
Abstract
Continuous epidural anesthesia is a classic anesthesia method that is widely used in abdominal surgery, labor analgesia, and postoperative analgesia. A long-term analgesic effect is achieved by continuously injecting local anesthetics into the epidural space through an epidural catheter. However, the insertion of epidural catheters is associated with various complications, such as total spinal anesthesia, nerve damage, bleeding, infection, and catheter distortion with difficult catheter removal. We present the case of a parturient woman who underwent vaginal delivery under epidural analgesia. However, after delivery, the epidural catheter could not be pulled out. Spinal computed tomography and three-dimensional reconstruction revealed that the catheter was coiled but not knotted in the spinal facet joints. Using optimal position simulation, we successfully pulled out the epidural catheter. This case demonstrates that spinal computed tomography reconstruction with optimal position simulation may be the most effective noninvasive method for successfully removing a trapped epidural catheter.
Keywords
Introduction
Continuous epidural anesthesia is a well-established anesthetic technique widely employed in abdominal surgeries, labor analgesia, and postoperative pain management. This method demonstrates prolonged analgesic effects through the continuous administration of local anesthetics into the epidural space via an indwelling catheter. However, epidural catheter placement is associated with inherent risks, including but not limited to total spinal anesthesia, neural injury, hemorrhage, infection, and catheter malpositioning with subsequent difficult removal. Although difficulty in removing an epidural catheter is rarely observed, with an incidence of approximately 0.012%, 1 it poses considerable mental burden on the patient when it occurs. Surgical procedures may be required to remove the indwelling catheter, leading to additional pain. In this case, we successfully extracted the trapped epidural catheter using three-dimensional spinal computed tomography (CT) reconstruction and optimal position simulation of the spinal model. This noninvasive method is expected to become the most efficient strategy for removing a trapped epidural catheter.
Case report
A 23-year-old woman, with a height of 164.0 cm, weight of 85.0 kg, and body mass index (BMI) of 31.6 kg/m2, underwent vaginal delivery under epidural analgesia at Xiushan Tujia and Miao Autonomous County People’s Hospital of Chongqing in November 2024. Preoperative examination showed no abnormality. At 10:00 AM on the day of the operation, the anesthesiologist performed continuous epidural anesthesia in the right lateral position. A midline puncture through the L2-3 intervertebral space was performed using a 16-gauge epidural puncture needle (Henan Tuoren Medical Device Company Ltd., Henan, China), and a reinforced catheter with a length of 4 cm was indwelled in the epidural space. A mixture of ropivacaine hydrochloride (9 mg) and sufentanil (4.5 μg) was administered. The anesthesia level was T10-L1 with almost no change in vital signs, and the visual analog scale pain score was 3 points. At 11:00 AM, the catheter slipped out of the epidural space. Epidural puncture was performed again. The parturient woman was lying on her right side; after performing a midline puncture through the L1-2 intervertebral space, a sensation of ligamentum flavum penetration was experienced at a depth of approximately 7 cm. The reinforced epidural catheter was inserted until a depth of 13 cm on the scale. The initial placement resulted in 6 cm of the catheter remaining within the epidural space following needle withdrawal. Subsequent attempts to adjust the catheter to the intended length of 5 cm proved unsuccessful due to resistance; ultimately, 6 cm of catheter depth was maintained within the epidural space. Despite maximal flexion positioning in the right lateral decubitus position, catheter removal remained unachievable. Saline injection through the catheter was performed to assess both catheter patency and proximity to neural structures. The injection demonstrated minimal resistance and elicited no signs of nerve root irritation in the parturient woman. Therefore, we decided to use the epidural catheter for labor analgesia and then attempted to extubate it after delivery. A test dose of 5 mL of 1% lidocaine was administered through the catheter, and the anesthetic level of T12-L1 was reached 5 min later. A mixture of ropivacaine hydrochloride (9 mg) and sufentanil (4.5 μg) was injected into the epidural space uneventfully, and the anesthesia level reached T10-S 15 min later. Then, an epidural pulse analgesia pump was connected. Continuous vital sign monitoring was maintained throughout the procedure, with no clinically significant deviations observed.
The parturient woman successfully delivered a baby through the vagina at 02:00 PM with an Apgar score of 10. Two hours after the delivery, the anesthesiologist tried the left-side position, right-side position, and sitting position again for epidural catheter removal, simultaneously adjusting the degree of spinal flexion. The anesthesiologist also injected ice saline to contract the epidural catheter. However, the catheter could not be removed. Imaging studies were performed after obtaining the woman’s informed consent. Spinal CT and three-dimensional reconstruction (Figure 1) revealed that the catheter was coiled but not knotted in the epidural space. An orthopedic spine surgeon was consulted to leverage their subspecialty expertise in spinal anatomy. The surgeon suspected that the catheter was trapped in the spinal facet joints. Various positions were simulated using the spinal model, and it was found that the prone position with a thick pillow placed beneath the lower abdomen could open the facet joints to the greatest extent (Figure 2). The complete catheter was successfully pulled out in the same position (in the prone position with a thick pillow placed beneath the lower abdomen); the catheter remained intact without becoming thinner (Figure 3). The parturient woman did not experience any adverse reactions. At 7 days of follow-up, there were no complications. This case report was published with the written consent of the parturient woman and conformed to the Case Report (CARE) guidelines. 2

Spine computed tomography reconstruction.

