
Abstract
Objective
Caries risk assessment tools are essential for identifying and providing treatment for individuals at high risk of developing caries. We aimed to develop a nomogram for the assessment and evaluation of caries risk among Chinese children.
Methods
We enrolled schoolchildren age 7 years from a primary school in Shanghai. Baseline information of participants was collected using a questionnaire completed by children’s caregivers. A nomogram of a novel prediction scoring model was established based on predictors detected in univariate and multivariate analyses. Predictive accuracy and discriminative ability of the nomogram were calculated using the concordance index (C index). The bootstrap method (1000 samples) was used to decrease overfitting. The net benefit of the model was validated using decision curve analysis.
Results
Overall, 406 children with complete information and two completed dental examinations were included in the final analysis. The nomogram based on logistic regression model coefficients demonstrated a C index of 0.766 (95% confidence interval: 0.761–0.771) for caries risk. The net benefit of the decision curve analysis was 38.6% at 55% threshold probability.
Conclusion
This nomogram model, derived using dietary habits, oral hygiene status, and caries experience, showed promising predictive ability to assess the caries risk among Chinese children.
Introduction
Dental caries refers to chronic and progressive destruction of dental hard tissue under the action of various factors, mainly bacteria. Caries may cause pulpitis and periapical inflammation and can produce severe pain and swelling of the jaw. If not treated in time, caries can eventually lead to missing teeth and a heavy financial burden to patients.1–3
The Fourth Chinese National Oral Health Survey showed that the prevalence of permanent tooth caries among children aged 12 years was 34.5%, an increase of 7.8% from 10 years earlier. The prevalence rate of deciduous teeth caries among 5-year-old children was 70.9%, an increase of 5.8% from 10 years earlier.4–7 These results demonstrated that with economic development in China, the incidence of dental caries has increased, in comparison with other countries in which this incidence has decreased.2,8,9 To effectively prevent children's caries and reduce the incidence of caries in China, comprehensive analysis of the causes as well as children's developmental characteristics, diet, hygiene habits, and other conditions is a first step. Dental caries is a progressive and preventable chronic disease that results from many factors ranging from socioeconomic status, eating habits, and oral hygiene to those related to attitudes about oral health and habits of visiting the dentist. 10 Therefore, screening and identification of individuals with a high risk of dental caries is essential for the early prevention of this disease. 11
Caries risk assessment (CRA) is a process of determining the probability of an individual developing new dental caries over a specified period. 12 CRA programs such as the Caries-risk Assessment Tool (CAT), 13 Caries Management by Risk Assessment (CAMBRA), 14 the Cariogram, 15 and the National University of Singapore Caries Risk Assessment (NUS-CRA) have been established. 16 These are widely used among non-institutionalized populations and in dental clinics for caries management. 17 However, the sensitivity and specificity of these predictive systems vary widely among different studies, from 100% (sensitivity) and 3.6% (specificity) to 86% and 69% for CAT, 16,18 and from 46% and 88% to 71% and 66% for the Cariogram.19,20 Furthermore, most CRA systems have been established and applied in developed countries and are more reliable in populations with a low risk of dental caries. 21 In developing countries that lack CRA programs, children experience much a higher prevalence of dental caries.
The aim of the present study was to identify the indicators associated with dental caries and develop predictive models for the assessment of caries risk based on a prospective cohort study conducted among 7-year-old schoolchildren in Shanghai.
Methods
Ethical issues
The protocol of this study was approved by the Ethics Committee of Shanghai Stomatological Hospital (permit number: 2014-0011). Written informed consent was obtained from the caregivers of each child before their enrollment in the study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 22
Participants and study design
Children aged 7 years were recruited from a primary school in Huangpu District, Shanghai in May 2014. After completing a dental examination and questionnaire (completed by caregivers), the children were included in this cohort study. The inclusion criteria for children in the study were: (1) no use of antibiotics or other drugs that may affect saliva production within the previous 2 weeks; (2) parents or guardians signed the informed consent form. Exclusion criteria were: (1) unable to cooperate with dental examination; (2) parents or guardians unwilling to sign the informed consent form. Two years later (in 2016), participants were examined again to determine their dental health status. All enrolled children who had completed two oral examinations and the questionnaire survey were included in the model. All participant data were de-identified and kept confidential after data collection.
