
Abstract
A 70-year-old man developed intermittent fever with chills, severe anorexia, generalized weakness, and mild exertional difficulty in breathing following posterior chamber intraocular lens replacement surgery for a mature white cataract in the left eye. Laboratory tests revealed persistent negative blood cultures, normocytic and normochromic anemia, neutrophilia, and elevated inflammatory markers despite multiple courses of antibiotics. All other investigations conducted to identify the cause of prolonged fever, including transthoracic echocardiography, were negative. However, transesophageal echocardiography detected an aortic valve vegetation. The patient had no history of valvular disease or any predisposing condition for infective endocarditis. The bacteremia was strongly suspected to have resulted from cataract surgery, although no obvious signs of eye infection were observed during the postoperative period. The patient was treated with empirical antibiotics, including vancomycin and ceftriaxone, which led to significant improvement. Because infective endocarditis remains a significant public health concern with increasing incidence rates, we present this unusual case of culture-negative infective endocarditis following cataract surgery, highlighting the diagnostic and therapeutic challenges encountered.
Keywords
Introduction
Infective endocarditis (IE) occurs worldwide and involves bacterial growth on the endocardial surface of native or prosthetic heart valves, pacemakers, or cardioverter-defibrillators. 1 The majority of IE cases are caused by gram-positive bacteria, including streptococci, staphylococci, and enterococci, with Staphylococcus aureus being the most common pathogen.¹ In addition to various species of streptococci, other oropharyngeal colonizers, such as the HACEK organisms (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, and Kingella), can infrequently cause infections. Additionally, fungi such as Candida and Aspergillus are rare but possible etiological agents. 2 The diagnosis of IE traditionally relies on the Modified Duke Criteria, which include major and minor criteria. A diagnosis is established by meeting either two major criteria, one major and three minor criteria, or five minor criteria. 3 The 2023 European Society of Cardiology (ESC) Guidelines for endocarditis management provide detailed and specific recommendations for antimicrobial therapy tailored to the identified causative pathogens. 4
IE is associated with significant public health concerns. According to 2019 data, IE caused 66,300 deaths globally, with an incidence of 13.8 cases per 100,000 individuals. 5 As diagnostic detection methods improve, the reported incidence is likely to increase. The significant morbidity and mortality rates of 1723.59 disability-adjusted life years and 0.87 deaths per 100,000 people are important factors to consider when determining the most effective preventive measures. 6
Fresh insights into susceptibility to endocarditis have emerged across various clinical contexts and demographic groups. Here, we address an unusual case of culture-negative IE following cataract surgery.
Case presentation
A 70-year-old man had recently undergone posterior chamber intraocular lens replacement surgery for a mature white cataract in the left eye. His medical history included hypertension, dyslipidemia, chronic kidney disease, and a transurethral prostate resection 14 years previously for benign prostatic hyperplasia. Following cataract surgery, he was prescribed prednisolone and ciprofloxacin eye drops.
Five days after surgery, the patient developed intermittent fever with chills, severe anorexia, generalized weakness, and mild exertional difficulty in breathing. A thorough assessment was conducted at a nearby medical facility over 8 days, but no definitive diagnosis was made. During this period, the patient received multiple courses of antibiotics. The fever initially subsided but recurred a few days later. There were no symptoms suggesting the involvement of other bodily systems. Additionally, there was no history of congenital heart disease, rheumatic fever, alcohol abuse, intravenous drug use, recent dental procedures, ongoing skin infections, tuberculosis contact, or recent travel. Fifteen days after the onset of fever (38.3°C), the patient was admitted to the medical unit because the fever was persisting despite treatment. Physical examination revealed pallor as the only significant finding. Chest auscultation detected normal vesicular breath sounds, and the cardiac examination revealed no murmurs or abnormal heart rhythms.
Initial blood tests revealed neutrophilic leukocytosis with elevated inflammatory markers and normocytic normochromic anemia. The blood picture suggested anemia of chronic disease and a bacterial infection. Apart from an elevated serum creatinine level, the patient’s urinalysis and liver function tests were normal. His laboratory investigations are summarized in Table 1.
Summary of the patient’s laboratory investigations.

ALP, alkaline phosphatase; ALT, alanine aminotransferase; ANA, antinuclear antibody; ANCA, antineutrophil cytoplasmic antibody; AST, aspartate aminotransferase; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HIV, human immunodeficiency virus; LDH, lactate dehydrogenase; MCV, mean corpuscular volume; MAT, microscopic agglutination test; SAg, surface antigen; WBC, white blood cells.
