
Abstract
Patients with cirrhosis may experience neurologic complications, including hepatic encephalopathy. Hepatic encephalopathy may be classified as covert (mild symptoms (e.g. lack of awareness)) or overt (moderate to severe symptoms (e.g. confusion or coma)), and symptoms may overlap with other neurologic conditions (e.g. epilepsy, stroke). Managing hepatic encephalopathy includes identifying and treating precipitating factors (e.g. dehydration). First-line treatment for patients with overt hepatic encephalopathy is typically lactulose; to reduce the risk of overt hepatic encephalopathy recurrence, lactulose plus the nonsystemic antibiotic rifaximin is recommended. Rifaximin reduced the risk of breakthrough overt hepatic encephalopathy by 58% versus placebo over 6 months (p < 0.001; 91% of patients in each group were on concomitant lactulose). However, neither pharmacologic hepatic encephalopathy treatment nor liver transplantation may completely reverse neurologic impairment in patients with hepatic encephalopathy. Additional neurologic considerations for patients with cirrhosis include preventing falls, as well as managing sleep-related issues, hyponatremia, and cerebral edema. Thus, monitoring neurologic impairment is an important component in the management of patients with cirrhosis.
Introduction
According to data from the National Health and Nutrition Examination Survey (NHANES), cirrhosis affects an estimated 0.3% of US adults (1999–2010 data). 1 However, some individuals may be unaware they have cirrhosis; 68.7% of individuals with cirrhosis included in NHANES indicated they had not been diagnosed with the condition. 1 During the compensated phase of cirrhosis, patients are asymptomatic and generally free of cirrhosis-related complications (e.g. ascites, variceal bleeding, jaundice, hepatic encephalopathy (HE));2,3 the onset of complications marks the transition to decompensated cirrhosis.3,4 The aim of this narrative review is to highlight several potential neurologic complications, with a focus on HE, and other neurologic-related issues that might arise in patients with cirrhosis at either stage of the disease.
Overt HE
HE is typically classified as covert or overt (Table 1).5,6 Because patients with covert HE do not present with clinically apparent symptoms, diagnosing covert HE (minimal HE or modified West Haven (WH) grade 1 HE) requires specialized psychometric, neuropsychologic, or neurophysiologic testing. 6 However, covert HE is associated with decreased quality of life, increased risk for falls, and driving impairment;7–9 falls within the previous year were predictive of poor quality of life in patients with covert HE. 10 Furthermore, covert HE is associated with development of overt HE and increased risk of mortality.11,12

Source: Adapted with permission from Vilstrup. 6
HE: hepatic encephalopathy.
Overt HE is a common neurologic complication of cirrhosis, 13 and symptoms range from lethargy and personality changes (WH grade 2) to somnolence and confusion (WH grade 3) to, in the most severe cases, coma (WH grade 4) (Table 1).5,6 One study reported that patients with grade 2 HE (40%) and grade 3 HE (42%) compose the majority of patients with HE admitted to the hospital. 14
Orientation to time and place are common challenges for patients with more severe overt HE. Because WH criteria are subjective, clinicians adapted a questionnaire used to assess outcomes in patients with traumatic brain injury for use as a modified-orientation log for evaluating patients with HE. 14 The modified-orientation log contains eight questions: five related to time and three related to place. Scores range from 0 (no answer or consistently answering question incorrectly, even with cuing) to 3 (correct answer provided without cuing) for each question, with a total score ranging from 0 to 24. 14 In addition, a newer tool—the Hepatic Encephalopathy Grading Instrument™—was developed to assess HE in clinical practice, in conjunction with a caregiver electronic diary (Figure 1). 15

Hepatic Encephalopathy Grading Instrument. 15
Precipitating factors for HE