Dental examinations
Dental examinations were performed under artificial lighting by four calibrated dentists in 2014 and 2016. Participants were examined while seated in a portable dental chair with fiber-optic lighting. The entire dentition was checked for caries using a combination of exploration and visual inspection. World Health Organization procedures and diagnostic criteria for dental caries as well as the Chinese Fourth National Oral Health Epidemiological Investigation standard were followed in unified training for the examiners and for standard consistency inspection. 7 The kappa value was required to reach 0.8 before inspection. 23 Tooth status was mainly assessed by visual inspection, aided by tactile inspection if necessary. A Community Periodontal Index probe was used and no radiographs were taken. Decayed, filled, and missing teeth (dmft for deciduous teeth, DMFT for permanent teeth) were recorded, and the caries increment (Δdmft + ΔDMFT >0) was calculated.
Questionnaire survey
A questionnaire to be completed by the children’s caregivers was developed according to the Third National Oral Health Survey of China. 24 Information was collected on socioeconomic status, eating habits, oral hygiene, parental knowledge on and attitudes about oral health, and habits of visiting the dentist.
Statistical analysis
Data were input to Epidata 3.1 (http://www.epidata.dk) and analyzed using IBM SPSS version 21 (IBM Corp., Armonk, NY, USA) and R Version 3.6.2 (The R Project for Statistical Computing, Vienna, Austria). Count variables are described as frequency and percentage and compared using the χ2 test, Fisher’s exact test, or Cochran–Mantel–Haenszel chi-square test. Prediction factors with P < 0.1 in the univariate analysis were included as candidate factors in a stepwise multivariate logistic regression model (LRM). A nomogram was elaborated using LRM coefficients with the RMS package in R. The predictive performance of the nomogram was measured using the concordance index (C index) and calibrated with 1000 bootstrap samples to decrease overfitting. Finally, using decision curve analysis (DCA), we evaluated whether the model improved the predictive net benefit. All tests were two-sided and P<0.05 was set to indicate significance.
Results
The inter-examiner reliability of the four examiners was high, and the kappa for caries examination was 0.90. No significant difference was found between children who were lost to follow-up and those who were followed up, in terms of demographic and socioeconomic profiles and baseline caries status.
Of the 497 children examined at baseline, 406 were re-examined after 2 years and were included in the analysis of this study. At baseline, 69.7% of children were affected by caries. The mean of dmft + DMF was 3.43 with a standard deviation of 3.57. During the following 2 years, 54.4% of children developed new caries (Δdmft +ΔDMFT >0).
We found that approximately 30% of 7-year-old children in this study consumed sweets once a day, and 11.7% of children did so more than twice a day (Table 1). As shown in the table, significant associations were found between the incidence of caries and the following eight factors: intake of cookies and cakes, bedtime sweets, frequency of tooth brushing, age at the start of tooth brushing, toothache or discomfort in the previous 12 months, evaluation of oral health by parents, and dental caries at age 7 years. There were no differences in sex, birth weight, education level of caregivers, family income, and pit and fissure sealing at age 7 years between the two groups (Table 1).
Association of factors with incident dental caries in children age 7 years (N = 406).

a Cochran–Mantel–Haenszel chi-square test.
b Fisher’s exact test.
All eight of the above potential risk factors or indicators with P < 0.1 were candidates for inclusion in the stepwise multivariate LRM. The results showed that among the eight candidates, three factors were independent risk factors for dental caries: dental caries at age 7 years, intake of cookies and cakes, and frequency of tooth brushing (Table 1).
We constructed a diagnostic nomogram to predict the risk of dental caries based on the multivariate LRM; with upper and lower bars. The values on the scale bar (dental caries at age 7 years, intake of cookies and cakes, and frequency of tooth brushing) corresponded to the scores on the points bar. By adding the scores of each factor, the total points for each child were obtained. The calculated “Total points” was then applied to the lower “Risk” bar of the nomogram to evaluate the risk of dental caries in a child aged 7 years (Figure 1).
