
Abstract
Cilioretinal artery occlusion is a serious condition that results in a sudden and severe decline in vision. There are various treatment methods for retinal artery occlusion, but their effect remains unclear. Cilioretinal artery occlusion post-intravitreal drug injection is rare, with no relevant reports published to date. A man in his early 50s was admitted to our department due to a nail injury to the right eye. The patient underwent exploratory and suture surgery for eyeball penetrating injury, intraocular foreign body removal, and intravitreal vancomycin injection. The patient’s preoperative visual acuity in the right eye was 0.1, which decreased to FC/5 cm one day after surgery. Wide-angle fundus photography revealed cilioretinal artery occlusion. We highly suspected that the sudden increase in intraocular pressure after intravitreal injection of vancomycin was the cause of cilioretinal artery occlusion in this case. Mouse nerve growth factor (30 μg) and anisodine hydrobromide tablets (3 mg) were used for neurotrophic and microcirculation-improving treatments. Follow-up fundus fluorescein angiography at 31 seconds on postoperative day 18 showed filling of the cilioretinal artery. At 14 months post-surgery, the patient’s right eye visual acuity recovered to 0.1. In conclusion, cilioretinal artery occlusion post-intravitreal vancomycin injection is an extremely rare but severe complication that significantly affects vision. Early diagnosis and timely treatment are vital in such cases.
Keywords
Introduction
Cilioretinal artery occlusion (CLRAO) is an acute, vision-threatening eye disease caused by embolism, arterial wall changes, or thrombosis, leading to partial or complete blockage of the cilioretinal artery and acute ischemia of the supplied retina. Anatomically, as the cilioretinal artery is not an end-artery, its occlusion is relatively rare, accounting for approximately 5.0% of all retinal artery occlusions. 1 CLRAO post-intravitreal drug injection is even rarer, with no relevant reports published to date. Diagnosis of this complication is based on acute retinal whitening in the cilioretinal artery distribution area observed through ophthalmoscopy, color fundus photography, and delayed perfusion of the cilioretinal artery on fundus fluorescein angiography (FFA). 2
Currently, there are various treatment methods for retinal artery occlusion, but their effect remains unclear. In terms of visual outcome, the efficacy of several conventional treatments, including paracentesis of the anterior chamber, acetazolamide, eyeball massage, heparin, and aspirin, has not been clearly proven. 3 Ophthalmologic signs and symptoms may be a warning sign of cardiovascular or cerebrovascular events such as stroke. 4 Patients should undergo urgent screening and treatment when vascular risk factors are present.
This is the first report to describe the case of a man in his early 50s who developed CLRAO following an intravitreal injection of vancomycin during surgery for an ocular injury. The patient exhibited a decrease in visual acuity in the right eye to FC/5 cm and was treated with neurotrophic and vasodilator medications. At 14 months post-surgery, the patient’s right eye visual acuity recovered to 0.1. The purpose of this case report is to discuss the mechanism and management of CLRAO following intravitreal drug injection, highlighting the need for clinical awareness.
Case presentation
Presentation
A man in his early 50s was admitted to the Department of Ophthalmology, Provincial Hospital Affiliated to Shandong First Medical University, China, due to a nail injury to the right eye on 15 November 2023. The patient had a 10-year history of hypertension and hyperlipidemia, with a blood pressure level of approximately 130/90 mmHg, peaking at 170/100 mmHg. He was not treated with medication. He had no history of smoking or chronic diseases such as diabetes or coronary heart disease as well as no family history of such conditions. The results of the ophthalmologic examination were as follows: visual acuity: right eye 0.1, left eye 0.8; intraocular pressure (IOP): cooperation insufficient; the right eyelid showed no significant swelling, conjunctival and ciliary congestion, and transparent cornea. A nail was embedded in the sclera 5 mm posterior to the nasal corneal limbus, with purulent discharge around the wound. Detailed fundus examination was not possible. No significant abnormalities were observed in either the anterior or posterior segments of the left eye. Orbital computed tomography revealed abnormal density focus in the right eye, suggesting the presence of a foreign body. Blood routine revealed a white blood cell count of 10.56 × 109/L (normal range: 3.5–9.5 × 109/L). The absolute monocyte count was 0.61 × 109/L (normal range: 0.1–0.6 × 109/L), and the absolute neutrophil count was 7.15 × 109/L (normal range: 1.8–6.3 × 109/L). Coagulation parameters were within the normal range.