According to the guidelines from the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL), treatment of patients with overt HE includes considering other potential causes of altered mental status, identifying and subsequently treating precipitating factors, and initiating drug treatment for overt HE. 6 In a study that examined patients with cirrhosis retrospectively and prospectively, overt HE–related hospitalization was associated with ⩾2 precipitating factors in most patients (101 of 149 patients (67.9%) and 42 of 45 patients (93.3%), respectively). In fact, in these studies, 18% and 47% of patients, respectively, had ⩾4 precipitating factors. 16 The three most common precipitating factors were lactulose (an HE treatment) nonadherence, dehydration, and constipation in the retrospective analysis, and dehydration, acute renal failure, and lactulose nonadherence and infections (latter two tied for third) in the prospective analysis. 16 Other precipitating factors for overt HE included use of certain medications (e.g. opioids, benzodiazepines), electrolyte imbalances (e.g. hypokalemia (potassium <3.5 mEq/L), hyponatremia (sodium <130 mEq/L)), transjugular intrahepatic portosystemic shunts, gastrointestinal bleeding, and paracentesis. 16 Identifying and managing all precipitating factors is an important component of treating patients with overt HE.6,16
Potential misdiagnosis of neurologic conditions in patients with cirrhosis
Given the overlap of some clinical symptoms across neurologic conditions, patients with overt HE might be misdiagnosed with other conditions (e.g. certain forms of epilepsy, stroke).17,18 In one retrospective, single-center study of patients with cirrhosis with a hospital stay, 20 of 2010 (number of patients) (1.0%) patients received an initial diagnosis of epilepsy. 17 Further medical record review determined the true prevalence of epilepsy was 0.7% (n = 15), as 3 of the 20 patients had been misdiagnosed and ultimately were found to have HE. 17 Although epilepsy in patients with cirrhosis is rare, diagnosis of certain forms of epilepsy requires both clinical observation and electroencephalographic testing, given the different readings in patients with epilepsy versus patients with overt HE (Table 2). 17 However, the potential for misdiagnosing epilepsy in patients with HE might be mitigated by a complete medical history and clinical exam. 17
Features of epilepsy and HE by EEG. 17

HE: hepatic encephalopathy; EEG: electroencephalogram.
Patients with HE might also be misdiagnosed with stroke. 18 A retrospective study found an increased risk of stroke in patients with cirrhosis versus patients without the condition (hazard ratio (HR) = 1.8, 95% confidence interval (CI) = 1.5–2.0). 19 One case study reported on a patient with HE who presented with neurologic symptoms compatible with a diagnosis of stroke (i.e. right-sided hemiparesis, right-sided sensory disturbance, Babinski sign, Chaddock sign, impaired language skills, flapping tremors) and initially was misdiagnosed and treated on suspicion of that condition. 18 A diagnosis of HE ultimately was established after researchers found no evidence for stroke based on magnetic resonance imaging and angiography during an examination, along with electroencephalographic results consistent with HE (i.e. triphasic wave). 18 The patient received branched-chain amino acids for HE, with symptom improvement observed. 18
In addition, Wilson’s disease, a rare genetic metabolic condition resulting in disordered copper storage, can progress from hepatic impairment to cirrhosis.20,21 The disease also is associated with neurologic symptoms that have been associated with HE (e.g. ataxia, dysphagia, dysarthria, parkinsonism, apathy, irritability, aggression, disinhibition).
Treatment of overt HE
Typically, first-line therapy for patients with overt HE is the nonabsorbable disaccharide lactulose (Figure 2). 6 Patients should receive 25 mL of lactulose every 1 to 2 hours until ⩾2 soft or loose bowel movements per day are achieved; lactulose should then be titrated to maintain 2 to 3 daily bowel movements. 6 Aspiration is a potential complication of oral lactulose administration in patients with more severe HE (e.g. unconscious patients); caution is warranted with this population. 6 For patients who are hospitalized and unable to swallow or are at risk of aspiration, lactulose can be administered using a nasogastric tube 6 or by enema.