Aerobic and anaerobic blood and urine cultures were repeatedly negative. Electrocardiogram and chest radiographs were normal. Tests for HIV, hepatitis B and C, antinuclear antibody, rheumatoid factor, and antineutrophil cytoplasmic antibody were also negative. The Mantoux test for tuberculosis showed negative results. Tests for Plasmodium falciparum, P. vivax, P. ovale, P. malariae, melioidosis, Brucella, Legionella, Mycoplasma, and Leptospira were all negative. Fungal and anaerobic blood cultures yielded negative results as well. No abnormalities were detected in thyroid function tests or thyroid ultrasound scans.
Serum protein electrophoresis and lower gastrointestinal endoscopy revealed normal results. A high-resolution computed tomography scan showed chronic renal parenchymal changes and an atelectatic band in the right lung with thin bilateral pleural reactions. Although transthoracic two-dimensional echocardiography (TTE) appeared normal (Figure 1), transesophageal echocardiography (TEE) detected a 5-mm vegetation on the aortic valve (Figure 2), consistent with bacterial endocarditis, with an ejection fraction of >60%. The aortic valve function was normal. Based on the modified Duke criteria, 3 the diagnosis of “possible native aortic valve IE” was made, supported by echocardiographic findings (major criteria) and additional evidence, such as a fever of >38°C.
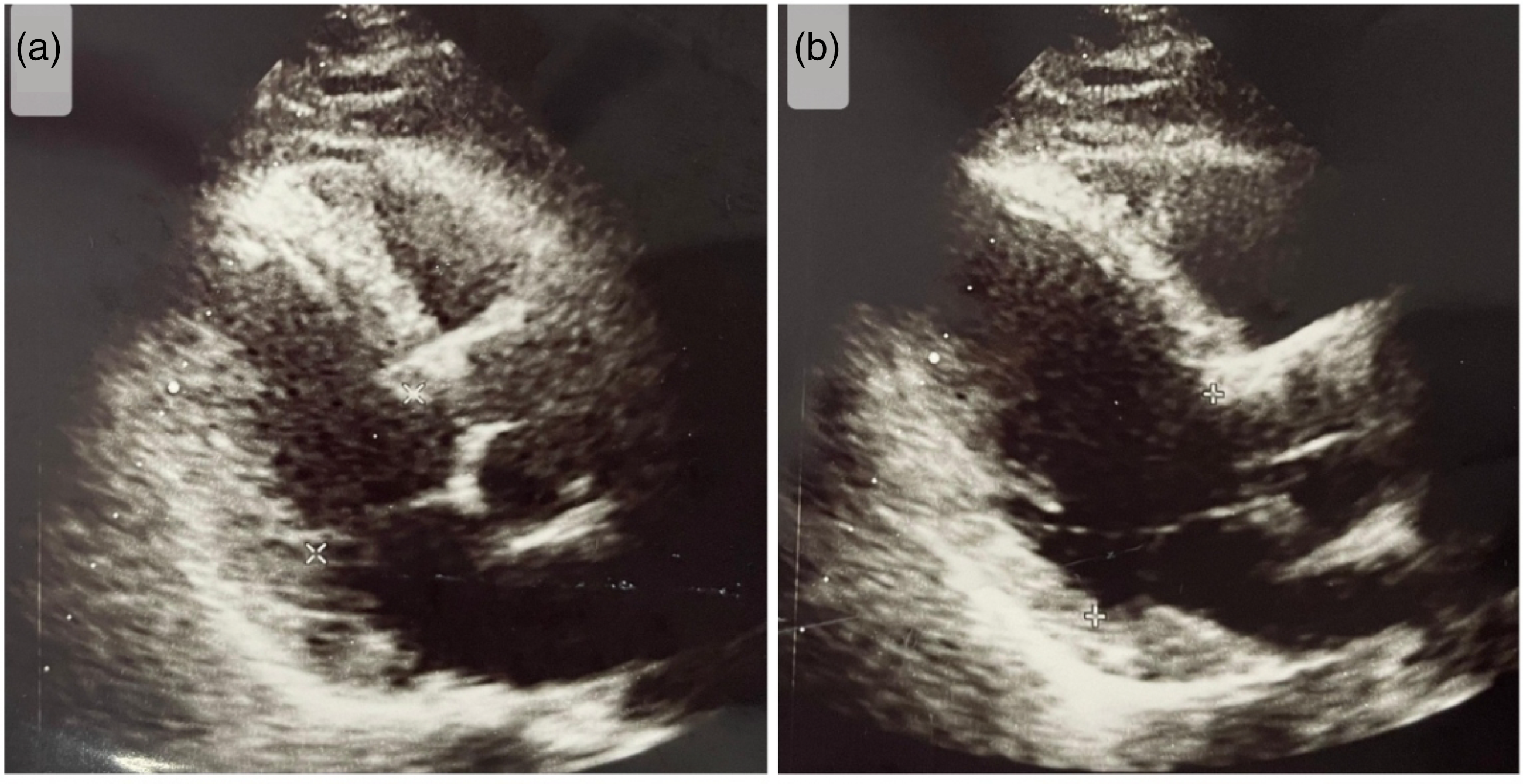
Transthoracic echocardiography images.

