
Abstract
Background
Previous studies have shown that soluble growth-stimulated expression gene 2 protein (sST2) plays a significant role in the progression of maintenance hemodialysis. However, the relationship between sST2 and cardiovascular events in maintenance hemodialysis patients remains largely understudied.
Method
This study systematically searched PubMed, Wanfang, and other Chinese and English databases for all published studies on sST2 in maintenance hemodialysis. Relevant literature meeting the requirements was screened, and relevant data were extracted accordingly. The Newcastle–Ottawa Scale was used to evaluate the quality of the selected studies. Publication bias was assessed via funnel plots and Egger’s test. A meta-analysis was performed using either a random-effects or fixed-effects model, as appropriate.
Results
A total of 10 high-quality studies were included in this study, with no significant publication bias. The meta-analysis revealed that sST2 level was associated with the incidence of cardiovascular events in maintenance hemodialysis patients (mean difference = 18.89, 95% confidence interval: 13.93–23.84; p < 0.001). Moreover, elevated sST2 levels were correlated with a higher risk of cardiovascular events (odds ratio = 2.89, 95% confidence interval: 1.71–4.89; p < 0.0001).
Conclusion
sST2 may serve as a predictive biomarker for cardiovascular events in maintenance hemodialysis patients.
Keywords
Introduction
Chronic kidney disease (CKD) is a major public health concern globally, affecting approximately 0.042% of the world’s population. 1 Compared with age- and sex-matched individuals without kidney disease, patients with CKD are associated with a 3-fold higher incidence of cardiovascular disease (CVD) and a 10-fold increase in cardiovascular mortality among dialysis patients. 2 Hemodialysis serves as one of the main treatments for patients with end-stage renal disease (ESRD), with approximately 0.578 million patients with ESRD in China relying on maintenance hemodialysis (MHD). 3 Although MHD can improve the survival rate of patients, CVD remains a major complication. Epidemiological surveys suggest a high prevalence of CVD among MHD patients in China at up to 45.7%, which is a significant contributor to mortality. 4 Although studies on MHD biomarkers have been extensively conducted worldwide, there is a lack of accurate predictors of cardiovascular events in MHD patients.
The accumulation of uremic toxins in the body during end-stage CKD may enhance leucocyte oxidative activity and promote infiltration of macrophages and monocytes into vascular atherosclerotic lesions, which may cause microinflammation of blood vessels, thereby promoting the occurrence of coronary atherosclerotic heart disease. 5 Growth-stimulated expression gene 2 protein (ST2), a member of the interleukin-1 (IL-1) family, exists as two major isoforms—ST2 ligands (ST2L) and soluble ST2 (sST2). It plays a key role in inflammation and immune regulation in vivo. 6 Current evidence suggests that sST2 plays an important role in CVDs such as coronary heart disease and heart failure. 7 Accordingly, sST2 has emerged as a promising biomarker in CVDs. However, its clinical utility may be limited by its relatively low specificity and potential measurement variability due to inconsistencies in diagnostic reagents. These factors could compromise the accuracy and reliability of sST2 analysis. Overall, the relationship between sST2 and CVD incidence in MHD patients remains incompletely understood.
Based on the above evidence, we speculate that sST2 may be associated with cardiovascular events in MHD patients.
Methods
A literature search was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (https://www.bmj.com/content/372/bmj.n160). The search encompassed PubMed, Web of Science, Wanfang, and other major Chinese and English databases from inception until 30 December 2023, using the following search strategy: “hemodialysis” [Title] OR “maintenance hemodialysis”[Title] OR “MHD”[Title] AND “sST2”[Title] OR “soluble ST2”[Title] OR “soluble growth stimulated expression gene 2 proteins” [Title] AND “cardiovascular diseases”[Mesh] OR “cardiovascular events”[Title] OR “CVD” [Title] OR “myocardial infarction”[Title] OR “MI”[Title] OR “heart failure”[Title] OR “HF”[Title] OR “congestive heart failure”[Title] OR “cardiac death”[Title] OR “acute coronary syndrome”[Title] OR “ACS”[Title] OR “angina pectoris”[Title] OR “arrhythmia”[Title] OR “malignant arrhythmia”[Title].
Two reviewers independently screened the literature in accordance with the Translating Research into Practice (TRIP) guideline.
Ethical statement
As this study involved secondary analysis of previously published data, an institutional ethics review was not required.