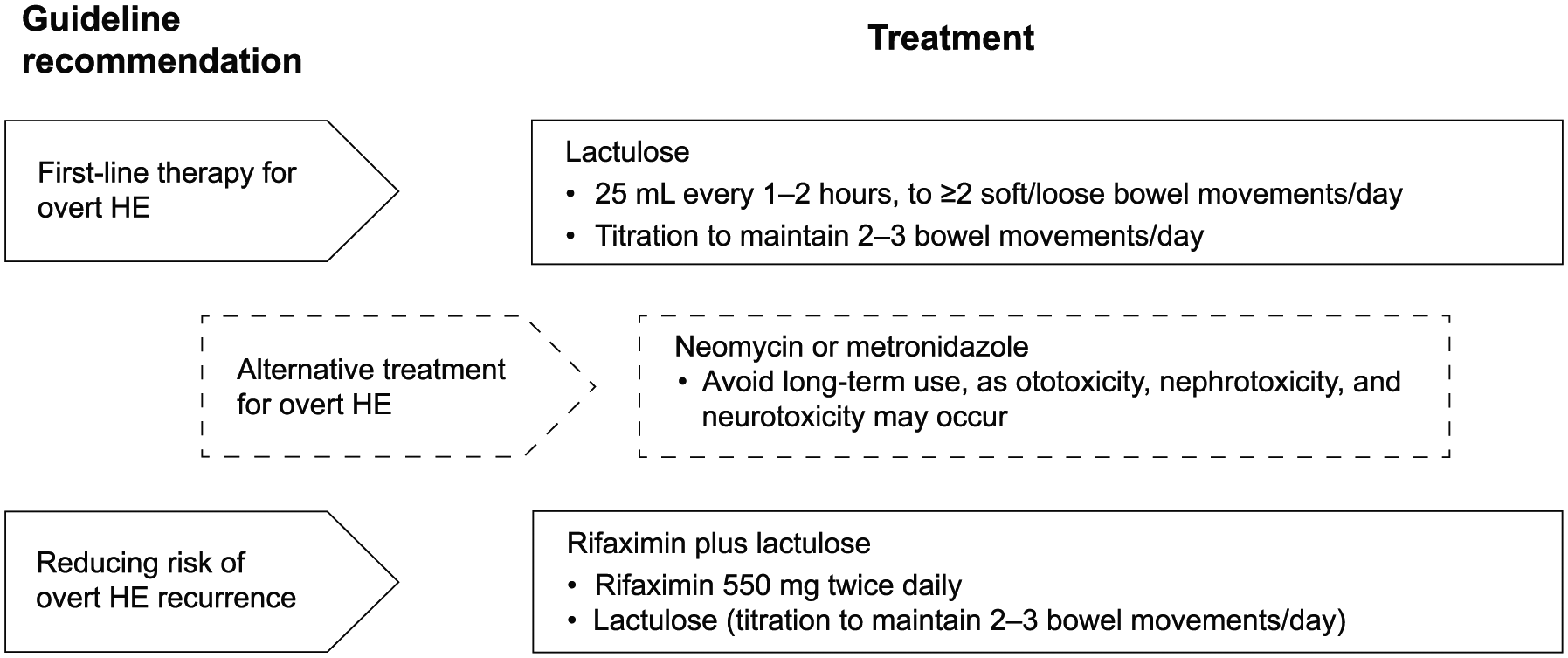
Guideline recommendations for management of patients with HE. 6
However, lactulose is plagued by nonadherence. Data from a single-center chart review of 137 patients reported that recurrence of HE (n = 103) was associated with lactulose nonadherence (n = 39, 37.9%) and lactulose-induced dehydration (n = 8, 7.8%; defined as >4 bowel movements per day with dehydration and azotemia). 22 Lactulose nonadherence (n = 39) was associated with gastrointestinal-related adverse events (AEs), including diarrhea (n = 27), bloating (n = 18), and abdominal pain (n = 16), which resulted in failure of patients to adequately self-titrate lactulose dosing. 22 Furthermore, both retrospective and prospective analyses of patients with HE reported that lactulose nonadherence was associated with recurrence of HE in more than half of patients examined (51.4% and 53%, respectively). 16 Interestingly, the authors also observed that 8 of 137 patients, all of whom were adherent to treatment, developed recurrent HE due to lactulose-associated dehydration (i.e. >4 bowel movements per day with dehydration and azotemia; new increase in serum creatinine >1.5 mg/dL). 22
Guidelines from AASLD and EASL recommend lactulose in combination with the nonsystemic antibiotic rifaximin for the prevention of HE recurrence. 6 In a phase 3, randomized, double-blind, placebo-controlled study, rifaximin 550 mg twice daily (n = 140) reduced the risk of breakthrough overt HE by 58% versus placebo (n = 159) during a 6-month period (HR = 0.42, 95% CI = 0.28–0.64, p < 0.001) in patients with a history of recurrent overt HE (i.e. ⩾2 episodes within previous 6 months). 23 Furthermore, rifaximin significantly reduced the risk of overt HE-related hospitalization versus placebo during 6 months of treatment (HR = 0.50, 95% CI = 0.29–0.87, p = 0.01). 23 Approximately 91% of patients in either group received concomitant treatment with lactulose. 23 In this 6-month study, twice-daily rifaximin was well tolerated. 23 The risk of Clostridium difficile infection with rifaximin was low: two rifaximin-treated patients had a C. difficile infection; both had multiple risk factors for C. difficile infection, including older age, recent hospitalizations during which antibiotics were used, and use of the proton-pump inhibitor pantoprazole. 23
An open-label study that evaluated rifaximin for long-term (⩾2 years) prevention of overt HE recurrence included patients who had received placebo during the original 6-month randomized study, 24 newly enrolled patients with a history of overt HE (new-rifaximin population), and patients who had received rifaximin during the original 6-month randomized study (historical-rifaximin population). 24 The groups were analyzed together (all-rifaximin population) and separately with comparison to the historical-rifaximin or historical-placebo population from the original study. 24 Overall, 89.8% of patients included in the all-rifaximin population received concomitant lactulose. 24 The rates of HE-related hospitalizations were comparable between the all-rifaximin, new-rifaximin, and historical-rifaximin (i.e. 6-month randomized study) populations (0.21 events/person-years of exposure (PYE), 0.23 events/PYE, and 0.30 events/PYE, respectively). 24 Furthermore, the rates of all-cause hospitalizations in the all-rifaximin and new-rifaximin populations were decreased compared with the historical-placebo population from the 6-month randomized study (0.45 events/PYE and 0.44 events/PYE versus 1.30 events/PYE, respectively). 24 No increase in AE rates was observed in the open-label, long-term (⩾2 years) study; four patients in the open-label study—all of whom had multiple risk factors for C. difficile—developed C. difficile infection. 24