Simulation of the optimal position using a spinal model for opening the facet joints to the greatest extent.

Successfully pulling out of the complete catheter.
Discussion
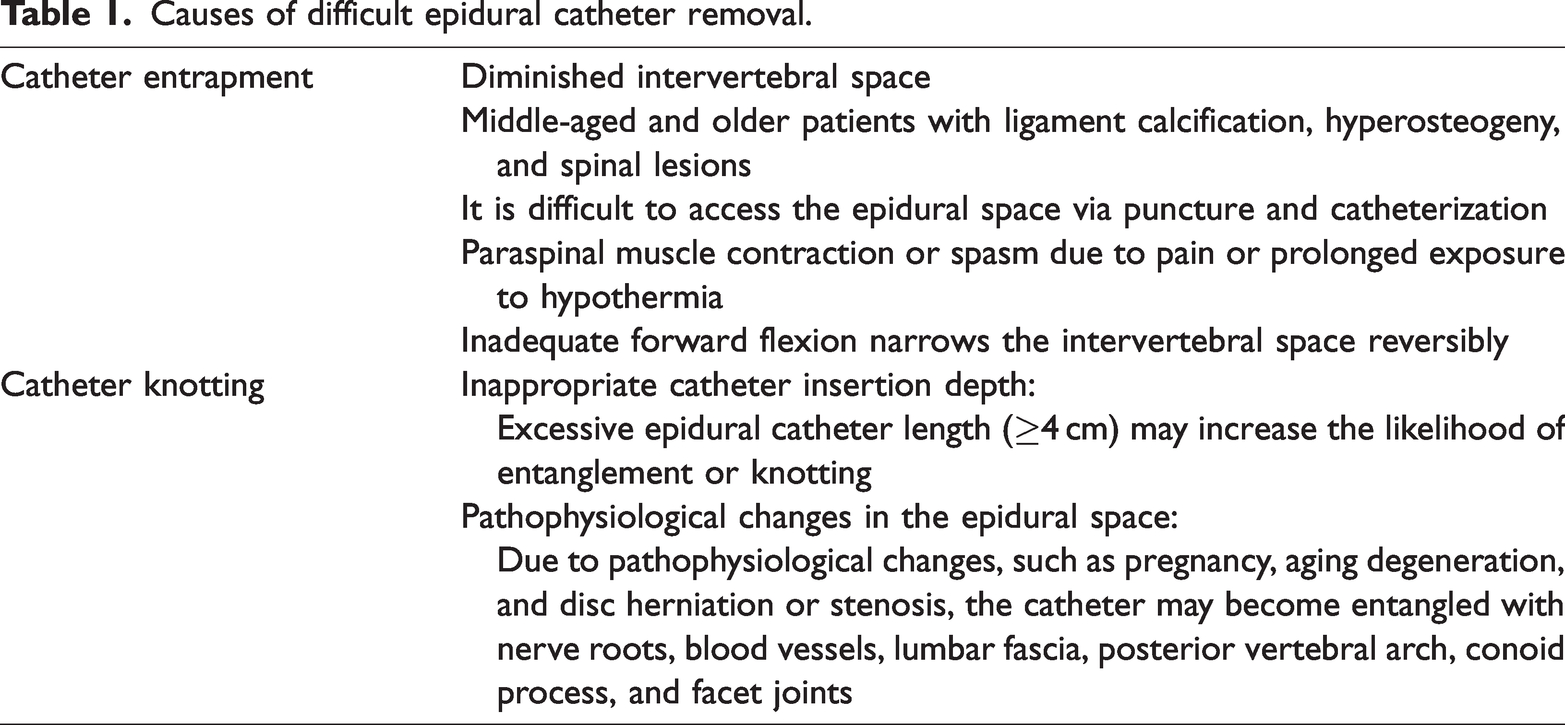
Twenty-three difficult epidural catheter removal cases have been reported in the PubMed database from 1978 to 11 December 2024 (Supplemental Table 1). Thus, it is important to explore effective noninvasive methods to remove trapped epidural catheters. Table 1 summarizes the causes of difficult epidural catheter removal. 3 In this case, we found that the epidural catheter was trapped in the facet joints of the spine. There are three reasons attributed to the difficulty of catheter removal. First, the catheter length in the epidural space was excessive. The catheter slipped out 1 h post-insertion, with 4 cm of the catheter residing within the epidural space during the first epidural analgesia administration. To prevent recurrent displacement during subsequent epidural analgesia administration, the catheter was advanced 2 cm beyond the conventional depth, which subsequently led to difficult catheter removal. Current recommendations suggest limiting the initial epidural catheter insertion depth to ≤5 cm within the epidural space to prevent complications such as catheter knotting or intervertebral foramen migration. 4 Following needle withdrawal, the catheter should be appropriately withdrawn to maintain an optimal 2–4 cm length within the epidural space. Although shorter catheter length may increase dislodgement risk, the catheter insertion depth should not exceed the conventional depth of ≤5 cm in the epidural space. Appropriate catheter fixation technique is essential to prevent migration while avoiding excessive tension. Second, secondary contributing factors included pathophysiological alterations associated with elevated BMI, particularly lumbar disc protrusion and spinal canal stenosis, which compounded catheter extraction challenges. Third, the puncture point may not be the median position of the intervertebral space, which facilitated catheter migration into the articular processes.
