level, UA, hypertension, type 2 diabetes mellitus, and habitual smoking between the two groups (p > 0.05; Table 2).
Comparison of baseline information between the two groups.

ALB: albumin; BMI: body mass index; BUN: blood urea nitrogen; eGFR: estimated glomerular filtration rate; Hb: hemoglobin; HCT: hematocrit; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; MCV: mean corpuscular volume; PALB: prealbumin; PLT: platelet; RBC: red blood cell count; Scr: serum creatinine; TC: total cholesterol; TG triglyceride; UA: uric acid.
Correlation between anemia and clinical parameters
Spearman’s rank correlation analysis revealed that the baseline levels of Hb were negatively correlated with age (r = −0.231, p = 0.004) and 24-h proteinuria (r = −0.290, p < 0.001) and positively correlated with diastolic blood pressure (r = 0.297, p < 0.001), BMI (r = 0.291, p < 0.001), ALB level (r = 0.415, p < 0.001), PALB level (r = 0.292, p < 0.001), Scr level (r = 0.265, p = 0.001), and UA level (r = 0.341, p < 0.001). The levels of systolic blood pressure, fasting blood glucose, BUN, eGFR, TC, and TG were not significantly correlated with Hb levels in PNS patients (p > 0.05; Table 3; Figure 1).
Correlation of hemoglobin with clinical indicators.

ALB: albumin; BMI: body mass index; BUN: blood urea nitrogen; eGFR: estimated glomerular filtration rate; PALB: prealbumin; Scr: serum creatinine; TC: total cholesterol; TG triglyceride; UA: uric acid.

Correlation between hemoglobin and clinical parameters.
Univariate logistic regression analysis of baseline anemia in patients with PNS
Univariate logistic regression analysis revealed that advanced age, absence of habitual alcohol consumption, low diastolic blood pressure, low ALB level, low PALB level, low eGFR, low TC, and low TG level were the risk factors for the development of anemia in patients with PNS (Table 4).
Univariate logistic regression analysis of baseline anemia in patients with PNS.

ALB: albumin; BMI: body mass index; BUN: blood urea nitrogen; CI: confidence interval; eGFR: estimated glomerular filtration rate; PALB: prealbumin; PNS: primary nephrotic syndrome; OR: odds ratio; Scr: serum creatinine; SE: standard error; TC: total cholesterol; TG triglyceride; UA: uric acid.
B represents the regression coefficient, indicating the change in the dependent variable when the independent variable increases by one unit while keeping other independent variables constant.
SE reflects the accuracy of the B estimate.
Multivariable logistic regression analysis of baseline anemia in patients with PNS
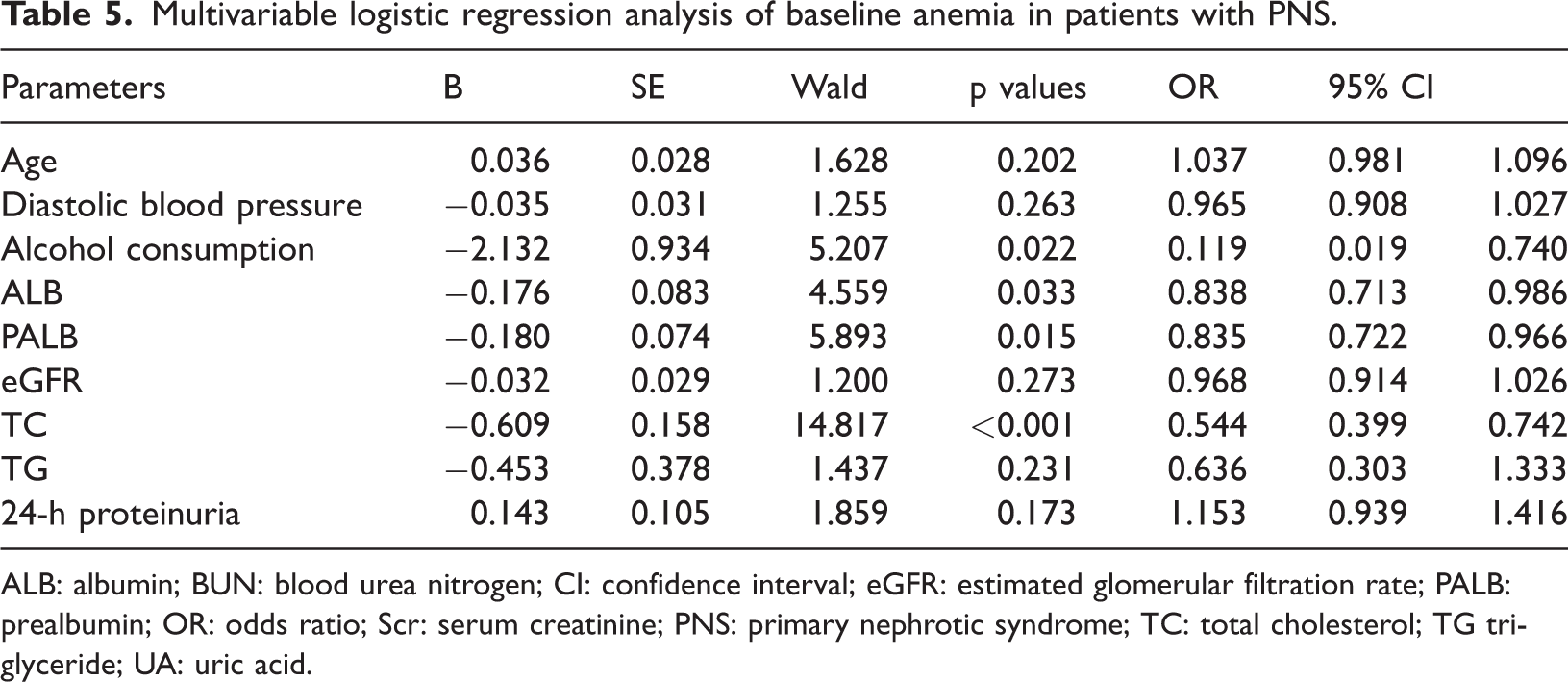
Variables with p < 0.1 in the univariate logistic regression analysis were included as independent variables in the multivariable logistic regression analysis. The included factors were age, diastolic blood pressure, habitual alcohol consumption, ALB level, PALB level, eGFR, TC, TG level, and 24-h proteinuria. The results revealed that ALB level, PALB level, TC, and habitual alcohol consumption were independent risk factors for baseline anemia in patients with PNS (p < 0.05). Decreased ALB level (OR = 0.838, 95% confidence interval (CI): 0.713–0.986, p = 0.033), PALB level (OR = 0.838, 95% CI: 0.722–0.966, p = 0.015), and TC (OR = 0.544, 95% CI: 0.399–0.742, p < 0.001) increased the risk of anemia in patients with PNS. The difference was statistically significant. PNS patients without habitual alcohol consumption had a significantly higher risk of anemia than those with habitual alcohol consumption (OR = 0.119, 95% CI: 0.019–0.740, p = 0.022; Table 5).