Literature selection
The inclusion criteria were as follows: (a) study designs including prospective studies, cohort studies, retrospective studies, and case–control studies; (b) studies investigating the correlation between sST2 and cardiovascular events in MHD patients; (c) studies reporting value or range of sST2; and (d) provision of valid effect estimates (e.g. hazard ratio (HR), odds ratio (OR), and 95% confidence interval (CI)) or p values. The exclusion criteria were as follows: (a) reviews, case reports, case series, and letters; (b) studies with incomplete data; and (c) duplicate studies.
Two reviewers independently reviewed and screened the included studies, and disagreements were resolved through consultation with a third reviewer.
Data extraction
Two authors systematically extracted the following data from the full-text articles: first author, publication time, sample size, grouping information, male sex proportion, age of patients, outcome events, and follow-up time. sST2 was measured in ng/mL via enzyme-linked immunosorbent assay in all included studies. Quality assessment was performed according to the Newcastle–Ottawa Scale (NOS), 8 with studies scoring ≥6 stars (of a maximum 9 stars) considered high-quality and eligible for meta-analysis inclusion. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to rate the quality of all studies.
Statistical analysis
Statistical analysis was conducted using RevMan 5.3 (Cochrane Collaboration). Categorical variables were expressed as percentages, and continuous variables were expressed as means ± standard deviations. Study heterogeneity was assessed using the I2 statistic, with I2 values >50% indicating significant heterogeneity, warranting a random-effects model. On the contrary, I2 values <50% indicated no significant heterogeneity among studies, warranting a fixed-effects model. HRs and 95% CIs were calculated using random-effects/fixed-effects models. Sensitivity analyses and funnel plots were used to evaluate publication bias, with p < 0.05 indicating statistical significance.
Results
Literature screening
Our systematic search yielded 483 studies across six Chinese and English databases. After removing duplicates, 215 articles remained. Twenty-two relevant articles were identified based on title and summary review. After reading the full text, 12 articles were excluded (8 were excluded due to a lack of relevant data, and 4 were excluded as they were reviews). Finally, we identified 10 articles for the meta-analysis, including 9 Chinese articles and 1 English article. The flowchart of the literature screening process is shown in Figure 1.
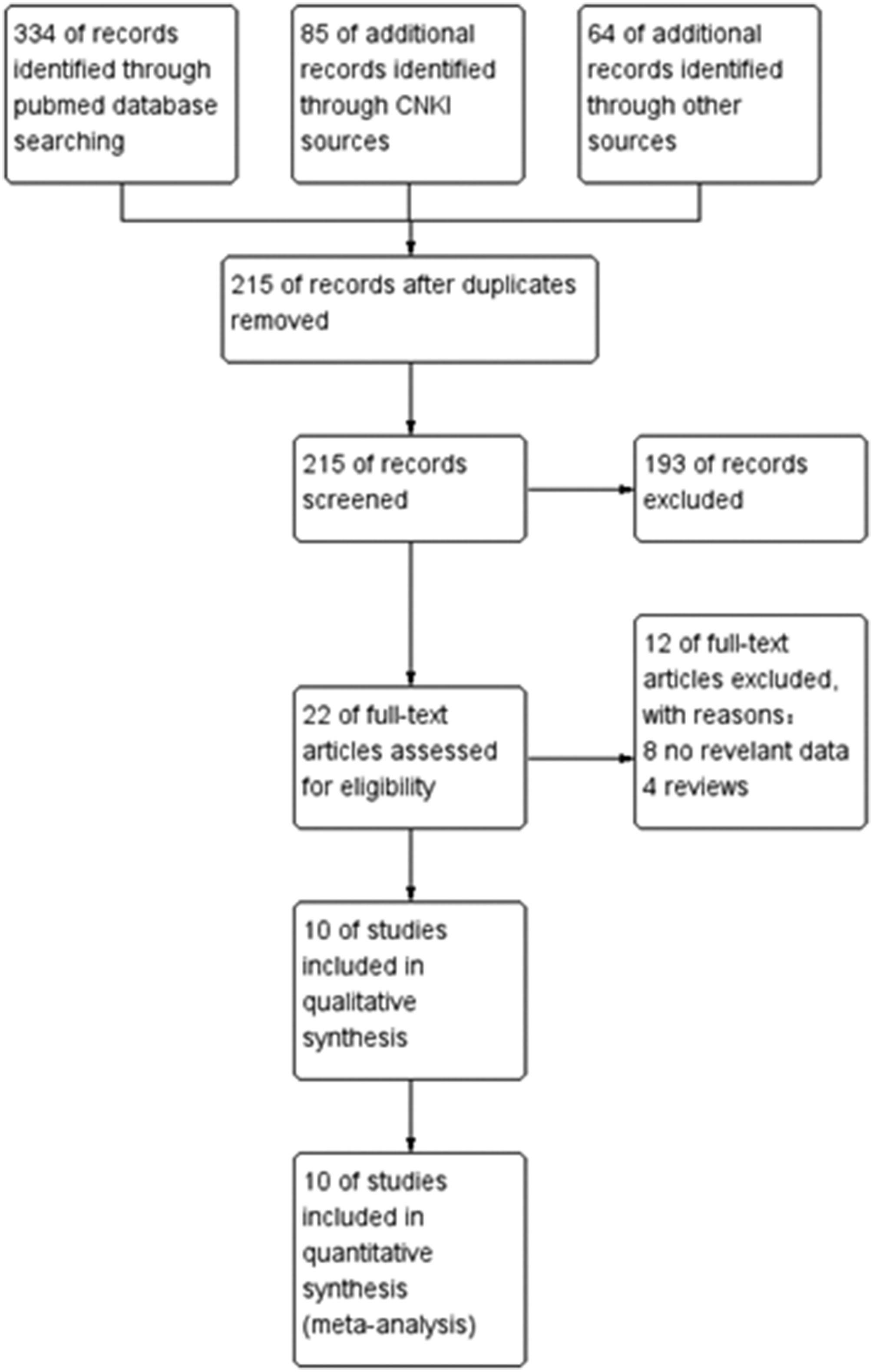