Transesophageal echocardiography images. The arrow indicates the vegetation on the aortic valve.
The patient was initially treated with meropenem. Significant improvement was observed after the addition of intravenous vancomycin, and the patient became afebrile within 7 days. After 10 days, meropenem was switched to intravenous ceftriaxone therapy. Vancomycin was continued for 28 days alongside intravenous ceftriaxone, with vancomycin levels closely monitored. Follow-up TEE revealed a resolving 4-mm vegetation. The patient was subsequently discharged on oral clindamycin (300 mg every 6 hours). The reporting of this study conforms to the CARE guidelines. 7
Discussion
A patient who had undergone cataract surgery developed a prolonged fever and nonspecific symptoms that persisted despite receiving multiple courses of antibiotics. He had no history of valvular disease or any predisposing condition for IE. It is highly likely that the bacteremia resulted from cataract surgery because no obvious signs of eye infection were detected during the postoperative period. Endophthalmitis is a rare complication of cataract surgery, affecting approximately 0.06% to 0.14% of adult patients, and can lead to bacteremia and endocarditis. 8 To our knowledge, this is the first reported case of IE in the native aortic valve resulting from bacteremia following cataract surgery. Despite the absence of predisposing heart conditions or established bacteremia, TEE was performed because of a high index of suspicion, even after normal TTE findings. Cataract surgery was the only recent event that could plausibly explain the bacteremia. In addition to the diagnostic challenges, the therapeutic approach was complicated by persistently negative blood cultures, likely due to prior antibiotic use. However, the patient responded well to empirical antibiotic therapy, achieving both biochemical and clinical recovery.
The diagnosis of prolonged intermittent fever is challenging. Approximately 2.9% of hospitalized adult patients are estimated to experience prolonged fever. 9 In adults, potential causes to consider in the differential diagnosis include infections, malignancies, non-infectious inflammatory responses, and other miscellaneous etiologies. 10 In developing countries, infections are the leading cause of prolonged fever, whereas non-infectious inflammatory diseases are more common in industrialized nations. In this case, the diagnosis of IE was made despite the absence of predisposing heart conditions or well-established bacteremia.
The ESC 2023 guidelines recommend TTE for patients suspected of having IE. 4 However, in this case, TTE did not reveal any abnormalities, underscoring the importance of TEE to confirm the diagnosis. TTE is less sensitive but more specific than TEE for assessing IE in native or prosthetic valves. 11 According to the ESC 2023 guidelines, TEE is particularly valuable in various clinical scenarios because TTE cannot detect perivalvular complications, small vegetations, prosthetic valve endocarditis, or vegetations associated with cardiovascular implantable electronic devices. TEE should be performed when TTE results are inconclusive or negative for vegetation. Repeat TTE and/or TEE is also recommended during follow-up of uncomplicated IE to monitor for developing complications.