Beyond reducing the risk of overt HE recurrence, rifaximin plus lactulose (n = 63) reversed HE in a significantly higher percentage of patients experiencing an overt HE episode versus lactulose alone (n = 57) within 10 days (76% versus 44%, respectively; p = 0.004). 25 Mortality was significantly decreased with rifaximin plus lactulose compared with lactulose alone (24% versus 49.1%, respectively; p < 0.05). 25 However, 81.7% of patients included in this study had WH grade 3 or 4 HE at baseline. 25 Furthermore, data suggest that rifaximin may reduce the risk of other complications of cirrhosis. In one study of patients treated for HE, rifaximin plus lactulose (n = 145) was associated with a reduction in the risk of a variety of complications of cirrhosis versus lactulose alone (n = 276): HE recurrence (HR = 0.45, 95% CI = 0.29–0.72, p < 0.001), developing spontaneous bacterial peritonitis (SBP; HR = 0.21, 95% CI = 0.11–0.40, p < 0.001), variceal bleeding (HR = 0.42, 95% CI = 0.22–0.82, p = 0.01), and mortality (HR = 0.70, 95% CI = 0.51–0.95, p = 0.02). 26
According to AASLD and EASL guidelines, neomycin or metronidazole may be used as an alternative to lactulose alone or lactulose plus rifaximin to treat patients with overt HE, though data are limited. 6 However, chronic use of these two agents should be avoided because of the risk for ototoxicity, nephrotoxicity, and neurotoxicity associated with long-term administration. 6 Although polyethylene glycol 3350-electrolyte solution (PEG) is not recommended in current guidelines, 6 a randomized, single-center US study (n = 50) reported that PEG significantly improved the mean HE grade from baseline compared with lactulose (baseline scores: 2.3 and 2.3, respectively) within 24 hours (1.5 versus 0.7, respectively; p = 0.002). 27 For patients who received either PEG or lactulose, median time to HE resolution was 1 and 2 days, respectively (p = 0.01). 27 In this study, PEG and lactulose were considered generally well tolerated, with no serious AEs (PEG, n = 3; lactulose, n = 5) considered to be “definitely” or “probably” related to treatment. 27
It should be noted that pharmacologic treatment of overt HE and liver transplantation may not completely reverse neurologic impairment in some patients.28,29 Results of a prospective study of patients with cirrhosis reported that, compared with patients without a history of HE (n = 138), those with a history of HE (n = 36) may have persistent learning impairments, as assessed by psychometric testing, despite having received lactulose with or without rifaximin for HE. 28 In addition, while liver transplantation is considered to largely reverse HE impairments, some patients with a history of HE may not experience a complete reversal of cognitive impairment posttransplant; 29 however, ongoing improvement in cognition has been observed during the first year posttransplant. 30
Additional neurologic-related issues to consider for patients with cirrhosis
Health care providers, caregivers, and patients should be aware of several neurologic-related issues affecting patients with cirrhosis, including fall prevention and management of sleep-related issues, hyponatremia, and cerebral edema.
