
Abstract
Objective
This observational study examined the risk factors associated with recurrence in patients with mild ischemic stroke and determined the characteristics of high-risk groups.
Methods
A total of 656 patients hospitalized for mild ischemic stroke were monitored for 1 year. Statistical analyses, including odds ratio calculations and K-means clustering, were conducted to examine risk factors for recurrence and the characteristics of high-risk groups.
Results
After 1 year of follow-up, 99 patients experienced recurrent mild ischemic stroke, resulting in a recurrence rate of 15.09%. The analysis revealed several significant risk factors, including type 2 diabetes mellitus, atrial fibrillation, smoking and alcohol consumption, carotid artery stenosis, cerebral vascular stenosis, and multiple lesions. Propensity score matching confirmed these associations, and K-means clustering revealed that older males with type 2 diabetes mellitus and hypertension were likely to be in the high-risk group.
Conclusions
Healthcare professionals should focus on tailored treatment and prevention strategies for high-risk patients, prioritizing the management of the abovementioned risk factors to reduce recurrence and improve outcomes.
Introduction
From 1990 to 2019, there has been a notable surge in the age-standardized prevalence rate of stroke by 33.5%, with the age-standardized incidence rate of ischemic stroke in China showing a corresponding increase of 34.7%. 1 The escalating trend in stroke incidence persists to date, with China exhibiting the highest rates globally, impacting both the nation’s healthcare infrastructure and medical services. 2 As China’s population ages, projections indicate a significant increase in stroke-related metrics by 2050 compared with 2019, with estimated increases of 55.58% in incidence, 119.16% in prevalence, 72.15% in deaths, and 20.04% in disability-adjusted life years. 3 These alarming statistical data underscore the substantial burden on healthcare systems.
Mild ischemic stroke, characterized by mild or rapidly improving symptoms that do not meet major stroke criteria, arises from localized cerebral or retinal ischemia, with clinical manifestations lasting <24 h and typically lacking evidence of structural lesions.4,5 Despite mild clinical symptoms or the absence of apparent neurological deficits, 6 neglecting or failing to address associated risk factors can lead to recurrent strokes. Importantly, individuals experiencing mild ischemic strokes often underestimate the need for interventions, which increases the degree of complexity in managing their risk factors. This oversight can have severe consequences, heightening the risk of subsequent major strokes and dementia,7,8 potentially resulting in disability or death. 9 Recurrent mild ischemic episodes can progressively impair neurological function, leading to symptoms such as paralysis, sensory disturbances, visual impairments, aphasia, and dysphagia, ultimately culminating in partial or complete reliance on caregivers. 10 Studies have reported that the average annual recurrence rate of mild ischemic stroke is 36%–52%.11,12 The recurrence of mild ischemic stroke profoundly impacts both patients and their caregivers, drastically compromising their quality of life. Furthermore, the recurrence of mild ischemic stroke episodes among patients places a substantial burden on the society, necessitating additional healthcare resources, increasing economic and healthcare costs, and increasing the burden on healthcare systems.
Numerous studies have emphasized the strong link between disease factors and minor ischemic stroke incidence.13–15 Hypertension is considered a significant risk factor, with effective treatment showing promise in reducing risk.16,17 Hyperlipidemia is another notable contributor, with elevated cholesterol and triglyceride levels promoting vascular sclerosis and plaque formation and increasing the risk of mild ischemic stroke. 16 Controlling blood lipid levels has been shown to be effective in mitigating this risk. 18 Additionally, type 2 diabetes mellitus, smoking, and a sedentary lifestyle have been associated with an increased risk of mild ischemic stroke.19–23 Promoting stringent control of these risk factors is paramount in reducing the incidence of mild ischemic stroke. Although previous studies have examined factors influencing recurrent events in patients with mild ischemic stroke, 24 further research is needed to delineate modifiable risk factors and better characterize high-risk subpopulations. A comprehensive understanding of these factors is crucial for developing targeted prevention strategies and personalized therapeutic interventions. Therefore, this study aimed to identify the risk factors associated with recurrence in patients with mild ischemic stroke in China and characterize the demographic profiles of high-risk patients. The findings are expected to enhance the identification of high-risk populations and inform effective preventive measures.
