
Abstract
Objective
This study aimed to investigate the prevalence of frailty and its influencing factors among older individuals diagnosed with proliferative diabetic retinopathy, a predominant complication of diabetes that frequently leads to visual impairment. Additionally, this study aimed to identify key demographic, socioeconomic, and clinical determinants linked to frailty within this specific patient population.
Methods
This multicenter cross-sectional study enrolled 600 patients with proliferative diabetic retinopathy (aged ≥60 years) from two tertiary hospitals in Baoding (February to August 2024). The patients were categorized into frailty (n = 345) and nonfrailty (n = 255) groups using standardized criteria. The data collected included demographic characteristics, medical history, frailty assessment (frailty phenotype), and social support rating scale scores.
Results
The frailty prevalence among the participants was 57.46%. Significant between-group differences (P < 0.05) were observed in diabetes duration, social support, monthly income, bilateral eye involvement, living alone, and having ≥3 comorbidities. Frailty scale scores were inversely correlated with social support (r = −0.42, P < 0.001). Multivariate analysis identified the following independent predictors: low income (odds ratio = 2.34; 95% confidence interval: 1.67–3.28), solitary living (odds ratio = 1.89; 95% confidence interval: 1.32–2.71), multiple complications (odds ratio = 3.12; 95% confidence interval: 2.18–4.46), prolonged diabetes (odds ratio = 1.45/year; 95% confidence interval: 1.32–1.59), and poor social support (odds ratio = 0.92/point; 95% confidence interval: 0.89–0.95).
Conclusions
Over half of the older patients with proliferative diabetic retinopathy exhibit frailty, which is significantly associated with socioeconomic disadvantages, clinical severity, and inadequate social support. These findings highlight the need for comprehensive geriatric assessment in proliferative diabetic retinopathy management.
Introduction
The incidence of type 2 diabetes mellitus (T2DM) is on the rise, with approximately 537 million adults worldwide suffering from this condition in 2021; this number is expected to reach 783 million by 2045. 1 This increase is particularly evident in the aging population, with a projected prevalence rate of 25% among individuals aged 75–79 years by 2045. 2 Prolonged exposure to high glucose levels can lead to damage in various tissues and organs, characterized by increased permeability of small blood vessels, vascular occlusion, compensatory neovascularization, and the potential of fragile neovascular vessels to rupture and bleed, worsening the progression of the disease. 3 One of the most common complications of diabetes is diabetic retinopathy (DR), which is prevalent among diabetic patients in China, currently home to the highest number of individuals with diabetes globally.4–6 DR is a prevalent microvascular complication in patients with diabetes, and its early identification and prompt treatment can prevent vision loss. DR initially presents as asymptomatic retinal abnormalities such as micro-aneurysms and then advances to proliferative DR (PDR), a more severe stage marked by neovascularization and bleeding in the retina or vitreous humor. 7 This issue has escalated into a significant public health concern. DR is categorized into two main types: nonproliferative DR (NPDR) and PDR, with the latter often necessitating surgical intervention in advanced cases. 8 Further investigation is warranted to determine whether postoperative visual outcomes can be successfully enhanced.
With the aging of the global population, frailty has emerged as a significant public health concern. Studies have shown that approximately 12% of adults aged ≥50 years who live independently in communities are considered frail. 9 Frailty is associated with various risk factors, including age and sex, and is linked to an increased likelihood of negative outcomes such as falls, fractures, hospitalizations, and mortality among older adults. 10 Given the accelerated aging of the Chinese population, the effective management of frailty is currently more crucial than ever. Frailty often results from a combination of aging processes and chronic conditions such as diabetes, hypertension, and chronic obstructive pulmonary disease. 11 A substantial proportion of older Chinese adults, approximately one in five, are affected by diabetes, which shares similar pathological mechanisms and risk factors with frailty, such as insulin resistance, glucose dysregulation, and obesity. 12 Research has indicated that the prevalence of frailty among community-dwelling older adults with diabetes (20.1%) is notably higher than that of the general older population (10%), and those with diabetes tend to experience a more rapid increase in frailty with aging, leading to worsened health outcomes and reduced quality of life. 13 Early detection of frailty is essential for initiating targeted interventions to slow or reverse its progression, thereby alleviating the burden on the healthcare system. 14 Therefore, it is important to identify older patients with PDR at high risk of deterioration early on and implement effective intervention measures. This can help improve the quality of life and prognosis of older patients with PDR.