Causes of difficult epidural catheter removal.
In cases where the epidural catheter is trapped, the patient and her family members should be fully explained the situation in a timely manner to reduce their fear and discomfort. The following eight methods are used to deal with the difficulty of removing an epidural catheter: (1) Pull with continuous gentle force and stop when the catheter is stretched and thinned to prevent the catheter from breaking. 5 (2) Maintain a warm temperature and provide adequate analgesia to prevent paravertebral muscle contraction or spasm due to hypothermia and pain at the exposed site. (3) Try to extubate after the patient has completely calmed down. 6 (4) Try to change the patient’s position and restore the puncture position.7,8 Generally, it is not recommended to pull out the epidural catheter in the sitting position. While sitting, as greater force is applied to the spine, greater resistance will be encountered when pulling out the catheter. The force required to remove the epidural catheter is 2.5 times greater in the seated position than in the lateral position. 6 (5) Inject ice saline through the epidural catheter to lubricate and contract the catheter. (6) Find the cause of difficulty in epidural catheter removal through imaging, 9 such as CT, X-ray, and fluoroscopy, and then try the best position for noninvasive epidural catheter removal. (7) In cases where the cause of catheter entrapment has been identified and all of the above methods have failed, a dual-lumen central venous catheter dilator can be used as a guide to pull out the catheter. 10 The central venous catheter dilator is not easy to break, has no inclined front end, is round and blunt, and does not easily puncture the epidural catheter. Simultaneously, it has a certain toughness that can change the direction of needle insertion and squeeze into the space of facet joints, which releases the catheter that is incarcerated between the bone spaces. In addition, nitinol sutures have been used as guide wires to remove the epidural catheters. 11 (8) Remove the catheter through a surgical procedure under local anesthesia or general anesthesia via imaging.12–14 However, methods 7 and 8 are invasive and can cause additional pain to the patient.
In this case, the epidural catheter could not be successfully removed after trying methods 1–5; thus, imaging examinations were performed. It was found that the epidural catheter could be trapped in the facet joints of the spine. The spinal model was further used to simulate the entanglement position of the epidural catheter to find the best physiological position for separating the facet joints. The prone position with a thick pillow beneath the lower abdomen was optimal for opening the facet joints (Figure 3). Finally, the complete epidural catheter was successfully removed under this position, avoiding the invasive approach. Similarly, a woman undergoing epidural postoperative analgesia for a fracture experienced difficulty in epidural catheter removal. Epidural catheter angiography showed that the catheter was fixed in the anterior epidural space without knot and distortion, and it was successfully removed after the patient was made to lie in the prone position and a pillow was placed under the abdomen. 15 Deng et al. 16 successfully pulled out a knotted epidural catheter in the left lateral position with the left lower limb extended and the right lower limb flexed at a 90° angle under the guidance of CT and spinal model. The anesthesiologist applied pressure to the patient’s right hip joint, pushing it forward with the right hand. This maneuver effectively separated the spine’s facet joints; however, it was more complicated than the present case. These results indicate that combined spinal reconstruction with optimal position simulation may be the most effective noninvasive method to remove a trapped epidural catheter.
In conclusion, we report the case of a parturient woman with a trapped epidural catheter. Three-dimensional spinal CT reconstruction showed that the catheter was trapped around the facet joint of the spine. Then, the optimal position for exposing the facet joints was simulated using the spinal model, and it turned out to be the prone position with a thick pillow placed beneath the lower abdomen. Finally, the catheter was removed entirely under the optimal position, avoiding additional surgery and trauma to the patient. This method may be the most effective noninvasive method for removing a trapped epidural catheter.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251340316 - Supplemental material for Removal of a trapped epidural catheter via spinal computed tomography reconstruction and optimal position simulation of the spinal model: A case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605251340316 for Removal of a trapped epidural catheter via spinal computed tomography reconstruction and optimal position simulation of the spinal model: A case report by Yang Liu, Jin Yang, Xun Zhu, Jingjing Wu, Qi Hu and Ai Yan in Journal of International Medical Research
Footnotes
Acknowledgments
The authors gratefully acknowledge all participants for their contribution to this study.
Author contributions
YL: Conceptualization, Writing—original draft. JY: Conceptualization, Writing—original draft. XZ: acquisition, analysis, and interpretation of data. JJW: Data curation. QH: Formal analysis. AY: Conceptualization, Writing—review & editing, Funding acquisition. All authors have read and approved the final manuscript and agreed to be accountable for all aspects of the work.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, and further inquiries can be directed to the corresponding authors.
Declaration of conflicting interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethics statement
Ethical approval was not required for this study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.
Funding
This work did not receive any funding.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.