
Abstract
Behçet’s disease, also known as the oral–ocular–genital syndrome, is a chronic systemic vasculitis characterized by recurrent oral and genital ulcers as well as ocular manifestations such as uveitis and conjunctivitis. When the cardiovascular system is predominantly affected, the condition is known as cardiac Behçet’s disease. This variant can manifest as aortic valve regurgitation, conduction system disorders, myocarditis, and even acute myocardial infarction. Aortic regurgitation is an exceedingly rare and threatening cardiovascular complication in patients with Behçet’s disease, often indicating a poor prognosis. Surgical intervention for aortic regurgitation in patients with Behçet’s disease is associated with high risks of postoperative complications and mortality. To mitigate these risks, techniques such as the Bentall procedure have been employed. This report describes the case of a patient with Behçet’s disease and severe aortic regurgitation who underwent the Bentall procedure. Unfortunately, the patient developed a pseudoaneurysm and prosthetic valve detachment at the aortic root 3 months postoperatively. This severe complication necessitated a subsequent intervention utilizing the Cabrol technique for correction.
Keywords
Introduction
Behçet’s disease (BD), a systemic vasculitis, is characterized by recurrent oral and genital ulcers, skin lesions, and uveitis. This condition can impact multiple organs, such as the eyes, skin, joints, gastrointestinal tract, and central nervous system. The exact cause of BD remains unknown, but it is believed to stem from an abnormal immune reaction prompted by an environmental factor in individuals with a genetic predisposition. The genetic link of BD is evident in its higher occurrence in families with a history of the disease and in individuals with the HLA-B51 allele, a genetic marker associated with BD. 1 Both innate and adaptive immune responses play a role in the immunological abnormalities central to BD pathogenesis. Research has shown that innate immune cells such as neutrophils and monocytes are more readily activated and produce greater amounts of proinflammatory cytokines such as interleukin (IL)-1β, IL-6, and tumor necrosis factor-α. These cytokines contribute to the chronic inflammatory state observed in BD. 2 BD presents a wide array of systemic manifestations, including arthritis, gastrointestinal lesions, and neurological and cardiovascular complications, often resulting in a poor prognosis. 3 Notably, cardiac involvement is considered one of the most severe complications in patients with BD, highlighting the complexity and critical nature of this disease. 4 Cardiovascular disorders are observed in approximately 30% of patients with BD. Histopathologically, the vasculitis in BD is characterized by neutrophil granulocyte infiltration and activation of endothelial cells. Cardiac involvement in BD includes various conditions, such as valvular diseases, pericarditis, myocarditis, and endocarditis. Notably, aortic regurgitation (AR), a manifestation of cardiac or large vessel involvement, occurs in approximately 2% of patients with BD. 5 The exact mechanism by which BD is associated with AR remains unclear, but it is hypothesized to be related to vasculitis, aortic valve prolapses, and perforation. 6 The most effective treatment approach is aortic valve replacement (AVR), supplemented with a range of immunomodulatory medications and hormone therapy. However, conventional AVR in patients with BD is often complicated by a high risk of prosthetic valve detachment (PVD), because residual inflammation makes the aortic root tissue fragile. Consequently, 40%–78% of patients with BD who undergo simple AVR frequently require secondary or even tertiary surgical interventions. 7
Various surgical methods have been employed to enhance the surgical outcomes for patients with BD who suffer from AR. The modified Bentall procedure has been utilized, which involves attaching the valved conduit to the more durable left ventricular outflow tract instead of the delicate annulus, with the goal of reducing the risk of PVD.7,8 Additionally, a novel technique has been implemented that involves wrapping the aortic root with Teflon felt to strengthen the anastomosis and prevent potential tearing. Nonetheless, a conclusive surgical approach for managing AR in patients with BD has not yet been determined.