Methods
Study participants
Convenience sampling was used to select 600 older patients with PDR and T2DM treated at two tertiary hospitals in Baoding from February 2024 to August 2024. The inclusion criteria were as follows: (a) aged ≥60 years; (b) meet the diagnostic criteria for PDR as outlined in the “China Clinical Diagnosis and Treatment Guidelines for Diabetic Retinopathy (2014)”; (c) have normal cognitive function, can communicate effectively, and can complete the questionnaire independently or with the assistance of relevant personnel; and (d) can provide informed consent. The exclusion criteria were as follows: (a) retinopathy caused by other diseases; (b) severe physical disabilities that hinder mobility; (c) communication difficulties due to cognitive impairment or mental illness that prevent completion of the questionnaire; and (d) incomplete survey data. Each predictive factor included in the final binary logistic regression analysis should have at least five cases of positive PDR patients. Previous studies have revealed that there are approximately 4–7 independent risk factors for frailty in older patients with chronic diseases. 15 Therefore, it was estimated that the predictive model in this study would include no more than 10 predictive factors, requiring a minimum of 100 PDR patients with frailty to be included. Given that the frailty rate of patients with DR is approximately 35.8%, the minimum sample size should be 150 cases, with 600 cases being finally included (Figure 1). This cross-sectional study has been approved by the Ethics Committee of Baoding No.1 Central Hospital (Ethics number: 2024015). The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 16 This research was conducted in full compliance with the ethical principles outlined in the Helsinki Declaration of 1975, including its most recent amendments (2024). To ensure confidentiality and privacy, all identifiable information pertaining to the study participants has been rigorously anonymized.
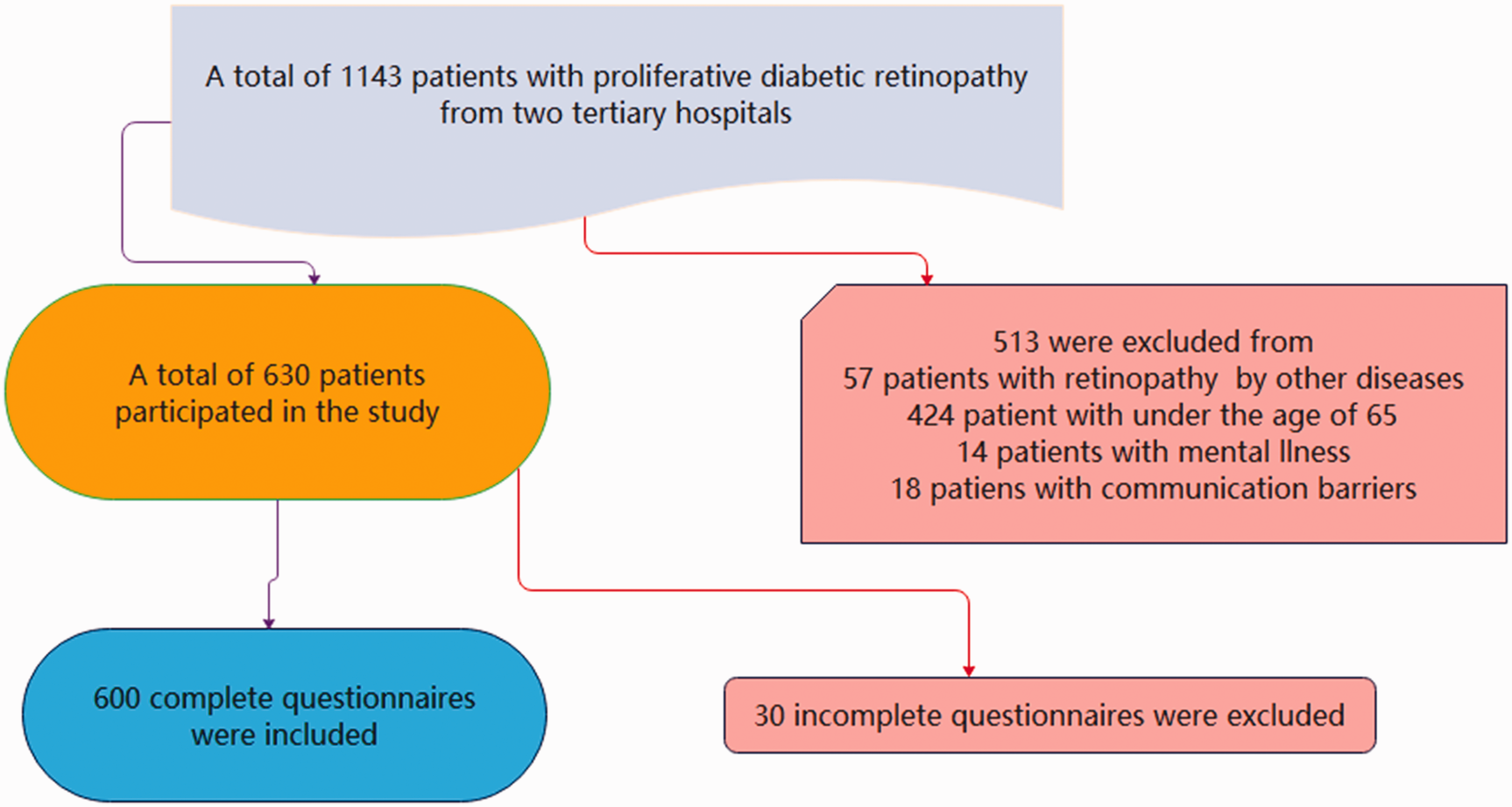
Flowchart of the study.
Study tools
General information questionnaire
Designed by the researcher according to the research objectives and significance, this questionnaire included demographic data such as age, sex, marital status, education level, diabetes duration, payment methods, average monthly household income, social support, number of diseased eyes, living situation, and number of complications.
Frail scale