Methods
Participants
Participants for this study included patients diagnosed with mild ischemic stroke at the First Affiliated Hospital of Xiamen University in China between January 2018 and June 2020. The research team executed a meticulous 1-year follow-up to monitor symptom recurrence. Follow-up interactions occurred through regular hospital visits and telephone inquiries.
This study explicitly defined the inception cohort based on several criteria. First, the inclusion criteria were as follows: (a) hospitalized within 7 days of the first stroke onset, with mild ischemic stroke confirmed by head computed tomography and magnetic resonance imaging (MRI); (b) National Institutes of Health Stroke Scale (NIHSS) score ≤3; (c) voluntary participation with consent for follow-up; and (d) no cancer diagnosis. Second, time zero evaluation was performed, wherein the follow-up period began on the day of discharge. Third, the exclusion criteria were as follows: (a) history of stroke or transient ischemic attack; (b) presence of malignant tumors or end-stage renal disease; and (c) death due to nonischemic cerebrovascular disease, loss to follow-up for other reasons, or withdrawal from participation before the occurrence of an endpoint event or the end of the follow-up period. Finally, 656 participants met the inclusion criteria and underwent further analysis.
All participants received standard treatment for mild ischemic stroke, including antiplatelet therapy, anticoagulation, statins for lipid and plaque stabilization, and antihypertensive and hypoglycemic treatment. Blood samples were collected within 48 h of admission at one time point, and blood biomarkers (e.g. C-reactive protein, interleukin-6, and tumor necrosis factor-α) were not tracked during follow-up. No fatalities occurred during the follow-up period. The Biomedical Ethics Review Committee of The First Affiliated Hospital of Xiamen University approved this study (approval #03/2023, No: XMYY-2023KY032-01). Written informed consent was obtained from all patients prior to their participation in the study, and patient details were deidentified during data analysis. This study was conducted in accordance with the principles of the Declaration of Helsinki. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 25
Data collection
This study meticulously extracted research data from electronic medical records, clinical records, and imaging data acquired during patients’ hospitalization. This comprehensive dataset included crucial information regarding patients and their conditions, including age, sex, hypertension, type 2 diabetes mellitus, hyperlipidemia, hyperuricemia, atrial fibrillation, carotid artery stenosis, cerebral vascular stenosis, smoking, alcohol consumption, and NIHSS score. Carotid artery stenosis was confirmed using diagnostic techniques such as carotid vascular ultrasound color Doppler, carotid computed tomography angiography (CTA), contrast-enhanced magnetic resonance angiography, and carotid digital subtraction angiography (DSA). Additionally, cerebral stenosis was confirmed via head CTA, head magnetic resonance angiography, and head DSA. Hypertension refers to a patient’s systolic blood pressure measurement of ≥140 mmHg and/or diastolic blood pressure measurement of ≥90 mmHg on three different days. Hyperlipidemia refers to a state in which the patient’s total cholesterol, low-density lipoprotein, and triglyceride levels are higher than the normal range, especially low-density lipoprotein level of ≥4.1 mmol/L, which is tested by collecting 2–3 mL of venous blood on an empty stomach and using the Beckman Coulter fully automatic biochemical analyzer (AU-5831). Smoking and drinking history referred to the patient’s current history of smoking and alcohol consumption. Atrial fibrillation refers to a patient’s diagnosis of paroxysmal, persistent, or permanent atrial fibrillation through routine electrocardiogram, dynamic electrocardiogram, and 7-day long-term electrocardiogram examinations.