Multivariable logistic regression analysis of baseline anemia in patients with PNS.
ALB: albumin; BUN: blood urea nitrogen; CI: confidence interval; eGFR: estimated glomerular filtration rate; PALB: prealbumin; OR: odds ratio; Scr: serum creatinine; PNS: primary nephrotic syndrome; TC: total cholesterol; TG triglyceride; UA: uric acid.
Discussion
PNS is a common clinical disease, accounting for >75% of NS cases. 24 Anemia is one of the many complications that occur in patients with PNS, particularly children with PNS. 5 The results of this study showed that 34 of the 150 adult patients developed anemia at the diagnosis of early PNS (eGFR ≥ 60 mL/min/1.73 m2), with a baseline anemia prevalence of 22.67%. The prevalence of anemia in PNS patients with normal renal function (eGFR ≥90 mL/min/1.73 m2) was 17.32%, indicating that some patients had PNS accompanied with anemia when their renal function was normal. Such patients should be recognized in clinical practice and should be actively diagnosed and treated.
In our study, baseline anemia in patients with PNS was mainly characterized by mild and normocytic anemia, with 91.18% of them showing mild anemia and 73.53% normocytic anemia. The reason may be related to the decreased production and urine loss of erythropoietin (EPO) in patients with PNS.1,15,25 EPO is mainly produced by renal interstitial fibroblasts, and its main function is to stimulate the proliferation and differentiation of erythroid progenitor cells in the bone marrow, which will ultimately transform these precursor cells into mature erythrocytes. 17 EPO also induces other effects, including inhibition of ferroportin activity, enhancement of iron uptake, and synthesis of transferrin receptor, 26 which will promote the transcription and translation of Hb genes as well as the release of reticulocytes into the circulation. 1 The damage of kidney tissue in PNS patients results in deficient EPO, which leads to shortened RBC lifespan, and folate deficiency. Meanwhile, due to the accumulation of many toxic substances in the bloodstream, the proliferation and differentiation of erythroids in the bone marrow are impaired. 27 The plasma colloid osmolality is lowered by hypoproteinemia in NS patients, coupled with a compensatory increase in the nonselective synthesis of several proteins in the liver, especially fibrinogen. The hypercoagulable state promotes the aggregation of RBCs and decreases the deformability of RBCs, resulting in the occurrence of anemia in patients with PNS. 27 In addition, it may be associated with a concomitant loss of urinary transcobalamin, vitamin B12 (VB12), folic acid, iron, and transferrin. 17 Transcobalamin is a plasma protein that is essential for the transport and cellular uptake of VB12. Iron and transferrin deficiencies cause microcytic anemia, whereas transcobalamin, VB12, and folate deficiencies cause macrocytic anemia. As patients with PNS may have deficiencies of all these substances, the anemia may be normocytic.