Despite a normal TTE, a moderate-sized vegetation was detected on the TEE of our patient. IE of the aortic valve has a poorer prognosis than mitral valve endocarditis. This condition can be complicated by congestive heart failure, annular abscesses, and mycotic aneurysms affecting the sinus of Valsalva. These complications may lead to pericarditis, hemopericardium, cardiac tamponade, or fistulas extending into the heart. 10 Involvement of the conduction system can result in atrioventricular block. Septic embolization may affect organs such as the brain, liver, kidneys, and spleen. 10
Rheumatic heart disease remains a major risk factor for IE in developing countries. Most affected individuals are younger and acquire their condition from the community, with these infections typically caused by penicillin-sensitive streptococci. 1 In developed countries, degenerative valve disease, malignancy, intravenous drug use, diabetes mellitus, and congenital heart defects are the primary risk factors for IE. Most patients with these conditions are older, often exceeding 70 years of age. 12 The majority of IE cases are caused by Staphylococcus aureus (31%), followed by oral streptococci (17%) and coagulase-negative staphylococci (11%). 13 Cases caused by Enterococcus faecalis and coagulase-negative staphylococci are increasing, particularly among the elderly. 14 Positive blood cultures are crucial for diagnosing IE because they allow for the identification and testing of viable bacteria. It is recommended to collect three sets of blood cultures at 30-minute intervals, with each set containing 10 mL of blood, before initiating antibiotic therapy. Cultures should be incubated both aerobically and anaerobically. 15 Identifying causative microorganisms is most effective when no prior antimicrobial therapy has been administered. The 2023 ESC Guidelines for managing endocarditis provide comprehensive and detailed recommendations for antimicrobial therapy tailored to the specific causative pathogen. 4
Despite advancements in management, the in-hospital mortality rate of IE remains approximately 20%. 16 Factors contributing to increased mortality risk include advanced age; IE caused by pathogens such as Staphylococcus aureus, Pseudomonas aeruginosa, Enterobacteriaceae, or fungi; a significant burden of comorbidities (including end-stage renal disease requiring hemodialysis, prosthetic valve endocarditis, severe heart failure, stroke, abscess, and severe immunosuppression due to HIV infection); and the presence of perivalvular extension or a myocardial abscess. 16 The decision to perform surgery in cases of acute IE is typically guided by three primary factors: heart failure, uncontrolled infection, and the need to prevent septic embolization, particularly in the central nervous system. 4 Despite the associated risks, existing research indicates that surgical treatment may provide a survival benefit of approximately 20% within the first year.17,18 Therefore, early recognition and prompt management of IE are crucial to achieving the best clinical outcomes.
In our patient, the primary challenge was the persistent negativity of blood cultures. Blood culture-negative IE poses significant difficulties in both diagnosis and treatment, often resulting from prior antibiotic use. It can also be caused by fungal infections or certain fastidious bacteria, particularly obligate intracellular pathogens. Based on regional epidemiology, systematic serological testing is recommended for specific pathogens such as Coxiella burnetii, Bartonella spp., Aspergillus spp., Mycoplasma pneumoniae, Brucella spp., and Legionella pneumophila. 19 This should be followed by targeted polymerase chain reaction assays for Tropheryma whipplei, Bartonella spp., and fungal pathogens (Candida spp. and Aspergillus spp.) in both blood and tissue samples. 20 Pathological examination of resected tissue or embolic fragments using stains for bacteria, mycobacteria, fungi, and organism-specific immunohistochemical staining is essential for accurate diagnosis. Additionally, histopathological analysis can aid in diagnosing non-infectious endocarditis, including neoplastic and autoimmune causes. 21
In cases where all microbiological tests yield negative results and patients do not respond to antibiotics, the diagnosis of non-bacterial endocarditis should be considered. This rare disorder is characterized by the formation of sterile thrombotic vegetations on cardiac valves and is often associated with hypercoagulable states, such as malignancy, and chronic inflammatory conditions, including systemic lupus erythematosus, antiphospholipid syndrome, rheumatoid arthritis, and sepsis. 22 Testing for antinuclear antibodies, anticardiolipin antibodies (IgG), and anti-β2-glycoprotein 1 antibodies (IgG and IgM) should be performed if non-bacterial endocarditis is clinically suspected. In this case, the patient had already received parenteral and oral antibiotics before blood cultures were obtained, likely resulting in negative culture findings.
Conclusions
It is crucial to evaluate individuals with prolonged fever of unknown origin for IE. Effective management of this condition requires the administration of timely and appropriate antibiotics, guided by the severity of symptoms and culture results. In cases where blood cultures are negative, it is essential to exclude infections caused by fastidious organisms and fungi. However, in Sri Lanka, the most common cause of culture-negative endocarditis remains prior antibiotic therapy. Additionally, non-bacterial thrombotic endocarditis should be considered and ruled out if clinically indicated. Empirical antibiotic therapy played a pivotal role in this case. We have herein reported a unique instance of bacterial IE affecting the native aortic valve, which developed after cataract surgery and was successfully treated with empirical antibiotics.
Footnotes
Author contributions
GKJ, an internal medicine trainee, was involved in the management of the patient and drafted the manuscript. IJ, the primary consultant under whom the patient was admitted, played a key role in the patient's management at all stages alongside GKJ and provided supervision and guidance for writing and reviewing the manuscript. LD, an internal medicine trainee, contributed to the patient's management. USP, a trainee in anesthesia and critical care medicine, was also involved in the patient's management. Both LD and USP reviewed the manuscript.
Consent
Written informed consent was obtained from the patient for treatment as well as for the publication of the case report.
Data availability statement
Not applicable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
This manuscript describes a case report. According to the policies of our institution, ethics review committee approval is not required for the publication of case reports.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.