The Frail Scale has a Cronbach’s alpha coefficient of 0.921, which is used for assessing frailty and consists of the following five items 17 : (a) fatigue: feeling tired most of the time or all the time in the past 4 weeks; (b) resistance: difficulty climbing a flight of stairs without any assistance or help from others; (c) ambulation: difficulty walking 100 m without assistance; (d) illness: having five or more illnesses; (e) loss of weight: a weight loss of over 5% in the past year. Each item is scored as 1 for “yes” and 0 for “no,” with a total score of 5. A score of 0–2 indicates no frailty, while a score of ≥3 is indicative of frailty.
Social support rating scale (SSRS)
The SSRS has a Cronbach’s alpha coefficient of 0.871, consisting of three dimensions (subjective support, objective support, and utilization of support) with a total of 10 items. 18 Scores range from 12 to 66; based on the SSRS scores, individuals are categorized as low (12–35 points), moderate (35–50 points), and high (50–66 points) social support. Higher scores indicate a better level of social support.
Data collection methods
The researchers utilized uniform instructions to clearly explain the purpose and contents of the investigation to the participants. After obtaining informed consent, one-on-one interviews were conducted, recording information truthfully and objectively. Following the completion of the survey, timely checks were conducted to ensure the completeness and accuracy of the data. A total of 630 questionnaires were distributed for this study, with 600 valid responses received, resulting in an effective response rate of 95.2%. Ultimately, a total of 600 samples were included in the study.
Statistical analysis
Initially, we utilized SPSS 25.0 software to conduct statistical analyses. Upon assessing all continuous variables for normal distribution, data displaying normal distribution were reported as mean ± standard deviation (X ± SD), with the comparison of mean differences between two groups conducted through the t-test for independent samples. Data exhibiting non-normal distribution were represented as median (25th percentile, 75th percentile), with differences between groups analyzed using non-parametric tests. The chi-square test was utilized to assess disparities in discontinuous variables among groups. Binary logistic regression was employed to determine the factors influencing frailty in patients with PDR. A P value of <0.05 was considered to indicate statistical significance in the observed differences.