Prevention of falls
A significantly greater percentage of patients with cirrhosis with cognitive impairment had >1 fall during a 1-year period (40.4%) versus patients with cirrhosis without cognitive impairment (6.2%, p < 0.001); furthermore, the group with cognitive impairment had a significantly greater mean number of falls per patient versus the group without cognitive impairment (0.8 versus 0.1, p = 0.003). 31 In addition, patients with cognitive impairment had a significantly greater need for fall-related care (i.e. primary care, emergency department care, or hospitalization) versus patients without cognitive impairment (e.g. emergency room visits, 23.8% versus 2.5%, respectively; p < 0.001). 31 In a retrospective study, intracranial hemorrhage occurred in a significantly greater percentage of patients with cirrhosis with falls or trauma, focal neurologic signs, or history of intracranial hemorrhage, versus patients with altered mental status, headache, or fever (8.9% versus 0.3%, respectively; p < 0.0001). 32 In patients with cirrhosis (n = 118), falls in the previous year negatively affected health-related quality of life (p = 0.001). 33
In a population-based study (n = 3764 per group), fracture incidence rate ratios (IRRs) versus matched controls were significantly greater in patients with cirrhosis and HE (IRR = 1.3, 95% CI = 1.02–1.72, p = 0.03) and patients with cirrhosis without a history of HE (IRR = 1.6, 95% CI = 1.69–2.05, p = 0.001). 34 Cumulative 18-month fracture incidence rates also were significantly greater for patients with cirrhosis with HE (7.1%) and without HE (7.7%) versus matched controls (4.0%; p = 0.001 and p < 0.001, respectively). 34 In a retrospective study of US hospitalized patients with cirrhosis (2010–2013), falls occurred in 55 of 1749 (3.1%) cirrhosis-related hospital admissions. 35 Patients who had taken benzodiazepines and antipsychotic agents were at significantly greater risk for falls (benzodiazepines: odds ratio (OR) = 6.6, 95% CI = 3.8–11.6; antipsychotics: OR = 3.7, 95% CI = 1.9–7.1, adjusted for HE). 35 Although patients with cirrhosis were not at significantly greater risk of experiencing a fall compared with patients in the general hospital population, they were more likely to experience a fall-related injury (rate ratio = 3.4, 95% CI = 2.0–5.7, p < 0.0001). 35 Thus, proactive prevention of falls should not be overlooked in the management of patients with cirrhosis, particularly patients with neurologic impairment (i.e. presence or history of HE).