Case report
In July 2023, a 32-year-old man was admitted to the West China Hospital of Sichuan University due to shortness of breath and chest distress that had persisted for 3 months. His symptoms worsened with physical activity, and he presented with chest pain and occasional orthopnea at night, without cough or fever. He reported a history of recurrent oral and external genital ulcers since June 2020, which had not been further diagnosed or treated. On physical examination, a 3/6 grade heart murmur was detected at the Erb’s point. His blood pressure level was 130/51 mmHg, and his heart rate was 102 beats per minute. Chest X-ray revealed an enlarged heart. Laboratory tests showed a white blood cell count of 4900/mL, C-reactive protein level of 0.12 mg/dL, and procalcitonin level of 0.03 mg/dL. The brain natriuretic peptide level was mildly elevated at 298 pg/mL. Transthoracic echocardiography showed severe AR with two distinct jets, suggesting a prolapse of the left coronary cusp. The ascending aorta had a diameter of 55 mm, and the aortic sinus diameter was 45 mm. Based on the diagnosis, the Bentall procedure was planned for the patient on 20 July 2023. Following a median sternotomy approach, cardiopulmonary bypass was established through cannulation of the aorta and right atrium. Upon aortotomy, significant thickening of the aortic wall was observed, with normal origins of the left and right coronary arteries. The aortic sinus was markedly dilated, and the aortic valve showed severe thickening and insufficiency. A 25-mm Medtronic ATS mechanical aortic valve and a 30-mm prosthetic graft were sutured at the aortic valve annulus and secured at the aortic root. After reimplanting the left and right coronary arteries in situ, the prosthetic graft was anastomosed with the distal aorta. The patient’s postoperative recovery was uneventful. Postoperative echocardiography indicated normal left ventricular function with an ejection fraction (EF) of 52%, and the prosthetic valve functioned normally.
In February 2024, 8 months after the surgery, the patient presented again with activity-induced chest pain and fatigue. Transesophageal echocardiography revealed severe AR, prosthetic aortic valve frame detachment (Figure 1(a) and (b)), and the formation of a pseudoaneurysm at the aortic root. Additionally, there was significant enlargement of the left ventricle (75 mm) and a marked reduction in the EF (32%). Computed tomography angiography demonstrated contained rupture of the ascending aorta, accompanied with the formation of a pseudoaneurysm. Furthermore, the coronary arterial system was adequately perfused (Figure 2(a) and (b)). Emergency surgery was planned for the patient, and a median sternotomy approach was employed after femorocaval bypass. Myocardial protection during the procedure was achieved through the administration of cold antegrade blood cardioplegia via the coronary ostium. After the excision of the aortic valve and ascending aorta, the coronary ostia were meticulously fashioned into buttons from the native aortic root. Significant displacement and distortion of the coronary ostia anatomy were observed. Consequently, 8-mm Dacron grafts were attached end-to-end to each ostium, in preparation for a modified Cabrol technique, which was performed subsequent to the root replacement. In this procedure, the aortic graft attaches to the coronary ostia with a separate Dacron graft to prevent pseudoaneurysms due to excessive tension on the anastomosis. The distal portion of the valved conduit was anastomosed to the proximal arch, which was performed under selective antegrade cerebral perfusion. Close postoperative monitoring and multidisciplinary management were adopted after surgery. The doctors prescribed the patient prednisolone acetate tablets (15 mg once daily); thalidomide tablets (50 mg once at night); tacrolimus capsules (1 mg twice daily); calcitriol capsules (0.5 G once daily); and calcium carbonate tablets (200 mg once at night). After this treatment, his symptoms were relieved. The patient experienced an uneventful recovery without complications and was discharged home after a 14-day hospital stay. The reporting of this study conforms to the Case Report (CARE) guidelines. 9 All patient details have been de-identified from this case report, and written informed consent to treatment was obtained from the patient.