Surgery
After thorough preoperative preparation, including establishing intravenous access and fluid supplementation to maintain water and electrolyte balance, the patient underwent an emergency operation under general anesthesia, which included exploratory and suture surgery for the eyeball penetrating injury, intraocular foreign body removal, and intravitreal vancomycin injection. The conjunctiva was incised 5 mm posterior to the nasal limbus, separating the underlying fascia, revealing the nail embedded in the scleral region near the muscle insertion of the medial rectus. The foreign body was removed, prolapsed vitreous was trimmed, and the sclera and conjunctiva were sutured. The temporal sclera remained intact. Vancomycin (0.1 mg, volume = 0.1 mL) was injected into the vitreous cavity using a 30G needle, 4 mm posterior to the inferior temporal corneal limbus, followed by pressing of the injection site with a moist cotton swab. Another 25 mg of vancomycin was injected subconjunctivally. At the end of the surgery, the IOP returned to normal. The conjunctival sac was coated with tobramycin–dexamethasone eye drops and compression bandaging.
Postoperative conditions
Postoperative management was implemented due to purulent wound secretions and included intravenous cefazolin (2 g daily for 1 week) for infection control and intravenous dexamethasone (5 mg daily for 3 days) for inflammation management. Topical ophthalmic treatments comprised tropicamide eye drops (twice daily for 9 days) for mydriasis, atropine ointment (once nightly for 9 days) for mydriasis, levofloxacin eye drops (four times daily for 2 weeks) as antimicrobial prophylaxis, and tobramycin–dexamethasone eye drops (seven times daily for 2 weeks) as combined anti-inflammatory and antimicrobial therapy.
On 16 November 2023 (first postoperative day (POD1)), the patient reported a dark shadow in the visual field, and the visual acuity in the right eye decreased to FC/5 cm. He had a IOP level of 18 mmHg, with mild corneal edema. Fundus examination was unclear. The patient’s cornea regained its transparency on POD3, and B-scan ocular ultrasound showed no significant retinal detachment (Figure 1(a)). Fundus photography showed a flat retina with scattered hemorrhages and grayish-white edema in the posterior pole, resembling a cherry-red spot, suggesting CLRAO in the right eye (Figure 1(b)). We considered that the cause of the CLRAO was the sudden and significant increase in IOP following a rapid intravitreal injection of 0.1 mL of vancomycin, which led to irreversible arterial hypoperfusion. Additionally, the patient had vascular risk factors, such as hypertension and hyperlipidemia, which made the cilioretinal artery more susceptible to occlusion. Optical coherence tomography (OCT) on POD5 showed retinal edema and thickening from the macula to the optic disc (Figure 1(c)). Neurotrophic and microcirculation-improving treatments were added, including mouse nerve growth factor (30 μg) and anisodine hydrobromide tablets (3 mg). On POD7, the visual acuity in the patient’s right eye recovered to FC/10 cm, with a IOP of 13 mmHg. Fundus examination with a slit lamp revealed a flat retina with few hemorrhages and grayish-white edema in the posterior pole, along with extremely thin temporal side arteries indicating CLRAO. No signs of infection were observed, ruling out endophthalmitis. Continued neurotrophic and microcirculation-improving treatments were administered.

Ophthalmic examination after the patient’s cornea regained transparency post-surgery. (a) B-ultrasound of the right eye showed no significant retinal detachment. (b) Fundus photography indicated grayish-white edema in the posterior pole with a cherry-red spot appearance, suggesting CLRAO and (c) OCT showed retinal edema and thickening from the macula to the optic disc. CLRAO: cilioretinal artery occlusion; OCT: optical coherence tomography.
On 27 November 2023 (POD12), the patient’s visual acuity was FC/10 cm, with a IOP of 16 mmHg, and he was discharged from the hospital. The temporal side arteries remained extremely thin, indicating continued presence of CLRAO.