Management of sleep-related issues
Patients with cirrhosis may experience sleep disturbances that can negatively impact cognitive function. In a study that compared patients with cirrhosis with a chronic disease control group (i.e. patients with inflammatory bowel disease), patients with cirrhosis had poorer sleep quality based on the results of the Pittsburgh Sleep Quality Index (PSQI; global, p = 0.002; PSQI components: sleep disturbance, p = 0.03; daytime dysfunction, p = 0.02; habitual sleep efficiency, p = 0.001; sleep latency, p = 0.03) and, not surprisingly, experienced worsening cognitive impairment. 36 For obese patients (body mass index >30 kg/m2) with cirrhosis, obstructive sleep apnea may be a potential cause of daytime sleepiness, rather than the disruption of sleep–wake cycles known to occur in patients with overt HE. 37 Thus, health care providers should assess potential sleep disorders in patients with cirrhosis, particularly patients who do not adequately respond to overt HE treatment. 37 Diagnosis and management of sleep-related issues in patients with cirrhosis may improve both overall sleep quality and cognitive outcomes; thus, a sleep medicine consult may be considered. Caution should be exercised when considering prescription sedatives for patients with cirrhosis, as sedatives can precipitate HE. Furthermore, sedatives should be prescribed in low doses due to pharmacokinetic changes observed in patients with cirrhosis. For patients with cirrhosis and insomnia, hydroxyzine can be efficacious; for depression, trazodone may be considered.
Hyponatremia
Hyponatremia, which is common in patients with cirrhosis, has been associated with poor outcomes (i.e. hospitalization, mortality).38–40 Indeed, hyponatremia significantly increased the risk of mortality 7.8-fold (serum sodium <126 mEq/L) and 6.3-fold (serum sodium <131 mEq/L) in patients with cirrhosis on a waiting list for liver transplant. 40 Furthermore, the presence of hyponatremia in patients with cirrhosis negatively affected cognition, independent of HE. 41 Correcting hyponatremia (i.e. with tolvaptan) has been reported to improve cognition in patients with cirrhosis. 42 However, due to the risk of serious liver injury, tolvaptan has a black box warning in its label and is only available through a Risk Evaluation and Mitigation Strategy. Given that hyponatremia is associated with poor outcomes in patients with cirrhosis, providers should consider monitoring sodium levels routinely in this patient population.
Cerebral edema
Low-grade cerebral edema, detected using magnetic resonance spectroscopy, may develop in patients with cirrhosis and HE, and has been hypothesized to affect function in patients with HE. 43 Ammonia detoxification occurs in astrocytes, with the conversion of ammonia to glutamine. 44 However, the conversion of glutamine to glutamate by glutaminase can result in high levels of ammonia in the mitochondria of astrocytes, potentially leading to cerebral edema in patients with HE.44,45 In fact, low-grade cerebral edema in patients with cirrhosis has been associated with increased levels of brain glutamine. 46 However, cerebral edema was reversed after treatment (e.g. tolvaptan, lactulose and rifaximin, mannitol, hypertonic saline) or transplantation.42,46–49 Short-term induction of high sodium levels can be very useful in patients with hyponatremia, but sodium correction needs to be closely monitored. Rapid correction of hyponatremia (i.e. >10 mmol/L within 24 h) has been associated with central pontine myelinolysis. 50
Conclusion
Patients with cirrhosis experience complications, including the common neurologic complication of overt HE, which marks the transition from the compensated to the decompensated phase of the disease. Overt HE has features that might overlap with other neurologic complications observed in patients with cirrhosis. International guidelines recommend that health care providers who treat patients with HE consider other potential causes of neurologic dysfunction, identify and manage the precipitating factors for HE, and initiate a treatment regimen to reduce the risk of overt HE recurrence (e.g. lactulose alone or with concomitant rifaximin). In a number of studies, rifaximin alone or with concomitant lactulose reduced the risk of overt HE recurrence, HE-related hospitalizations, and development of other complications (e.g. SBP, variceal bleeding). Because nonadherence to lactulose is associated with a risk of recurrence of HE, patients should routinely be evaluated to determine their adherence to prescribed therapies. Cognitive impairment in patients with cirrhosis may impact patients’ health (e.g. risk for falls), but other neurologic-related issues can also impact cognitive function and quality of life (e.g. sleep-related issues, hyponatremia). Neurologic complications of cirrhosis can have a profoundly negative impact on patients, and ongoing evaluation and maintenance of ideal cognitive function is an important component in overall management strategies.
Footnotes
Acknowledgements
Technical editorial assistance was provided, under the direction of the authors, by Mary Beth Moncrief, PhD, and Sophie Bolick, PhD, Synchrony Medical Communications, LLC, West Chester, PA, USA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for technical editorial assistance was provided by Salix Pharmaceuticals, Bridgewater, NJ, USA.