The diagnostic criteria for mild ischemic stroke rely on evaluations through head CTA, MRI, and NIHSS score. The NIHSS score serves as a critical tool for gauging the severity of neurological deficits resulting from localized cerebral ischemia. 6 Typically, a score of 3 points or less on the NIHSS is indicative of mild ischemic stroke. This standardized approach ensures a comprehensive assessment, incorporating advanced imaging techniques and a nuanced scoring system to accurately diagnose the severity of the ischemic event.
Statistical analysis
The SPSS 26.0, G-Power 3.1, and R 4.3 statistical software were used in this study. SPSS and R were used to perform statistical tests such as the chi-square test, whereas G-Power was employed to calculate the sample size and power of the main outcomes. Descriptive statistics were expressed as case numbers and percentages, and group comparisons were conducted via the chi-square test. Odds ratios (ORs) were calculated to identify risk factors for recurrent stroke. To control for potential biases related to age and sex differences, propensity score matching was applied for secondary validation of the results. Additionally, K-means clustering was used to determine the characteristics of high-risk groups for recurrent stroke. A p value of <0.05 was considered to indicate statistical significance.
Results
Baseline characteristics of the recurrent and nonrecurrent groups
Table 1 presents the analysis of baseline risk factors between the recurrent and nonrecurrent groups within 1 year of mild ischemic stroke. The results indicated that the following factors were likely associated with an increased risk of recurrent mild ischemic stroke within 1 year: type 2 diabetes mellitus (OR = 3.057, 95% confidence interval (CI): 1.976–4.731), atrial fibrillation (OR = 14.008, 95% CI: 7.246–27.081), drinking (OR = 4.790, 95% CI: 3.062–7.492), smoking (OR = 1.778, 95% CI: 1.157–2.734), carotid artery stenosis (OR = 2.725, 95% CI: 1.496–4.964), cerebral vascular stenosis (OR = 5.819, 95% CI: 3.687–9.183), and multiple lesions (OR = 2.078, 95% CI: 1.037–3.304). These findings suggest that patients with these conditions as well as those with smoking and drinking habits should pay closer attention to the risk of recurrent mild ischemic stroke.
Risk factor analysis of baseline characteristics in the recurrent and nonrecurrent groups (N = 656).
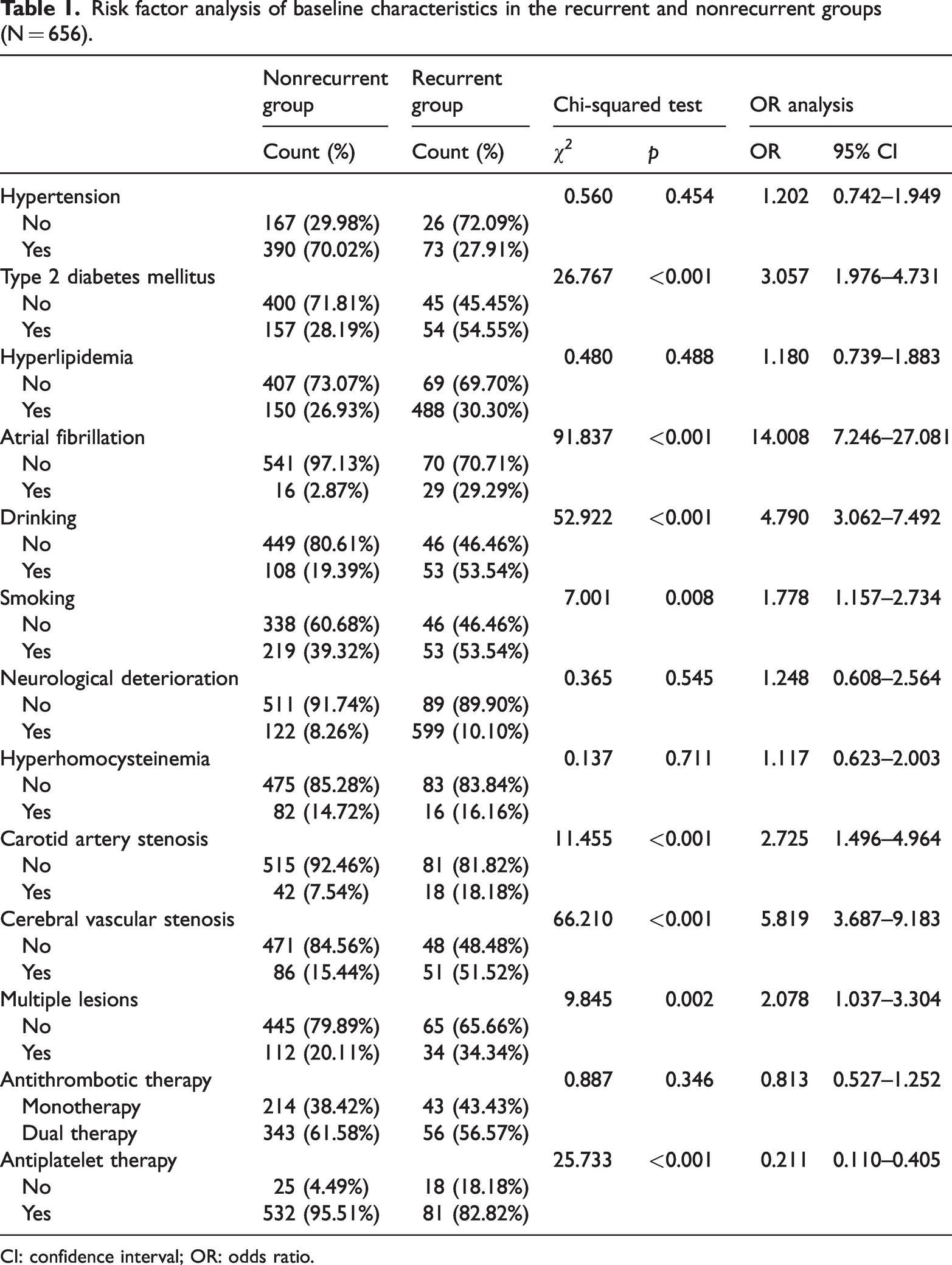
CI: confidence interval; OR: odds ratio.
Analysis of risk factors between the recurrent and nonrecurrent groups after propensity score matching
To control for potential bias caused by differences in sample characteristics, propensity score matching was used to match the samples on the basis of age and sex, resulting in a matched sample of 184 cases. The results, as shown in Table 2, indicated that several factors were associated with an increased risk of recurrent stroke within 1 year of an ischemic mini-stroke. These factors include type 2 diabetes mellitus (OR = 3.300, 95% CI: 1.788–6.092), atrial fibrillation (OR = 13.656, 95% CI: 3.985–46.800), drinking (OR = 5.735, 95% CI: 2.939–11.193), smoking (OR = 1.856, 95% CI: 1.032–3.339), carotid artery stenosis (OR = 3.486, 95% CI: 1.315–9.241), cerebral vascular stenosis (OR = 7.273, 95% CI: 3.499–15.118), and multiple lesions (OR = 2.110, 95% CI: 1.100–4.049). The results indicated that even after propensity score matching, the abovementioned factors were associated with the recurrence of mild ischemic stroke. This further underscores the need for targeted interventions to mitigate the risk of recurrence.
Association of recurrent mild ischemic stroke with risk factors after propensity score matching (n = 184).