Postoperative follow-up conditions
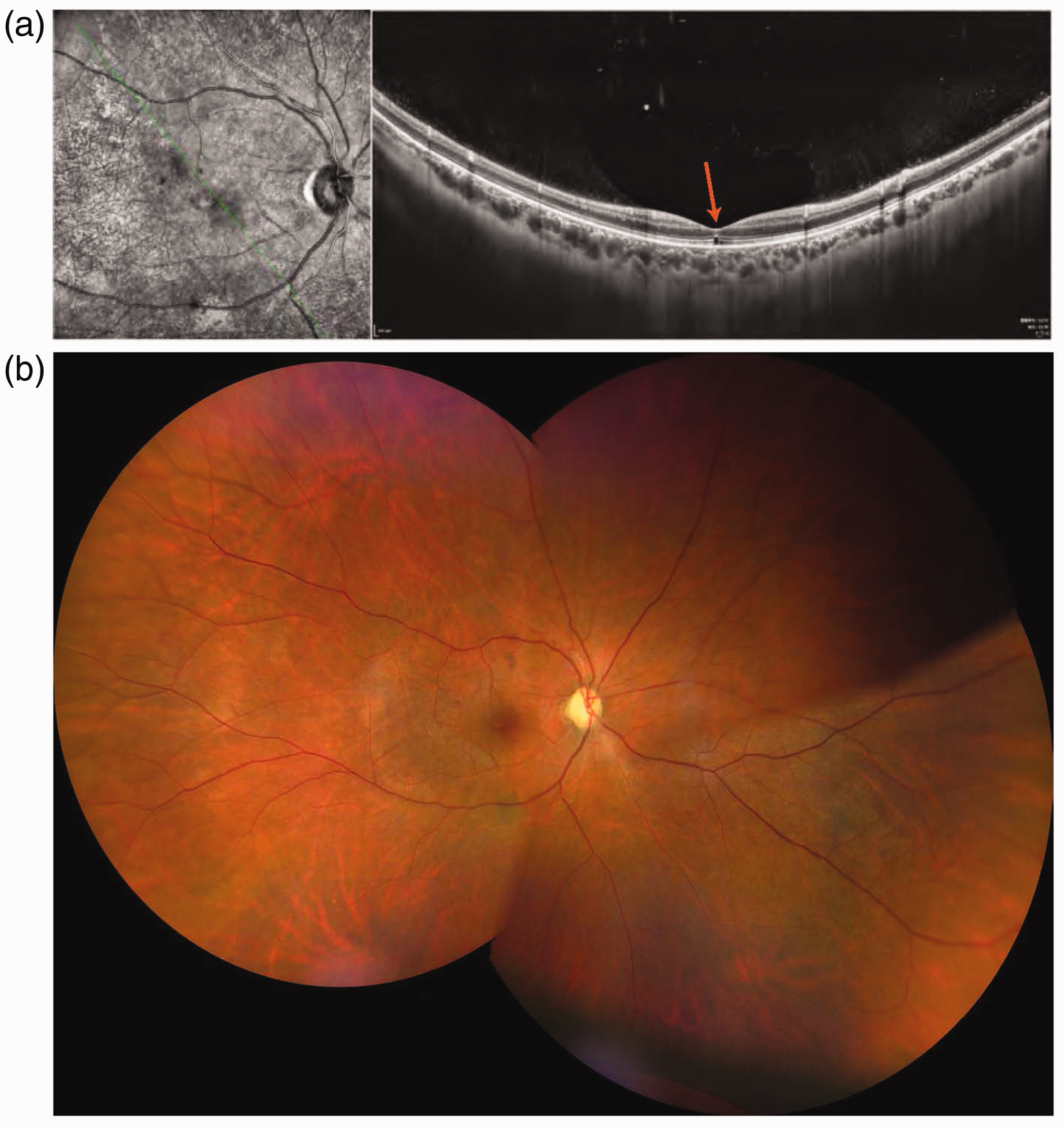
After discharge, the patient continued neurotrophic and microcirculation-improving treatments, with monthly follow-ups including vision tests, OCT, fundus photography, and B-ultrasound of the eyes. On 3 December 2023 (POD18), the visual acuity in the patient’s right eye was FC/15 cm. OCT showed reduced retinal edema and central foveal thickness thinning (Figure 2(a)). FFA at 31 seconds showed filling of the cilioretinal artery (Figure 2(b)). Fundus photography showed the disappearance of the cherry-red spot (Figure 2(c)).

The 7-day follow-up conditions. (a) OCT showed reduced retinal edema and decreased central foveal thickness. (b) FFA at 31 seconds showed filling of the cilioretinal artery and (c) Fundus photography showed the disappearance of the cherry-red spot. OCT: optical coherence tomography; FFA: fundus fluorescein angiography.
On postoperative month 12, a follow-up examination revealed that the visual acuity in the patient’s right eye was 0.1. OCT showed disruption of the ellipsoid zone under the central fovea (Figure 3(a)). Fundus photography revealed that the retinal vascular structure had returned to normal (Figure 3(b)). On postoperative month 14, a follow-up examination showed the visual acuity in the patient’s right eye was 0.1.