The male-to-female ratio in this study was 1.42:1. Although the difference in the male-to-female ratio between the two groups was not statistically significant, the baseline anemia rate was higher in females (29.03%) than in males (18.18%). The reason for the sex difference in anemia remains unclear, which may be due to the fact that female patients have a higher volume of blood loss during their menstrual period. This may also be related to the poor dietary habits during excessive dieting, which may lead to nutritional deficiency anemia. It may also be related to the lower level of androgens in women. In the present study, Hb levels were positively correlated with diastolic blood pressure in patients with PNS, which may be related to the increased activity of nitric oxide and hypoxia-induced vasodilation. 28
The study revealed that habitual alcohol consumption was also associated with a reduced risk of anemia in patients with PNS, with a corresponding OR of 0.119, which is consistent with the results of a large-scale cross-sectional study in China. 29 In a study analyzing the association between habitual alcohol consumption and erythrocyte-related markers in Japanese men, 30 the participants were categorized into nondrinkers, occasional drinkers, and regular drinkers based on the frequency of alcohol consumption. The results showed that Hb levels tended to increase with increasing frequency and volume of alcohol consumption and that alcohol intake was negatively correlated with low Hb levels. These findings suggested that alcohol can promote Hb synthesis, but the underlying mechanism remains unclear. Meanwhile, habitual alcohol consumption may be detrimental to the individual’s health, depending on the amount of alcohol consumed. Excessive alcohol consumption may increase the risk of various health problems, including cancer and alcoholism. 31 In addition, it has been reported 29 that Hb levels in the cytoplasm of RBCs are reduced in the presence of toxic concentrations (0.5%) of ethanol. Given the potential risks of alcohol consumption to human health, patients with PNS should not be advised to reduce the risk of anemia by drinking alcohol.
In this study, we found that Hb level is closely related to ALB and PALB, which are important indicators of the nutritional status of the body. Our results indicated that Hb level was positively correlated with both ALB and PALB levels. Multivariable logistic regression analysis showed that low levels of ALB and PALB were independent risk factors for baseline anemia in patients with PNS. PALB is mainly synthesized and secreted by the liver, and the total amount of PALB in the serum is low, with a shorter half-life and higher renewal rate. PALB is more sensitive to changes in the body’s nutritional status and is significantly superior to common nutritional monitoring indicators such as ALB. 32 Malnutrition causes a negative nitrogen balance in the body and decreases the PALB level. 32 It is hypothesized that the production and metabolism pathways of Hb, ALB, and PALB may partially share commonalities, which may be related to liver function. PNS patients with long-term malnutrition inevitably had lower levels of ALB, PALB, and protein, resulting in a decrease in the hematopoietic raw materials. At the same time, hypoproteinemia can cause gastrointestinal mucosal edema, reducing digestion and absorption functions, which may further aggravate anemia. In addition, hypoproteinemia induces oxidative stress, which contributes to enhanced phosphatidylserine exposure on the outer leaflet of the RBC membrane. 33 Macrophages and specialized dendritic cells rapidly recognize these RBCs, leading to phagocytosis and catabolism of RBCs in the spleen and liver. 34 This results in a shortened RBC lifespan, which further exacerbates anemia. 15 Meanwhile, the TC and TG levels in the baseline anemia group were significantly lower than those in the other group in our study. Low TC was an independent risk factor for baseline anemia in PNS patients. This suggests that some patients may have excessive control over protein and lipid intake. Serum TC can also be used as an indicator of the nutritional status of the body, and lower cholesterol can cause a decrease in the deformability of RBCs, making them susceptible to destruction. 35 Several studies have shown that there is also a positive correlation between TC and Hb.36–38 The correlation between Hb and cholesterol in the present study was not statistically significant. It might be because the sample size was not large enough. The mechanism underlying the lower serum cholesterol levels in patients with anemia remains unclear. It is believed to be related to the compensatory proliferation of RBCs, which increases cholesterol requirements, relatively low cholesterol levels due to blood thinning, and decreased endogenous cholesterol synthesis in the liver.37–39 Xiong et al. 40 showed that malnutrition was associated with an increased risk of mortality in patients on maintenance hemodialysis. Therefore, regular nutritional assessment and active improvement of nutritional status are important approaches to reduce the incidence of anemia in PNS patients.