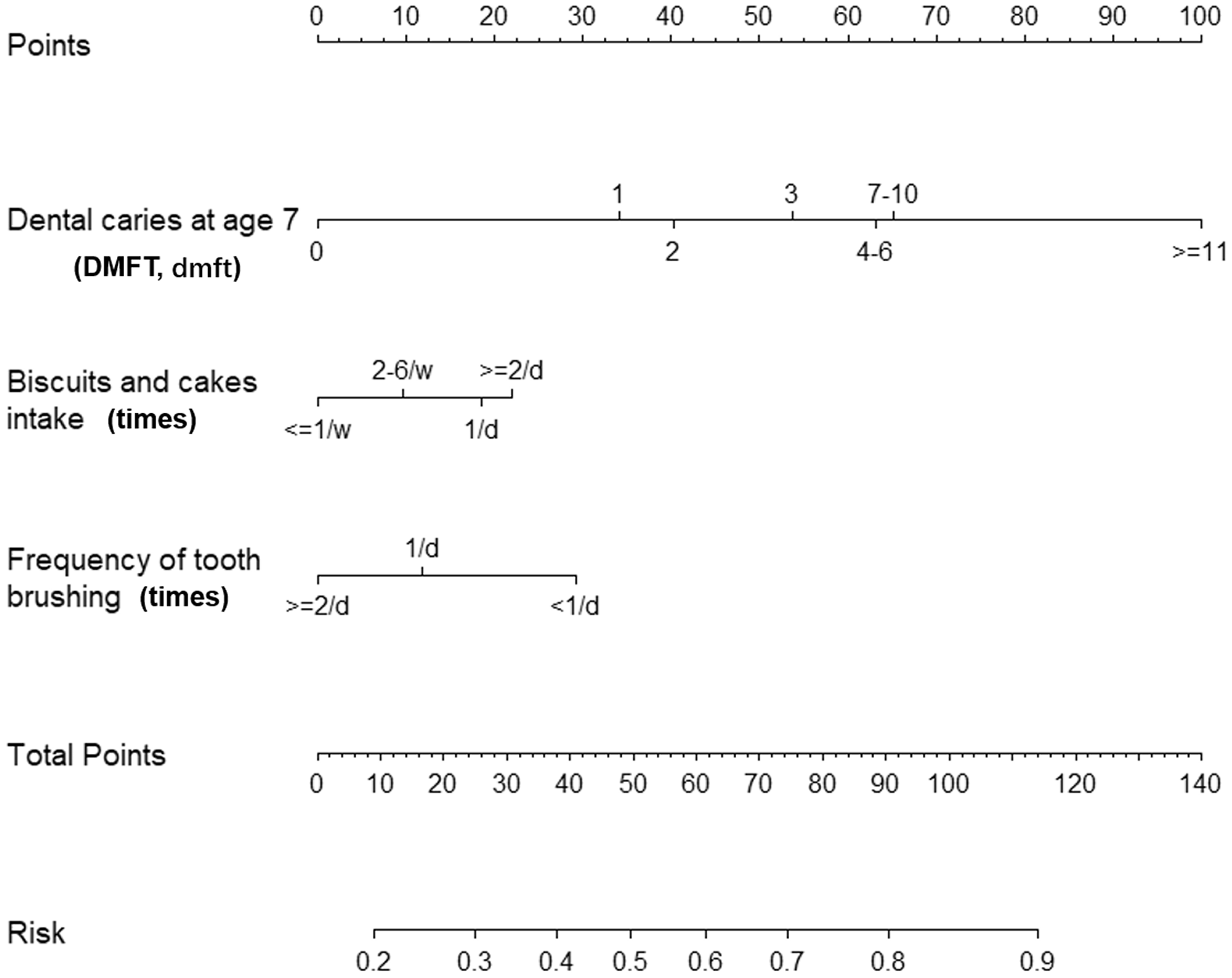
Nomogram to predict the risk of dental caries based on multivariate logistic regression model.
The resulting model was internally assessed using the C index and calibrated with 1000 bootstrap samples (Figure 2). The nomogram demonstrated good accuracy in estimating the risk of dental caries, evidenced by a C index of 0.766 (95% CI: 0.761–0.771; P < 0.001) for dental caries.

Evaluation of nomogram accuracy.
The results of DCA showed a net benefit of 38.6% at a 55% threshold probability, which was superior to the baseline model (Figure 3).

Decision curve analysis for the risk of dental caries based on the nomogram.
Discussion
According to the Fourth National Oral Epidemiological Survey in China, 79.3% of dental caries occurred in 33% of the population. 25 The distribution of caries in the population is not uniform and depends on various factors include diet, genetics, socioeconomic status, and dental care habits. Proper evaluation of the caries risk in children will lead to timely detection, treatment, and a reduced financial burden for both families and society.8,26
Caries risk assessment is a fundamental measure in the screening of people with a high risk of caries to facilitate prevention. 27 There are two main types of CRA, namely, reasoning-based programs (CAT and CAMBRA) and algorithm-driven programs (Cariogram and NUS-CRA). 16 However, no CRA model can accurately predict whether an individual will develop caries at a certain time. Most existing models were developed based on local living habits, diet structure, dental hygiene habits, and fluoride application. 11 As a result, it is difficult to find an appropriate prediction model for use among children in China for caries risk prediction. In this study, we developed a novel caries risk prediction nomogram model based on a prospective cohort study in Shanghai to detect and effectively intervene among children with a high risk of dental caries. Three factors were included in the final model: dental caries at age 7 years, intake of cookies and cakes, and frequency of tooth brushing.