Flowchart depicting the literature screening process.
Basic characteristics of the included studies
The meta-analysis included data from 10 studies,9–18 with a total of 1456 patients, including 842 men (57.8%). Detailed study characteristics, including grouping, average age, follow-up duration, and endpoint events, are described in Table 1.
Characteristics of the included literature.

CVD: cardiovascular disease; HD: hemodialysis; HF: heart failure; MHD: maintenance hemodialysis; sST2: soluble growth-stimulated expression gene 2 protein.
ACS: acute coronary syndrome; CHF: congestive heart failure: HF: heart failure; MI: myocardial infarction.
Correlation between sST2 and cardiovascular events
Among the 10 studies included in the analysis, eight reported serum sST2 levels among MHD patients in the CVD and non-CVD groups. The meta-analysis showed a significant correlation between sST2 levels and cardiovascular events of MHD (mean difference (MD) = 18.89, 95% CI: 13.93–23.84; p < 0.001; Figure 2(a)). In addition, two studies categorized patients into sST2-elevated and sST2-reduction groups according to the sST2 level. Our analysis showed that MHD patients in the sST2-elevated group were more susceptible to CVD than those in the sST2-reduction group (OR = 2.89, 95% CI: 1.71–4.89; p < 0.0001; Figure 2(b)).

(a) Meta-analysis of sST2 levels in MHD patients with CVD. (b) Meta-analysis of sST2 levels and CVD risk in MHD patients and (c) Subgroup analysis based on follow-up time. sST2: soluble growth-stimulated expression gene 2 protein; MHD: maintenance hemodialysis; CVD: cardiovascular disease.
Subgroup analysis (database)
We next conducted a subgroup analysis based on follow-up duration (<2 years vs. >2 years). We found that the correlation between sST2 level and CVD rate became more apparent with prolonged follow-up time (Figure 2(c)). The pooled effect sizes were 18.50 (16.42, 20.57) and I2 = 0% in studies with >2-year follow-up and 26.34 (23.93, 28.75) and I2 = 25% in studies with <2-year follow-up. The overall group exhibited substantial heterogeneity (I2 = 84%), indicating that the follow-up time was an important confounding factor affecting the outcome events. Accordingly, baseline sST2 level can serve as a robust predictor of the incidence of CVD.
Literature quality assessment
The quality of all included articles was evaluated using the NOS. Of the 10 included studies, 7 achieved a score of 6 and 3 achieved a score of 5, indicating acceptable quality for inclusion in the meta-analysis (Tables 2 and 3).
NOS quality scores for the included case–control studies.

NOS: Newcastle–Ottawa Scale.
NOS quality scores for the included cohort studies.

NOS: Newcastle–Ottawa Scale.