Results
Comparative analysis of the characteristics of patients with PDR between the frailty and nonfrailty groups
The two groups showed significant disparities in diabetes duration, social support, average monthly family income, number of diseased eyes, living situation, and number of complications (P < 0.05; Table 1). However, there were no significant differences in terms of sex, age, marital status, education level, and payment method (P > 0.05; Table 1). Compared with patients in the nonfrailty group, those in the frailty group had longer diabetes duration, lower levels of social support, decreased average monthly family income, higher prevalence of eye disease in both eyes, higher rates of living alone, and higher number of complications.
Comparative analysis of the characteristics of frailty in patients with proliferative diabetic retinopathy.
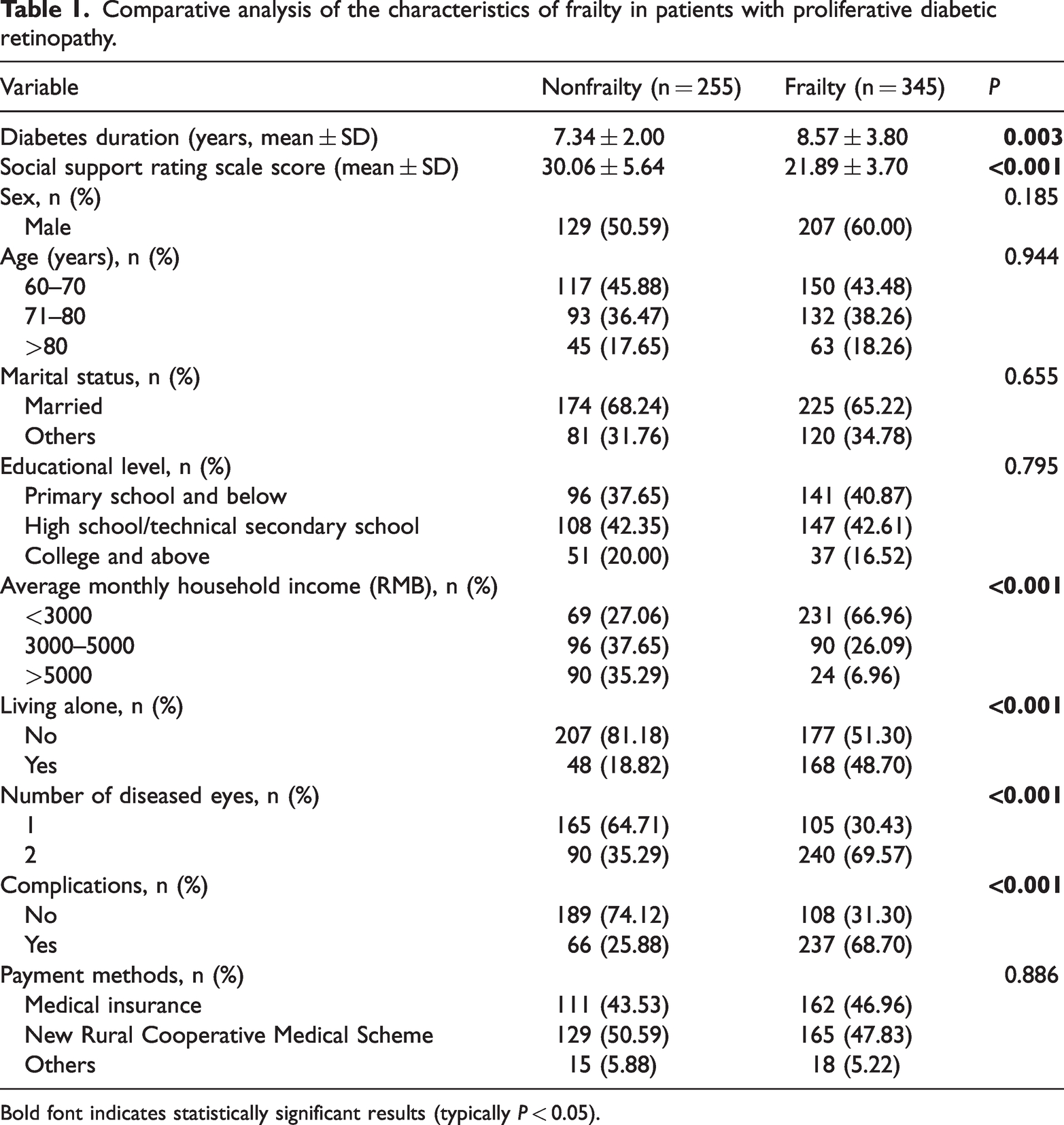
Bold font indicates statistically significant results (typically P < 0.05).