Dental caries is a multifactorial disease and CRA tools usually include multiple risk factors and protective factors in a prediction system. In the current study, children’s dietary habits (e.g., consumption of cookies and cakes) and oral hygiene (e.g., frequency of tooth brushing) were validated as significant predictive factors, which was consistent with many previous investigations.13–16 According to previous studies, a high-sugar diet and snacking can cause plaque formation on the surface of the tooth and reduces pH in the mouth. With inadequate friction from consuming raw, high-fiber foods or incorrect methods of plaque removal, demineralization and cavity formation in the teeth are inevitable.
As the results demonstrated, approximately 30% of 7-year-old children in this study consumed sweets once a day, and 11.7% of children did so more than twice a day (Table 1). Similar observations were made by Zhang et al., who conducted a survey in an different district of Shanghai. 28
Tooth brushing is an important way to inhibit the formation of dental plaque. In this study, we found that the occurrence of dental caries in children aged 7 years was related to the frequency of tooth brushing. Previous studies also show that children with a low frequency of brushing teeth are more likely to develop dental caries.29,30 Additionally, there is a significant relationship between proper tooth brushing technique among children and their parents’ awareness about dental health care.31,32 Therefore, dentists should work together with teachers and parents to develop a plan to educate children in proper tooth brushing, which will have a positive influence on inhibiting the occurrence and development of dental caries among children.
Past caries experience was the strongest indicator of caries risk in both the univariate and multivariate analyses. This factor comprehensively reflects the interaction of the effects of protective factors and risk factors and even the individual’s susceptibility. Our results showed that 71% of children who had dental caries at 7 years of age developed new caries 2 years later (Table 1). These results are consistent with those of several studies, which have demonstrated that children with past caries experience had a significant likelihood of developing new caries in the future, using past caries experience alone or in combination with other factors in caries prediction models. 33 Moreover, investigations also suggested that children with lesions such as a chalky color change, detectable plague on the tooth surface, or undeveloped enamel should also be classified in the high-risk category because these are indicative of present caries.26,29
Our findings revealed that toothache or discomfort in the previous 12 months, bedtime sweets, evaluation of oral health by parents, and filled caries at age 7 years were significant predictors of future caries development, which is consistent with many previous investigations.32,34,35 In our study, all these factors were treated as candidate risk factors or indictors in the stepwise multivariate LRM with backward selection. Despite correlation existing among these factors, ignoring some of them may lead to increased reliability of the prediction model. As for the present study, we chose P < 0.05 as the criterion for variable selection. Although, some other statistical tools, such as ridge regression and principal component analysis, are suggested to resolve this problem, their application in the context of nomograms must be further investigated. 36
Interestingly, previous studies have demonstrated a significant association between socioeconomic disadvantages and the prevalence of dental caries at different ages among children, especially toddlers and kindergarten-aged children. This is because the oral hygiene habits of these children are greatly influenced by parental skills and attitudes toward dental hygiene.34,37,38 However, in the present study, the education level of caregivers and family income were not significantly associated with dental caries in 7-year-old children. Our results are similar to findings from another study conducted among children aged 11 to 14 years 39 and a cross-sectional study on the disparity in caries between migrant and native children in Shanghai. 28 All these studies were performed in Shanghai, which is the most highly developed city in China in terms of economy and public health care and where free dental health checkups and treatment are provided by community dentists in every public school each year. 40 This might partly demonstrate that school-based dental public health services play an important role in ensuring accessibility to these services and reducing disparities in dental health status among children with different socioeconomic levels.28,40,41
In the present study, we developed a nomogram model for caries risk prediction among children living in Shanghai, which integrates multiple prediction indicators and uses the line segment with scale in a certain proportion to express the relationship between each variable in the model. Compared with other CRA models, this model is easy to use and is more applicable in mass screening to identify individuals with a high-risk of dental caries. Internal data were used for verification of this model, and the C index was 0.76, suggesting that this prediction model was in good agreement with the actual observations.
There are several limitations in the present study. First, all participants were recruited from one primary school; therefore, the restricted representativeness of the sample may limit the generalizability of the results to other populations. Second, the follow-up period in the present study was 2 years, which is a time-dependent process. Whether there was any change in dental caries during the 2 years is not only related to the baseline but is also related to the children's dietary habits and oral health. This may be part of the reason why the prediction accuracy in the current model could not be further improved.
Conclusions
In this study, we developed a caries risk prediction nomogram model. Eating patterns, oral hygiene habits, and caries experience were the most important factors to predict the incidence of caries among children living in Shanghai. This model provides a simple and reliable scoring system for caries risk prediction.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This research received financial support from the Research Project of Shanghai Municipal Commission of Health and Family Planning (201740062), Clinical Research Cultivating Project of SHDC (SHDC12017X22).