The 12-month follow-up conditions. (a) OCT showed disruption of the ellipsoid zone under the central fovea and (b) Fundus photography revealed that the retinal vascular structure had returned to normal. OCT: optical coherence tomography.
This study was approved for publication by the review board of the Provincial Hospital of Shandong First Medical University (Shandong Provincial Hospital). All patient details have been de-identified. After fully informing the patient and their family members about treatment and prognosis, we obtained patient consent to treatment. The reporting of this study conforms to the Case Report (CARE) guidelines. 5
Discussion
Retinal artery occlusion is an acute, vision-threatening eye condition. These occlusions can be categorized based on the affected blood vessels as follows: CLRAO, central retinal artery occlusion, branch retinal artery occlusion, and precapillary arteriole occlusion. The cilioretinal artery, originating from the short posterior ciliary arteries, supplies blood to the macular region. It may run above or below the macula, supplying a small part of the inner retina near the macula, with significant variations in number, size, and distribution. When an occlusion occurs, it is termed as CLRAO. CLRAO involving macular blood supply typically leads to sudden catastrophic vision loss and subsequent retinal neuronal damage.
Retinal artery occlusion results from acute interruption of blood flow in the eye due to various underlying conditions. Most patients with retinal artery occlusion have vascular risk factors, including hypertension, hypertensive crisis, diabetes, dyslipidemia, acute coronary syndrome, and smoking. 6 Smoking is a well-known risk factor for vascular dysfunction and thrombotic events, exerting adverse effects on cardiovascular health by causing endothelial dysfunction, inflammation, and oxidative stress. 7 However, the patient had no smoking history. Additionally, embolism from the internal carotid artery, aortic arch, or heart is a major cause of retinal artery occlusion. 8 Systemic evaluations should focus on the risk of fatal strokes and cardiovascular events due to emboli causing retinal artery occlusion. 9 Infection and dehydration are risk factors for thrombosis and atherosclerosis. 10
Iatrogenic ophthalmic artery occlusion is a rare cause of sudden vision loss. It is a general term that includes occlusions of all types of ophthalmic artery or its branches (central retinal artery, ciliary arteries, cilioretinal artery, branch retinal artery, and arterioles occlusions) caused by iatrogenic reasons. Owing to the direct association between retinal vessels and IOP, IOP is considered one of the most important factors affecting retinal blood flow and velocity. 11 Changes in IOP may lead to hemodynamic changes in the retinal artery, which could predispose the patient to retinal artery occlusion events. 12 A sudden extreme increase in IOP can reduce retinal blood flow; if the IOP is high enough, it can block the blood circulation in the outer layers of the retina, leading to ophthalmic artery occlusion. Animal studies have shown reduced retinal function and blood flow when IOP exceeds 60 mmHg. 13
Iatrogenic increases in IOP can result from facial filler injections, intravascular procedures, intravitreal gas or drug injections, retrobulbar anesthesia, intra-arterial chemotherapy, and vitrectomy.13,14 A study by Hoguet et al. demonstrated that immediately or within 1 min after intravitreal injection, 100% of the study patients experienced an increase in IOP, with a reported mean post-injection IOP range of 28.3–55.2 mmHg. 15 A study by Meyer et al. showed that after an intravitreal injection of 0.05 mL, IOP immediately rose to 50 mmHg. 16 A study by Bracha et al. suggested that when the needle specifications are controlled, injecting a larger volume intravitreally may lead to greater acute IOP fluctuations. 17 Although a transient increase in IOP after intravitreal drug injection is common and reversible, routine procedures may cause IOP elevation and subsequent iatrogenic ophthalmic artery occlusion in patients with risk factors (old age, hypertension, diabetes, stroke history, and atherosclerosis). 13
In this case, the patient underwent exploratory and suture surgery for the eyeball penetrating injury, intraocular foreign body removal, and intravitreal vancomycin injection (0.1 mg, volume = 0.1 mL) under general anesthesia. Based on the disease course, we speculate that the patient’s CLRAO is related to the following factors: a 10-year history of hypertension and hyperlipidemia without medication increased the risk of retinal artery occlusion, and the sudden increase in IOP after intravitreal vancomycin injection reduced cilioretinal artery blood flow, eventually causing the occlusion. A study by Kudsieh et al. suggested that elevated IOP can increase capillary pressure, leading to vascular occlusion, and a sudden significant rise in IOP may cause irreversible arterial perfusion insufficiency. 18 Although the patient was admitted due to ocular trauma, which could have led to CLRAO, the patient’s right eye visual acuity was 0.1 before surgery and decreased to FC/5 cm on POD1, thus excluding trauma as the cause of the CLRAO. Nagpal et al. reported a case of a 34-year-old male with a penetrating ocular injury combined with an intraocular metallic foreign body embedded in the superficial layer of the temporal inferior retina, leading to occlusion of the temporal inferior branch of the retinal artery. 19 However, in our case, the retina was not damaged by the intraocular foreign body, and the IOP was maintained at a low level throughout the surgery to remove the foreign body. Therefore, we did not consider surgery to remove the foreign body as the cause of the patient’s CLRAO. Post-surgery, there were no significant abnormalities in the anterior segment of the eye, and fundus photography showed no retinal tears and no significant retinal detachment. The corrected visual acuity did not significantly improve. We considered that the large volume and rapid injection of vancomycin into the vitreous cavity caused a transient and sharp increase in IOP, which led to CLRAO in this patient.