Sensitivity analysis and publication bias assessment
Sensitivity analysis demonstrated that the results were stable and reliable (Figure 3(a)). The funnel plot (Figure 3(b)) and Egger’s test (p = 0.091) indicated no significant publication bias among the included studies. A leave-one-out sensitivity analysis was used to evaluate the source of heterogeneity. After excluding two articles,12,13 the I2 value decreased to 42%, significantly reducing the heterogeneity, with an MD of 19.02 (95% CI: 17.58–20.47, p < 0.00001) (Figure 4). Overall, the results remained consistent. Accordingly, our findings suggest that elevated sST2 is a risk factor for CVD events in patients undergoing MHD.

(a) Sensitivity analysis and (b) Funnel plot.

Forest plot of sensitivity analysis.
GRADE assessment
As most studies included in this meta-analysis were retrospective, we conducted a subgroup analysis based on the evaluation indicators of the included studies used for the GRADE assessment to further evaluate the reliability of the conclusions. We adjusted the GRADE scores based on study design, risk of bias, inconsistency, imprecision, and other relevant factors. The final GRADE ratings for both groups were very low (Table 4).
GRADE scores.

CVD: cardiovascular disease; sST2: soluble growth-stimulated expression gene 2 protein; OR: odds ratio; MD: mean difference; GRADE: Grading of Recommendations Assessment, Development and Evaluation.
Correlation between N-terminal pro-brain natriuretic peptide (NT-proBNP) and cardiovascular events
Among all included studies, only three reported patients’ NT-proBNP levels. The meta-analysis revealed a pooled effect size of 7.93 (95% CI: −6.94 to 22.81) for NT-proBNP. Due to substantial heterogeneity (I2 > 50%), we performed a sensitivity analysis by removing the study contributing most to the heterogeneity. The adjusted effect size was 7.03 (95% CI: −5.60 to 19.65); however, significant heterogeneity persisted, and the 95% CI crossed the null line. These findings suggest that based on current data quality, NT-proBNP may not serve as a reliable predictive biomarker for CVD (Figure 5(a) and (b)).

(a) Meta-analysis of NT-proBNP levels in MHD patients with CVD. (b) Meta-analysis of NT-proBNP levels in MHD patients with CVD after removing articles with high heterogeneity. NT-proBNP: N-terminal pro-brain natriuretic peptide; MHD: maintenance hemodialysis; CVD: cardiovascular disease.
Discussion
This meta-analysis found a correlation between sST2 and the incidence of cardiovascular events in MHD patients, with an increased incidence of cardiovascular events observed at high sST2 levels. However, although sST2 levels were significantly higher in patients with CVD, the GRADE assessment indicated a very low quality of evidence, suggesting that the results may be affected by measurement bias and confounding, warranting validation in prospective studies. Although the association between elevated sST2 and CVD risk was substantial, it was based on only two studies with small sample sizes. Further large-scale studies are needed to confirm these findings.
The increased incidence of CVD in patients with CKD is not only associated with traditional CVD risk factors, such as age, sex, diabetes, hypertension, dyslipidemia, smoking, but also with factors related to CKD, including estimated glomerular filtration rate, albuminuria, calcium and phosphorus metabolism disorders, and uremic toxins. 19 In addition, intestinal microbial dysbiosis can affect immune cells, leading to kidney cell activation and increased accumulation of uremic toxins, thereby promoting CVD. 20 Left ventricular hypertrophy reportedly develops in approximately 69% of children, 75% of adult patients at the start of dialysis, and almost 100% of patients after 5 years of dialysis. 21 Some studies have shown that men have a higher risk of mortality than women prior to dialysis, whereas women undergoing dialysis have a higher risk of mortality and a greater risk of cardiovascular events than men. 22 This poses a major threat to the health of dialysis patients.