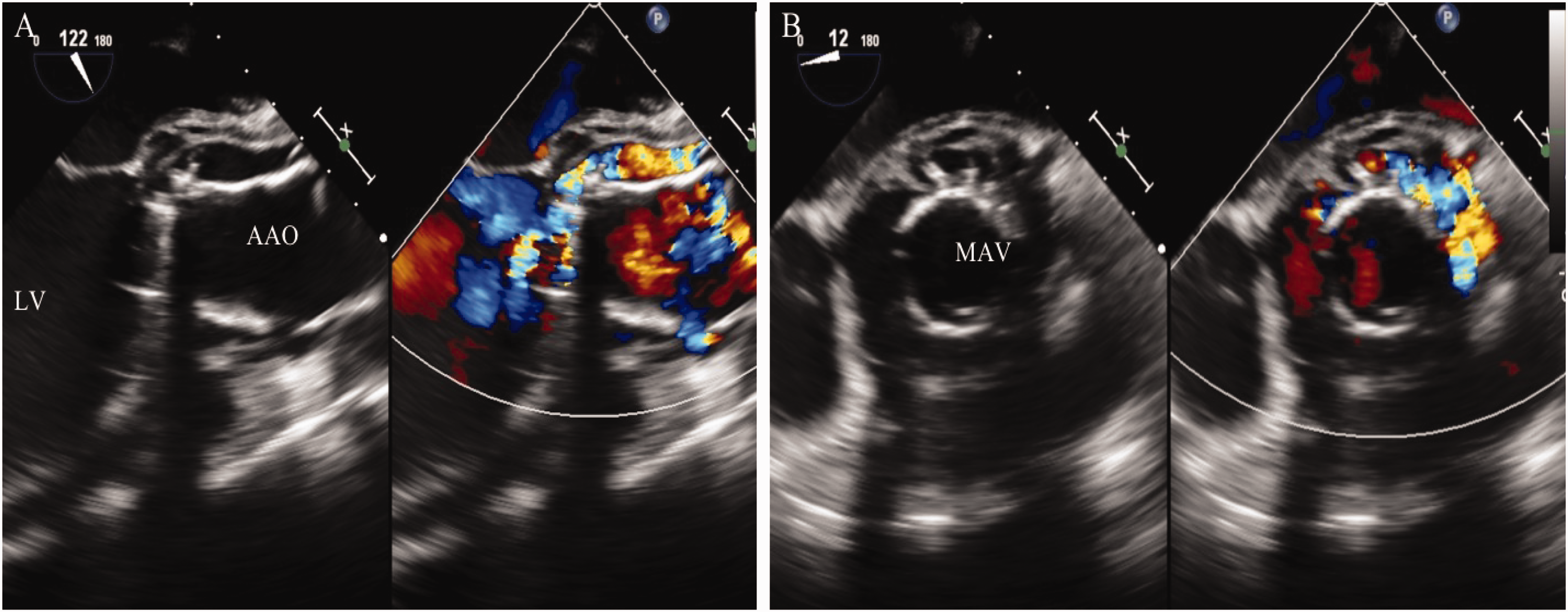
Transesophageal echocardiography. (a) 122 degree of mid-esophageal image and (b) 12 degree of mid-esophageal image showing severe aortic regurgitation and prosthetic aortic valve frame detachment.

CTA. (a) CT and (b) 3D reconstruction of chest CTA demonstrating contained prosthetic valve detachment and pseudoaneurysm formation. CT: computed tomography; 3D: three dimensional; CTA: computed tomography angiography.
Discussion
Cardiovascular issues affect approximately 30% of patients with BD. Although AR is less frequently observed, its consequences can be life-threatening. The success rate of standard AVR in patients with BD is typically low, and there is ongoing debate about the use of alternative surgical techniques. In particular, pseudoaneurysm formation has been documented in 40%–78% of BD cases, underscoring the challenging nature of surgical management in BD.5,10 In addition to intensive immunosuppression therapy, including the use of oral steroids, recent studies have emphasized various technical adjustments during the initial valve implantation to prevent subsequent dehiscence of the valve prosthesis. 11 Consequently, for patients with BD and aortic valve lesions, aortic root replacement surgery is often preferred over traditional AVR. Aortic root reconstruction is effective in preventing PVD and the development of pseudoaneurysms. In cases where AVR has been unsuccessful, the removal of the damaged and weakened annulus, followed by direct placement of the suture line onto the left ventricular outflow tract, may also be beneficial in carefully selected cases. 12 It is essential to acknowledge that BD is a chronic, multisystemic inflammatory disorder of unknown cause. The administration of glucocorticoids and a range of immunosuppressive medications has been shown to be crucial in managing inflammation and enhancing surgical outcomes in patients with BD and aortic root disease. When BD is definitively diagnosed during the initial surgery, isolated AVR should be avoided. Even when patients with BD undergo the Bentall procedure for aortic valve disease, there is still a risk of PVD and pseudoaneurysm formation. Therefore, vigilant postoperative monitoring is essential for these patients.
Conclusion
This report delineates the case of a patient with BD who presented with a contained pseudoaneurysm and PVD at the aortic root. The patient was successfully treated with the Cabrol technique coupled with meticulous postoperative care. It is imperative to note that future studies are essential to assess the long-term outcomes associated with this surgical strategy in BD cases. This report underscores the complexity of surgical management in patients with BD, particularly with regard to aortic root disease, and highlights the need for ongoing research to optimize treatment strategies and improve patient outcomes.
Footnotes
Author contributions
DY: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing.
Availability of data and materials
Data will be made available following reasonable request to the corresponding author.
Consent for publication
Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval
The protocol was approved by the West China Hospital, Sichuan University Clinical Research Ethics Committee.
Funding
Not applicable.