In theory, the sooner the retina is reperfused after acute retinal artery occlusion, the better the chance of visual function improvement. Timely intervention is crucial for improving vision and prognosis, but most cases of acute retinal artery occlusion lack standardized treatment methods. The previously explored options include ocular massage, hemodilution, anterior chamber paracentesis, antiplatelet drugs, transluminal neodymium-doped yttrium aluminum garnet (Nd:YAG) laser embolectomy/embolysis, hyperbaric oxygen therapy, local intra-arterial fibrinolysis, andsystemic intravenous fibrinolytic therapy, but most of these have not shown significant benefits compared with non-intervention. 4 The current literature suggests that treatment with intravenous tissue plasminogen activator may be effective. Patients should undergo urgent screening and treatment in the presence of vascular risk factors. 20 It has been reported that intravenous tenecteplase may be a safe and reasonable treatment for central retinal artery occlusion and branch retinal artery occlusion. 21 Anisodine, a tropane alkaloid extracted from the root of Anisodus tanguticus, exhibits significant vasoactive properties and microcirculation-improving effects. To improve its chemical instability, researchers have developed a hydrobromide form of anisodine. 22 Anisodine hydrobromide promotes both neural cell regeneration, namely, dendritic and axonal structural reorganization and synaptic vesicle protein remodeling, and enhances neurological function through the modulation of neurotrophic factors and neuroplasticity mechanisms. 23 Nerve growth factor is a well-characterized neurotrophic factor that plays a critical role in the survival, growth, and differentiation of neurons both in the central and peripheral nervous system. 24 Studies have demonstrated that nerve growth factor ameliorates retinal ganglion cell conduction, which correlates with the recovery of retinal nerve fiber plus ganglion cell layer structure. 25 In this case, the patient was administered with mouse nerve growth factor and anisodine hydrobromide as neurotrophic and microcirculation-improving treatments while avoiding strenuous exercise. At 12 months post-surgery, the right eye’s visual acuity improved to 0.1, but OCT showed ellipsoid zone disruption, possibly related to macular edema post-ischemia.
This case report had a limitation. Although we ultimately identified the cause of the patient’s postoperative vision loss, his visual outcome might have been better if CLRAO had been considered and treated earlier.
Conclusion
CLRAO post-intravitreal vancomycin injection is an extremely rare but severe complication that significantly affects vision. Early diagnosis and timely treatment are vital in such cases.
Footnotes
Acknowledgements
The patient cooperated with our work during the process of diagnosis and treatment and followed the diagnosis and treatment plans prepared by our surgery team. We are deeply grateful to the patient and their family members for their cooperation.
Author contributions
CZ provided patient information and wrote the manuscript. CZ and MH collected the data. HZ and WZ obtained resources and reviewed and edited the manuscript. All authors contributed to the article and approved the submitted version.
Consent to participate
After fully informing the patient and their family members about treatment and prognosis, we obtained patient consent to treatment.
Consent for publication
We have de-identified the patient details, and the identity of the patient cannot be ascertained in any way.
Data availability statement
The datasets generated for this study can be found within the article.
Declaration of conflicting interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical considerations
This study was approved for publication by the review board of the Provincial Hospital of Shandong First Medical University (Shandong Provincial Hospital) (SZRJJ:NO.2023-037).
Funding
This research was funded by the National Natural Science Foundation, China (grant number 81873677).