In this study, 24-h proteinuria was higher in the baseline anemia group than in the baseline no anemia group. Multivariable logistic regression analysis showed that 24-h proteinuria was not an independent risk factor for baseline anemia in patients with PNS, which is consistent with the results of a study in adult MN patients. 41 Unlike the results of a study on anemia in children with NS, the cause of anemia in children with NS is closely related to the urinary loss of metal ions such as iron, copper, and zinc as well as transferrin, EPO, and VB12 due to massive proteinuria. 17 The reason for this finding may be related to the small sample size, and a large cross-sectional study is needed to further clarify the relationship between proteinuria and anemia in adult PNS patients.
Conventional anemia treatments involve supplements of hematopoietic raw materials such as iron or folic acid, erythropoiesis-stimulating agents (ESAs), and RBC transfusion.42–43 However, these treatments have their own limitations. Iron supplementation may increase the risk of infection and cardiovascular-related side effects. RBC transfusion could cause an anaphylactic reaction, infection, and graft versus host disease. It has been reported that ESAs may increase the risk of hypertension, thrombotic complications, and adverse cardiovascular events due to the nonphysiological increase in erythropoietin levels. Meanwhile, high doses of ESAs may induce glomerular endothelial dysfunction.41–43 Hypoxia-inducible factor (HIF) prolyl hydroxylase inhibitor (PHI) is a novel drug for renal anemia. Roxadustat is the most commonly used HIF-PHI, which could increase erythropoietin levels physiologically. The main mechanisms include activating HIF transcription factors, increasing endogenous EPO production, and decreasing hepcidin and ferritin levels. Previous clinical studies have verified the efficacy of HIF-PHIs in the treatment of renal anemia while avoiding the risks caused by high-dose iron and ESA treatments.42–44 The HIF-prolyl hydroxylase domain pathway can regulate the expression of genes related to psoriasis, cancer, rheumatoid arthritis, hematopoiesis, and glucose metabolism. 44 Hence, HIF-PHIs may increase the risk of cancer development, as confirmed by some animal experiments.45–46 However, recent large-scale clinical studies on roxadustat have not shown any cancer risk. There are inadequate real-world data supporting side effects such as vascular endothelial growth factor-mediated retinal hemorrhage, thrombosis events, and cancer activation.47–48
There are some limitations of this study. First, this study is a single-center cross-sectional study, and the sample size is small. Hence, it is necessary to expand the sample size and conduct further prospective studies to confirm the results. Second, as all patients included in this study were required to undergo renal biopsy to confirm the diagnosis of PNS, some patients did not undergo renal biopsy for various reasons. Thus, there may be a selection bias. Finally, the reasons for anemia in patients with PNS have not been explored in depth. Anemia in PNS may occur due to excessive urinary loss of iron, transferrin, EPO, transcobalamin, and metals. 17 Because most of the patients in this study were mildly anemic, they did not undergo serum iron metabolism, folate, and VB12 tests. The data related to the abovementioned possible causes of anemia were missing.
In future prospective studies, serum and urine EPO, iron metabolism, folic acid, VB12, and other indicators related to anemia in NS should be included in the scope of analysis. The relationship between anemia and the prognosis of patients with PNS should be further evaluated. This will provide a reliable basis for improving the quality of life and prognosis of PNS patients.
Conclusion
PNS patients have a high prevalence of comorbid anemia, mainly mild anemia and normocytic anemia. Some PNS patients develop anemia when their renal function is not yet significantly reduced. Reduced ALB, PALB, and TC as well as the absence of habitual alcohol consumption were independent risk factors for baseline anemia in patients with PNS.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251359458 - Supplemental material for Clinical analysis of primary nephrotic syndrome complicating anemia
Supplemental material, sj-pdf-1-imr-10.1177_03000605251359458 for Clinical analysis of primary nephrotic syndrome complicating anemia by Xing Chen, Xiaoyu Liu, Zhen Feng, Zhijuan Hu, Kai Niu and Bing Liu in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605251359458 - Supplemental material for Clinical analysis of primary nephrotic syndrome complicating anemia
Supplemental material, sj-pdf-2-imr-10.1177_03000605251359458 for Clinical analysis of primary nephrotic syndrome complicating anemia by Xing Chen, Xiaoyu Liu, Zhen Feng, Zhijuan Hu, Kai Niu and Bing Liu in Journal of International Medical Research
Footnotes
Acknowledgements
The authors are thankful to the patients for their participation.
Author contributions
C.X. analyzed, revised, and drafted the manuscript. L.X. collected and analyzed the data. F.Z., H.Z., N.K., and L.B. collected the data. C.X. had full access to the study data and assumed responsibility for the integrity and accuracy of the data. All authors approved the final manuscript.
Data availability statement
All data generated or analyzed during this study are included within the article. Further enquiries can be directed to the corresponding author.
Disclosure
There are no conflicts of interest reported by the authors.
Statement of ethics
The study was approved by the Ethics Committee of Hebei General Hospital.
Funding
The study received no funding.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.