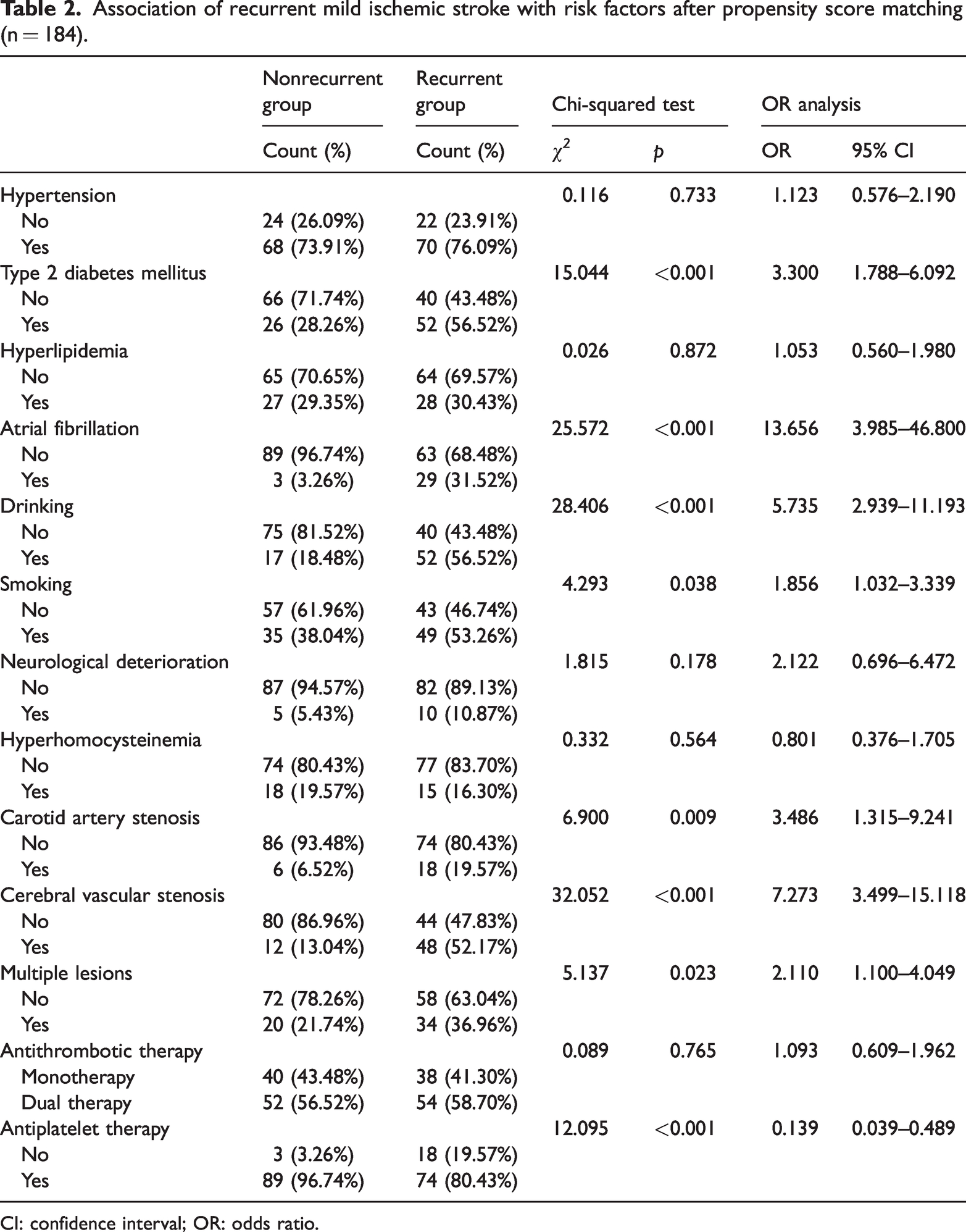
CI: confidence interval; OR: odds ratio.
K-means clustering analysis of different recurrence risk groups
Figure 1 illustrates the optimal number of clusters based on the elbow method. The x-axis represented the number of clusters, which corresponded to the range of K values in the K-means method. The y-axis represented the total within-cluster sum of squares, which refers to the sum of the squared distances from each sample point to its respective cluster center. A smaller total within-cluster sum of squares indicated that the data points within a cluster were more tightly grouped. Figure 1 shows that when K = 1, the total within-cluster sum of squares was at its maximum. As K increased, the total within-cluster sum of squares decreased rapidly. However, at approximately K = 3, the rate of decline slowed down, and further increasing K had a diminishing effect on reducing the total within-cluster sum of squares. Therefore, dividing the samples into three clusters appears to be the most reasonable approach. This grouping effectively captures differences in recurrence risk among different groups.