Comparison analysis of frailty scale scores and SSRS scores of patients with PDR between the frailty and nonfrailty groups
The prevalence of frailty among older patients with PDR was 57.46%. The average frailty scale score in the frailty group was 2.93 ± 1.38, while the average SSRS score was 27.00 ± 9.12. In contrast, the nonfrailty group exhibited significantly different scores, with an average frailty scale score of 1.12 ± 0.15 and SSRS score of 55.23 ± 15.34. These differences between the two groups were statistically significant (Figure 2). Thus, patients in the frailty group exhibited higher frailty scale scores and lower SSRS scores.

Comparison of the frailty scale scores and social support rating scale scores between the two groups (**P < 0.01, *P < 0.05).
Correlation analysis between frailty and social support among patients with PDR
The correlation between frailty scores and the total dimension of social support as well as scores in each individual dimension demonstrated a negative relationship (P < 0.05; Table 2). This suggested that as frailty levels increase, social support levels decrease, and vice versa.
Correlation analysis between frailty and social support in patients with proliferative diabetic retinopathy (r value).

Note: all P < 0.05.
Results of a binary multiple factor logistic regression with depression as the dependent variable
The results of binary logistic regression analysis indicated that several factors, including average monthly family income (odds ratio (OR) = 0.18, 95% confidence interval (CI): 0.04–0.77), living alone (OR = 2.90, 95% CI: 2.11–8.52), number of complications (OR = 4.23, 95% CI: 2.71–9.43), number of diseased eyes (OR = 3.22, 95% CI: 2.14–8.10), and level of social support (OR = 0.70, 95% CI: 0.62–0.80), were found to be independent predictors associated with the development of frailty in older patients diagnosed with PDR (P < 0.05; Table 3).
Results of a binary multiple factor logistic regression with depression as the dependent variable.

Bold font indicates statistically significant results (typically P < 0.05).
Discussion
This study showed that the prevalence of frailty in older patients with PDR was 57.46%, which is significantly higher than that in the general older population (26.02%) and older diabetic population (20.10%).19,20 Recent studies have highlighted that frailty is a significant concern among individuals with diabetes, affecting up to 48% of this population. 21 Moreover, research has suggested that diabetic patients are 3–5 times more likely to develop frailty than their nondiabetic counterparts. 21 A comprehensive meta-analysis focusing on frailty in older adults with diabetes further supports these findings, reporting a pooled prevalence of 20.1%. Notably, this analysis revealed considerable heterogeneity across the included studies, reinforcing that frailty is markedly more common in older diabetic patients than in those without diabetes. 22 These findings emphasize the heightened vulnerability of patients with PDR in tertiary care settings. This increased susceptibility is likely due to their advanced progression of retinal disease and a greater burden of comorbid conditions compared with community-based populations. The potential reasons for this could be that older patients with PDR included in this study had multiple chronic complications of diabetes, along with a long diabetic duration, poor daily blood glucose control, and lack of regular follow-up examinations, all of which are closely related. This suggests that older patients with PDR are more prone to experiencing frailty. Furthermore, with aging, the risk of frailty, cognitive impairment, and other geriatric syndromes in patients with PDR also increases. According to the latest data from the China National Bureau of Statistics, the population of older people aged ≥60 years in China has reached 253.8 million as of 2019, accounting for 18.1% of the total population. 23 Frailty is a significant health hazard that threatens the safety of older patients; however, it is often overlooked. Recent studies have indicated that frailty affects approximately one-third of the older population, increasing the risk of adverse events in older individuals. 24 Compared with nonfrail older individuals, frail older people have a 15%–50% higher risk of mortality, and incur medical expenses that are three times (on average) higher than those of normal older individuals. 25 Therefore, frailty significantly impacts the health of older individuals, imposing a heavy burden on both families and society as a whole. Therefore, early identification of frailty risk in older patients with PDR and development of relevant preventive measures are particularly important.