Interleukin (IL)-33, a member of the IL-1 family, is synthesized by cardiac fibroblasts. The binding of IL33 to ST2L can inhibit nuclear factor kappa B activity induced by angiotensin II and phenylephrine, thereby exerting an anti-cardiomyocyte hypertrophy effect. 23 sST2 has been established as a biomarker for various CVDs. In a group of patients admitted for all forms of CVD, including acute coronary syndrome, heart failure, and the presence of multiple other cardiovascular comorbidities and risk factors, sST2 was associated with any unplanned readmission due to major adverse cardiovascular events (MACE) within 1 year. 24 In addition, multiple studies have shown that sST2 is associated with peripheral edema and inferior vena cava width. Accordingly, sST2 can be used as a biomarker to evaluate peripheral and central effusions in patients hospitalized primarily for right cardiac decompensation, exhibiting superiority over established biomarkers for cardiorenal disease. 25 As aortic and coronary endothelial cells and immune cells can secrete sST2, sST2 levels may also be elevated during inflammation and immunity. Hemodynamic congestion and inflammation in patients with acute heart failure activate vascular endothelial cells to release inflammatory cytokines, which in turn lead to upregulation of sST2. 26
Common CVD biomarkers, such as NT-proBNP, are persistently elevated in patients with CKD, prompting an increasing number of studies exploring new biomarkers. 27 Among these, sST2 exhibits stability in kidney disease, exhibiting less susceptibility to kidney function and limited influence from dialysis treatment. Thus, sST2 has become a research hotspot in recent years. 28 It is widely believed that sST2 is involved in the progression of CKD, and serum sST2 level is correlated with the severity of patients with CKD, potentially serving as a marker of disease severity. 29 Evidence from a large cohort study involving patients with CKD showed that elevated sST2 was independently associated with an increased risk of all-cause mortality and cardiovascular death (HR = 0.55, 95% CI: 0.36–0.86). 30 Another cohort study observed that decreased levels of sST2 over 2 years were positively associated with the risk of heart failure and atrial fibrillation in patients with CKD (HR = 1.90, 95% CI: 1.14–3.18), whereas NT-proBNP levels remained comparable. This suggests that sST2 is a more sensitive predictor of CVD in patients with CKD than NT-proBNP. 31 Our results showed that NT-proBNP might not be a suitable predictor of CVD in MHD patients. In a prospective follow-up study, MHD patients with elevated sST2 levels exhibited significantly increased mortality at 1 and 3 years, representing the only independent predictor of short-term death. 32 Serum levels of sST2 are significantly increased in patients with heart failure, and sST2 is associated with the prognosis of patients with coronary artery disease and heart failure, consistent with the results of this study. 33 However, some studies have suggested that the increase in sST2 level is not significantly related to the occurrence of atherosclerotic CVD, potentially due to the primary role of intravascular plaque deposition in atherosclerotic CVD, with myocardial cell remodeling playing a less significant role. Further prospective studies are warranted to verify the association between sST2 and atherosclerotic CVD. 34
This study had limitations that should be acknowledged. Most of the studies included in this meta-analysis were retrospective in nature and conducted in China, which may limit the generalizability of our findings to other populations. Future studies should prioritize prospective studies from other countries and regions to verify the accuracy of these conclusions. In addition, the single-center design of many included studies, coupled with potential variations in detection platforms, may increase the heterogeneity to a certain extent. Future studies should focus on differences in detection platforms and minimize the heterogeneity among studies. Although Egger’s test in this study yielded a p value of 0.091, suggesting no significant publication bias in the included studies, the limited number of included studies in this meta-analysis raises the possibility of potential publication bias. Sensitivity analysis and funnel plot showed that the results of the study were reliable, with a 95% CI for the effect size being 13.93–1.71, suggesting that sST2 was clinically associated with CVD. Indeed, these conclusions warrant further validation in larger prospective studies. Previous research on the association between sST2 and CVD events in MHD patients has often been limited to single-center clinical studies. Although one meta-analysis explored the association between sST2 and all-cause mortality in MHD patients, this meta-analysis included only four studies and did not analyze the association between sST2 and CVD, despite potential publication bias and methodological differences. The larger sample size and robust sensitivity analysis in this study support the clinical value of sST2 in CVD events among MHD patients. However, future studies should standardize sST2 measurements, include more European and American populations, incorporate RCTs, and extend the follow-up to further verify the conclusions. Finally, the study review process may have been subject to subjective bias.
Conclusion
This study highlights the association between sST2 and cardiovascular events in MHD patients. sST2 is expected to be an early biomarker for predicting cardiovascular events in MHD patients in the future.
Footnotes
Acknowledgements
We are grateful to the researchers who previously worked on these research areas.
Author contributions
Ze Zhang completed literature collection, screening, data analysis, and article writing; Tao Yang completed literature collection and screening; Mengya Zhao completed literature screening and data analysis; and Huaqian Chen completed review and revision of the article.
Data availability statement
The data that support the findings of this study are available in these public databases, including PubMed, Web of Science, Wanfang, and CNKI.
Declaration of conflicting interests
The authors have no financial or non-financial competing interests to declare.
Funding
There was no financial support for this study.