Number of K clusters.
Table 3 presents the results of the K-means clustering analysis for different recurrence risk groups. The findings revealed that in the high-risk group, the average age was 72.02 ± 4.26 years. In this group, 59% of the patients were male, 80% had hypertension, and 36% had type 2 diabetes mellitus. These results suggest that individuals at high risk of stroke recurrence are likely generally characterized by older age, male sex, type 2 diabetes mellitus, and hypertension. This highlights the importance of considering these factors in targeted interventions for stroke prevention.
Characteristic description of different recurrence risk groups (N = 656).

M: mean; SD: standard deviation.
Discussion
Our findings revealed that type 2 diabetes mellitus, atrial fibrillation, carotid stenosis, drinking, smoking, carotid artery stenosis, multiple lesions, and cerebral artery stenosis may be predictors of recurrence within 1 year. First, previous studies have identified these factors as significant risk factors for stroke recurrence.10,26–28 However, our study specifically focused on the recurrence risk of mild ischemic stroke, distinguishing it from previous studies that did not fully address this subtype. Our findings indicate that these factors are not only critical for stroke risk but also play crucial roles in the recurrence risk of mild ischemic stroke. Second, atrial fibrillation, a common cardiac arrhythmia, can lead to the formation of blood clot in the heart, 28 increasing the recurrence risk of mild ischemic stroke if clots travel to cerebral blood vessels. Additionally, atrial fibrillation tends to cause a decrease in blood flow velocity in the left atrium and left atrial appendage, leading to the formation of blood clots. When these clots dislodge, they can enter cerebral arteries and cause cerebral embolism, thereby increasing the risk of stroke recurrence. 29 Carotid artery stenosis and cerebral artery stenosis, often caused by arteriosclerosis, narrow blood vessels, restrict blood flow, and increase the likelihood of thrombosis and stroke. 30 Regarding smoking and alcohol consumption, the physiopathological interactions between nicotine, carbon monoxide, ethanol metabolites, and cerebrovascular homeostasis collectively affect the vascular system and blood components, thereby increasing the risk of recurrence. Given the association between these factors and the increased risk of mild ischemic stroke recurrence, appropriate interventions, such as anticoagulants to prevent thrombosis and carotid endarterectomy, should be implemented.31,32 Hyperlipidemia increases blood viscosity, slows blood flow, and causes lipid deposition, which can narrow the arteries and, in severe cases, obstruct blood flow. 33 It also contributes to atherosclerosis via cholesterol buildup.34,35 Therefore, it is important to avoid high-fat and high-cholesterol foods and maintain a low-salt, low-fat diet. Additionally, adopting a healthy lifestyle, including quitting smoking and alcohol consumption, undergoing regular medical check-ups, and engaging in physical exercise, is essential.16,36
Our results suggest that individuals at high risk of mild ischemic stroke recurrence are likely generally characterized by older age, male sex, type 2 diabetes mellitus, and hypertension. Although previous studies have also identified these factors as major contributors to increased stroke risk,10,16,17 they have typically examined them separately from a single perspective. Researchers have not considered these risk factors collectively to identify the characteristic profiles of high-risk populations. Determining the group characteristics of high-risk individuals is crucial for effective prevention in both clinical practice and public health. The underlying causes of this outcome are likely the result of the combined effects of physiological, hormonal, and metabolic factors. Aging leads to vascular degeneration, increased arterial stiffness, and a greater likelihood of atherosclerosis, all of which contribute to impaired cerebral blood flow and an elevated risk of stroke recurrence. Owing to differences in sex hormones, males generally have a higher risk of stroke recurrence than females, as estrogen provides a protective effect in premenopausal women by promoting vasodilation and reducing inflammation. 37 Type 2 diabetes mellitus exacerbates vascular damage by accelerating atherosclerosis, promoting endothelial dysfunction, and increasing blood viscosity, collectively increasing the risk of recurrent ischemic events. 38 Similarly, hypertension, a major modifiable risk factor, causes chronic damage to arterial walls, increases the likelihood of plaque rupture, and leads to microvascular changes in the brain, further predisposing individuals to stroke recurrence. The interplay of these factors creates a cumulative risk, increasing the susceptibility of older adults, particularly men with type 2 diabetes mellitus and hypertension, to recurrent strokes. For older individuals, males, and those with type 2 diabetes mellitus or hypertension who have a higher risk of stroke recurrence, a comprehensive approach to achieve prevention and intervention should be adopted. This includes health education, individualized pharmacological treatment, lifestyle modifications, and a multidisciplinary management model to effectively reduce the risk of recurrence and improve patients’ quality of life.