Our study findings indicated that an increase in average monthly household income was an independent protective factor against frailty in older patients with PDR, indicating that patients with lower average monthly household income had a higher rate of frailty. This may be due to high-income patients being able to afford the treatment expenses for long-term diabetes complications, having autonomy in seeking medical care, accessing high-quality medical services and professional advice, prioritizing disease management, and ensuring timely and effective treatment, thereby experiencing milder frailty symptoms. 26 Conversely, patients with lower average household income with diabetes complications tend to delay seeking medical attention until experiencing significant discomfort or symptoms, leading to more severe complications and increased frailty.
This study revealed that living alone is an independent risk factor for the development of frailty in older patients with PDR, consistent with previous research findings. A comprehensive literature search was conducted to analyze the association between living alone and frailty. 27 Of the 203 studies reviewed, data from 44 cross-sectional studies (46 cohorts) and 6 longitudinal studies were included in the analysis. The results of the meta-analysis indicated that older adults living alone had a higher likelihood of experiencing frailty than those who did not. Sex-stratified analysis revealed that only men living alone were at an elevated risk of frailty, while women did not exhibit the same risk. Conversely, no significant association was found in the meta-analysis of longitudinal studies. A further systematic review was conducted to investigate the frequency and determining factors of frailty among older individuals residing in community and nursing-home environments. 28 The review included 38 studies involving a total of 150,642 participants. The findings revealed a higher prevalence of frailty among individuals in nursing homes than among those living in community settings. Frailty was found to be significantly linked to various factors, including sociodemographic aspects (such as living alone and reporting poor health), physiological indicators (such as poor sleep quality and low levels of daily activity), behavioral patterns (such as physical inactivity), and health conditions (including chronic illnesses and depression), in both community and nursing-home settings.
This study also revealed that the number of chronic complications of diabetes and the presence of bilateral eye disease are independent risk factors for the occurrence of frailty in older patients with PDR. Cross-sectional studies have revealed a significant link between frailty and prevalent diabetic microvascular complications (DMC) among individuals with T2DM. 29 This research involved a total of 18,062 adults (with an average age of 59.4 ± 7.2 years and 37.4% being female) enrolled in the UK Bio-bank at the baseline. DMC were defined as diabetic nephropathy, diabetic neuropathy, or DR. The participants were categorized as follows: 6101 (33.8%) were classified as nonfrail, 10,073 (55.8%) as pre-frail, and 1888 (10.4%) as frail. Over a median follow-up period of 12.0 years, 3678 cases of DMC were documented, comprising 2213 cases of diabetic nephropathy, 1520 cases of DR, and 673 cases of diabetic neuropathy. In the multivariable-adjusted model, individuals classified as pre-frail or frail demonstrated a significantly higher risk of overall DMC than nonfrail individuals. This association was consistently observed across all subtypes of DMC. These findings suggest that both pre-frailty and frailty are independently associated with an elevated risk of developing DMC in individuals with T2DM. Another study conducted a comprehensive analysis involving 5321 individuals aged 60–95 years as a part of the China Health and Retirement Longitudinal Study. 30 The findings from the analysis revealed that both near and distance vision impairments were linked to a higher prevalence of frailty, irrespective of various influencing factors. The results from the longitudinal examination showed a significant association between incident frailty and various visual impairments such as glaucoma, distance vision impairment, near vision impairment, and general vision issues. Moreover, the study highlighted a correlation between vision issues and reduced handgrip strength over time. Furthermore, individuals diagnosed with glaucoma, distance vision impairment, or general vision problems exhibited a decrease in gait speed compared with those in the control group. The abovementioned studies have all confirmed a close relationship between frailty and the number of complications in diabetic patients and the decline in bilateral visual acuity, which is highly consistent with our research. This highlights the need for healthcare professionals to pay adequate attention to this issue.