Limitations
Although this study offers valuable insights, it is imperative to acknowledge certain limitations. First, the study’s sample size, although contributing meaningful data, remains relatively small compared with other studies, potentially constraining the generalizability of our findings to broader populations or diverse contexts. Addressing this limitation in future research could involve employing larger and more diverse samples, coupled with more comprehensive measures of the variables under investigation. Second, the follow-up period in this study spanned only 1 year, limiting the scope of observation. Prolonging the follow-up duration in future investigations may unveil novel insights into the risk factors associated with mild ischemic stroke recurrence. Finally, the identified risk factors in this study remain relatively limited, and future research should explore additional influencing factors. For example, the data records related to medication adherence in this study (such as statin therapy and anticoagulation therapy) were still incomplete, and these data were not fully incorporated into the data analysis. Given the correlation between medication adherence and the recurrence of mild ischemic stroke, further exploration of the correlation between medication adherence and stroke recurrence is needed in the future.
Conclusions
This study highlights that patients with type 2 diabetes mellitus, atrial fibrillation, carotid stenosis, smoking and alcohol consumption, multiple lesions, and cerebral artery stenosis are likely susceptible to recurrent mild ischemic strokes. Moreover, individuals at high risk of recurrence are likely to be characterized by older age, male sex, type 2 diabetes mellitus, and hypertension. Therefore, timely and effective interventions, including targeted secondary prevention strategies, are essential for reducing recurrence rates and alleviating the associated socioeconomic burden.
Footnotes
Acknowledgments
We are grateful to the First Affiliated Hospital of Xiamen University for facilitating data collection. We would like to thank the patients for participating in the study.
Author contributions
Conceptualization, Shangmeng Huang; Data curation, Shangmeng Huang, Wenbin Lan, Junqing Huang, and Huijuan Wan; Funding acquisition, Jin Han Chen; Project administration, Jin Han Chen; Resources, Wenbin Lan, Junqing Huang, and Huijuan Wan; Supervision, Dewen Wang and Jin Han Chen; Visualization, Dewen Wang; Writing—original draft, Shangmeng Huang and Zhengyu Wu; Writing—review & editing, Zhengyu Wu.
Data availability statement
The study includes no data from unpublished restricted (nonpublicly available) human clinical databases. The data supporting this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that they have no conflicts of interest.
Funding
This research was funded by the Translational Medicine Foundation of Xiamen University (no. XFY2020003) and the National Natural Science Foundation of China (no. 72074187).
Institutional review board statement
All methods were conducted in accordance with relevant guidelines and regulations. The Biomedical Ethics Review Committee of The First Affiliated Hospital of Xiamen University approved this study (no: XMYY-2023KY032-01), and all participants signed informed consent. This study was conducted in compliance with the Helsinki guidelines.
Informed consent statement
Not applicable.