This study revealed that social support serves as a protective factor for older patients with PDR. The findings of this study revealed a significant negative correlation between the total score of social support and scores in various dimensions with the score of frailty. 31 This suggests that the higher the level of social support, the lower the frailty score. Conversely, the lower the score of social support, the higher the score of frailty. Despite the mounting evidence regarding the impact of social factors on frailty in the older population, the precise effect of social support remains ambiguous. A research endeavor evaluated the relationship between social support and frailty progression among older adults residing in the community. 32 Through the utilization of a cohort study framework, a total of 1059 seniors from the Berlin Initiative Study were monitored over a span of 2.1 years. The findings derived from adjusted logistic regression analysis demonstrated that individuals with inadequate social support were twice more likely to develop frailty compared with those with robust social support. This research outcome reinforces the significance of social factors in the onset of frailty and underscores social support as a plausible focal point for interventions aimed at preventing frailty in older individuals. Frailty is a complex condition with various physiological and psychosocial components that are closely interconnected. Social support is believed to have a significant impact on frailty, and these pathways can influence each other in a reciprocal manner. 33 At a physiological level, social support is believed to prevent the worsening of frailty by decreasing the burden of disease. Specifically, stronger social support has been associated with a stress-buffering effect, leading to lower cardiovascular reactivity. 34 Additionally, the incidence of frailty may be linked to chronic inflammation mediated by inflammatory cytokines, which have been found to be lower in individuals with robust social support networks. 35 These pathophysiological processes could help explain the lack of a clear association between social support and the transition into frailty. Conversely, social support can also affect frailty through psychological and behavioral pathways. 36 It has the potential to encourage healthy behaviors and improve medication adherence, thereby impacting the progression of frailty. 37
Therefore, medical staff should actively provide health education to older patients with PDR and encourage family members, friends, and colleagues to offer emotional and material support to these patients. This support can include sharing self-care knowledge and skills, providing motivating visits, and increasing the patient’s level of social support, ultimately reducing the occurrence and development of frailty. 38
This study had several limitations. First, the cross-sectional design of the study prevented the establishment of causal relationships between variables. Second, the limited sample size and data from two centers indicated the need for future prospective multicenter studies and improved sampling methods to clarify the causal relationships between variables for more generalizable results. Third, the frailty instrument utilized focused solely on the frailty phenotype, specifically physical frailty, without exploring varying degrees of frailty. Therefore, this study could not investigate other dimensions of frailty or transitions between different levels of frailty among frail individuals. Fourth, any intervention strategy must incorporate considerations for visual impairments and emphasize psychosocial support as a critical component. However, the current study did not specifically address these factors in its intervention framework, which represents a notable research limitation. Future investigations should prioritize integrating these elements to achieve a more comprehensive and inclusive approach. Finally, the study did not account for the potential impact of other aspects of social isolation such as social participation.
Conclusions
Based on a comprehensive review of the existing literature, this is the first study to investigate the prevalence of frailty and its independent influencing factors among older patients with PDR. The findings of this research provide a basis and potential direction for future studies focusing on both DR and frailty in the older population. Factors such as average monthly family income, living situation, number of diabetes complications, number of diseased eyes, and social support play independent roles in influencing the occurrence of frailty in this population. In the future, targeted interventions can be developed based on these modifiable influencing factors to achieve the goal of preventing or reversing frailty.
Footnotes
Acknowledgement
We acknowledge the contributions of the staff in Baoding No. 1 Central Hospital who aided the efforts of the authors.
Authors’ contributions
Jie Li: Study design and manuscript writing; Kai Wang and Bei Yuan: Collection and analysis of clinical data; Na Chen and Yueling Zhang: Formal analysis, literature review and revision. All authors contributed to the article and approved the submitted version.
Consent for publication
Written informed consent was obtained from the patient for the publication of this study.
Data availability statement
The original contributions presented in the study are included in the article, and further inquiries can be directed to the corresponding author.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Baoding No. 1 Central Hospital. All methods were performed in accordance with the relevant guidelines and regulations. Written informed consent for participation in this study was obtained from the patient’s representative, as required by the national and local guidelines.
Funding
This study was supported by Baoding Science and Technology Plan Self-financing Project (2141ZF253).